
Prevalence of iron deficiency in patients aged 75 years or older with heart failure
2018-12-11 12:24:24PaulMiniBonnefoyMarcSubtilFabienMichelChuzeville
Journal of Geriatric Cardiology 2018年11期
Paul Mini, Bonnefoy Marc, Subtil Fabien, Michel Chuzeville
1Geriatric Cardiology Department, Edouard Herriot Hospital, Hospices Civils de Lyon, Lyon, France
2Geriatric Department, Lyon South Hospital, Hospices Civils de Lyon, Lyon, France
3Biostatistics Health Department, University Claude Bernard Lyon 1, Hospices Civils de Lyon, Lyon, France
4Geriatric Cardiology Department, Edouard Herriot Hospital, Hospices Civils de Lyon, Lyon, France
Abstract Background The latest studies presented at the American Heart Association (AHA) meeting on heart failure and the update of the European Cardiology Society’s (ECS) recommendations on heart failure in 2016 recommend intravenous iron supplementation in patients with heart failure, reduced ejection fraction and iron deficiency for improves walking performance and quality of life, and reduces morbidity.In the present study, we investigated the prevalence of iron deficiency in heart failure patients aged 75 years or older, as there is currently no data on these patients. Methods We performed an observational study on hospitalized patients in Geriatric Cardiology Department. Among the 462 patients hospitalized during eight months, 176 were eligible for inclusion; 22 patients was significant interference with an inflammatory syndrome (high ferritin with high C-reactive protein), and for 13 patients iron-related data were not available. For each patient included,a complete iron assessment and type of heart failure was available. Results A total of 141 patients were included, the mean age was 88 years (range: 75–101), and there were 52 (36.9%) of patients with reduced ejection fraction (EF), 37 (26.2%) with mid-range EF, and 52(36.9%) with preserved EF. Irrespective of heart failure type, 73.8% had iron deficiency (95% CI: 65.7%–80.8%); this was found in 57.7%(95% CI: 43.2%–71.3%) of those with reduced EF, 78.4% (95% CI: 61.8%–90.2%) of those with mid-range EF, and 86.5% (95% CI:74.2%–94.4%) of those with preserved EF (P = 0.003). Conclusion The prevalence of iron deficiency was very high in very elderly patients with heart failure, especially those with HF with mid-range EF or HF with preserved EF.
Keywords: Heart failure; Iron deficiency; Very elderly patient
1 Introduction
The increasing incidence and prevalence of heart failure(HF) and the associated medical, social, and economic consequences has led this to become a public health problem.Despite advances in HF management, morbidity and mortality remain significant cardiovascular and non-cardiovascular comorbidities often have a deleterious impact on the clinical condition, symptoms, and progression of HF.[1]
Owing to longer life expectancy, greater control of cardiovascular risk factors, and improved management of cardiac diseases, such as ischemic or valvular heart disease, the age of HF onset has increased and therefore the incidence and prevalence of HF has increased in elderly people, particularly those over 65 years of age.[2]This age group is,however, underrepresented in large prospective studies concerning the treatment of HF. Furthermore, the latest classification of heart failure by the European Society of Cardiology (ESC) retains three types of HF, defined primarily by left ventricular ejection fraction (EF); HF with reduced EF (HFrEF), HF with mid-range EF (HFmrEF), and HF with preserved EF (HFpEF),[3]yet there is little reported data for the latter two as they are often excluded from studies because the underlying physiopathological and etiological mechanisms are still not well understood. Although existing treatments for HFrEF have not demonstrated their efficacy on the mortality of HmrEF and HFpEF, they are of importance as they represent more than 50% of new HF diagnoses.[4–6]
Recently, iron deficiency has been recognized as an independent marker of poor prognosis in HFrEF. The 2013 American Heart Association (AHA) recommendations do not provide guidelines for iron, but the 2016 European guidelines[3]are more clearly positioned; based on the FAIR-HF[7]and CONFIRM-HF[8]studies, these propose to consider intravenous iron carboxymaltose in symptomatic patients with HFrEF and iron deficiency defined by a ferritin <100 μg/L or ferritin between 100-299 μg/L associated with saturation of transferrin < 20%. This treatment decreases HF symptoms, increases exercise capacity, and improves quality of life. A grade IIa is brought to this recommendation, with a degree of evidence rated A.
In this context, we therefore conducted a study to estimate the prevalence of iron deficiency in HF patients aged 75 years or more, irrespective of HF type, with subgroup analysis according to the type of HF and sought predisposing risk factor. There are no data concerning patients aged 75 years or older with HFmrEF or HFpEF.
2 Method
2.1 Selection of participants
All patients aged 75 years or older admitted to the geriatric cardiology department of the Lyon teaching hospitals with previous history HF (any type) between January 1 and August 31, 2017 were included; those who had had iron supplementation in the previous six months were excluded.All patients were informed of the purpose of this study and non-opposition to the use of their biological data was collected (in accordance with the laws in place at the time of the study written consent was not required).
Among the 462 patients identified, 176 were eligible; 22 patients there was significant interference with an inflammatory syndrome defines by High ferritin with high C-reactive protein, and for 13patients iron-related data were not available.
For each patient included, a complete iron assessment and type of heart failure was available, and for 13 patients iron-related data were not available. A total 141 patients were included.
2.2 Technical information
For each patient, venous blood samples were obtained and hemoglobin, ferritin, transferrin saturation factor, creatinine, and C-reactive protein (CRP) were analyzed. Iron deficiency was defined according to the international recommendations adopted by the ESC; ferritin < 100 μg/L or ferritin between 100-299 μg/L associated with saturation of transferrin < 20%. For all the patients included in this study,a brain natriuretic peptide (BNP) assay and a transthoracic ultrasound were available to classify the type of heart failure according to the definition of the ESC: HFrEF is defined by clinical symptoms and LVEF < 40%; HFmrEF by clinical symptoms, a left ventricular ejection fraction (LVEF) between 40%–49%, and BNP > 35 ng/L; HFpEF by clinical symptoms, LVEF > 50%, and BNP > 35 ng/L. The nutritional status was assessed on body mass index (BMI). For a BMI less than 16.5 kg/cm2, we talk about undernutrition, between 16.5 and 18.5 kg/cm2, leanness; between 18.5 and 25 kg/cm2, normal; between 25 and 30 kg/cm2, overweight;and over 30 kg/cm2, obesity. Renal function was evaluated according to the Kidney Disease Improving Global Outcomes (KDIGO) classification: moderate renal insufficiency was defined as glomerular filtration rate (GFR) between 60-30 mL/min per 1.73 m2, severe renal insufficiency by GFR between 15–29 ml/min per 1.73 m2, and terminal GFR< 15 mL/min per 1.73 m2.
2.3 Statistics
The Chi-square test or Fisher’s exact test was used for comparisons of categorical variables, as appropriate. Multivariate logistic regression analysis was used to evaluate predictors for iron deficiency. A value of P < 0.05 was considered statistically significant.
3 Results
Among the 462 patients identified, 176 were eligible;there was significant interference with an inflammatory syndrome in 22 patients; and for 13 patients iron-related data were not available. A total of 141 patients were included.
The mean age of patients was 88 years and the majority were women (56%). Nutritional status was normal for 47.5%; 12.2% were undernourished and 18.4% were obese.The number of hospitalizations was > 3 for 17% of patients,and the reason for hospitalization was cardiac decompensation for the majority (70.2%) of those included. Just over quarter (26.2%) had HFmrEF, 36.9% had HFpEF, and 36.9% HFrEF; 51.1% had moderate renal insufficiency and 15.6% severe renal insufficiency, and 68.8% had anemia(Table 1). For the prevalence of iron deficiency was 73.8%(95% CI: 65.7%–80.8%), irrespective of HF type.
Women had significantly more frequently iron deficiency(82.3%, 95% CI: 72.1%–90.0%) than men (62.9%, 95% CI:49.7%–74.8%; P = 0.016). Iron deficiency was significantly different between categories of nutritional status (P = 0.028);those classified as overweight least frequently had iron deficiency (58.1%, 95% CI: 39.1%–75.5%), and those classified as obese most frequently had iron deficiency (92.3%, 95%CI: 74.9%–99.1%). It also differed significantly according to type of HF (P = 0.003); patients with HFmrEF and HFpE were the most often iron deficient (78.4%, 95% CI: 61.8%–90.2% and 86.5%, 95% CI: 74.2%–94.4%, respectively;Table 2).

Table 1. Characteristics of patients (n = 141).
In univariate analysis, the factors significantly associated with iron deficiency were sex and HF type (Table 3). In multivariate analysis, female sex was significantly associated with iron deficiency (OR: 2.4; 95% CI: 1–5.5). At comparable sex, HFmrEF have a 3 OR, 95% CI: 1.1–8.1, P= 0.028, risk than HFrEF; HFpEF have a 3.8 OR, 95% CI:1.4–10.3, P = 0.009, risk than HFrEF (Table 4).
4 Discussion
The present study found that the prevalence of iron deficiency was very high among very elderly patients with HF,in particular in those with HFmrEF or HFpEF. In this study,more than half of the patients presented HFpEF or HFmrEF,reflecting an evolution of types of HF with an increase types HFpEF and HFmrEF and decrease type HFrEF.
All studies of iron supplementation are of excellent methodology and have led to the drafting of new ESC recommendations. However, all of these studies focused on HFrEF; in the absence of studies showing the same results in HFmrEF and HFpEF, it is difficult to recommend iron supplementation for such patients because the effects of ferric supplementation have not been demonstrated. It should be noted that all the effects noted by the iron supplementation, is noted only for intra-venous supplementation.[9,10]
As expected, the prevalence of iron deficiency was higher in anemic patients; however, it is interesting to look at the prevalence of patients without anemia, it was, in our study, 70.5%. Indeed, in our clinical practice, the prescription of iron balance is often motivated by anemia. This can question us about the relevance of a systematic iron assessment in HFrEF.
It should be noted that all the patients recruited in this study were hospitalized in the geriatric cardiology department of the Lyon teaching hospitals which may have led to selection bias and overrepresentation of iron deficiency as compared to the general HF population. Patients hospitalized in this department are often complex and advanced cases requiring specific care, and therefore the study should be extended to at least the geriatric services of the Lyon teaching hospitals to provide more generalizable results.
The mean age was 88 years, and it is interesting to note that, compared with existing data, the prevalence of iron deficiency in HF seems to increase exponentially with age;it is reported to be 50% at 64 years of age, 61.3% at 65.3 years, and 73.2% at 88 years.[11–13]In this study, 88% of patients over 95 years of age were iron deficient. In this study, the female sex is an important risk factor for developing iron deficiency in HF, it might be interesting to explore this fact to understand why women are more deficient in iron while they are menauaus.
The nutritional status seems interesting to explore. In all available prevalence studies, the BMI of individuals was relatively standardized. In the present study, recruitment was more heterogeneous, the subgroup analysis was very interesting because the prevalence was very important in the subjects obese versus undernourished individuals. TheseHFmrEF: heart failure with mid-range ejection fraction; HFpEF: heart failure with preserved ejection fraction; HFrEF: heart failure with reduced ejection fraction.results are to be interpreted with caution due to the small size of the study but could be a track for a future research project.
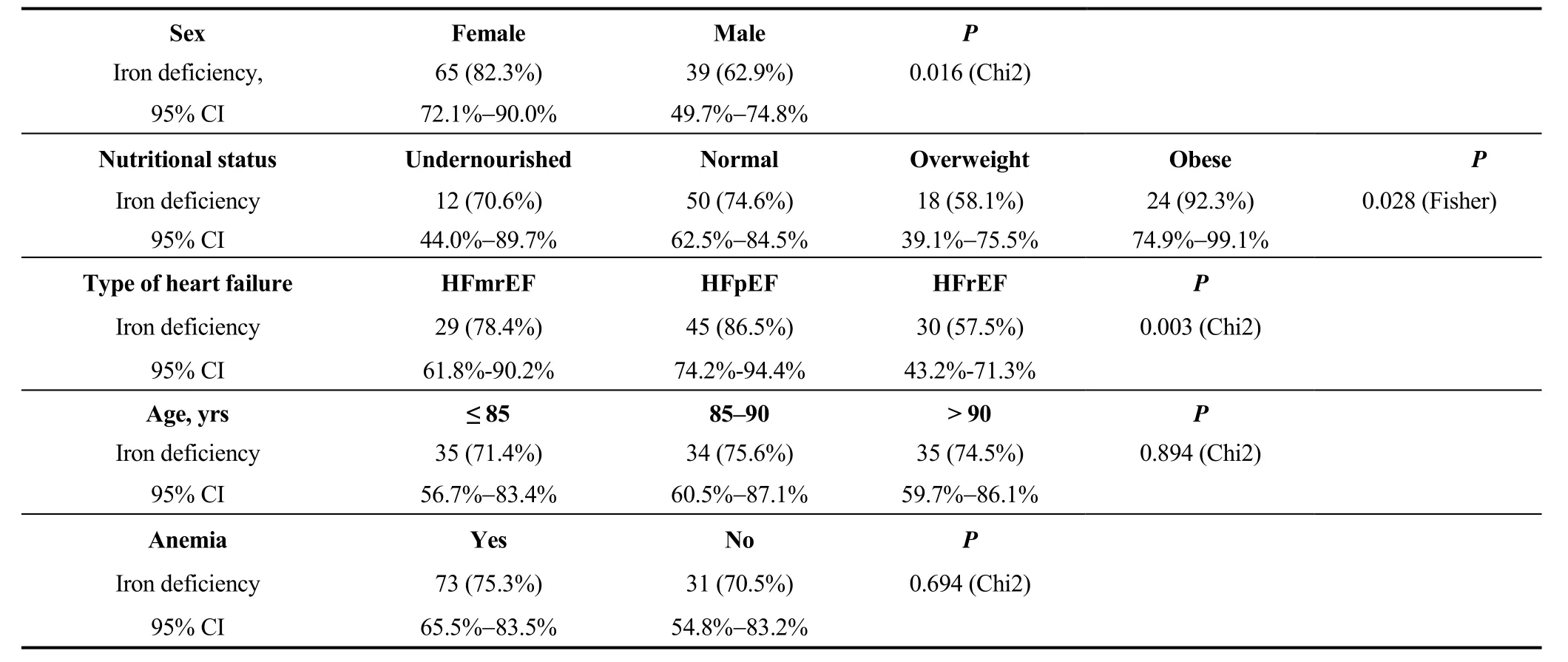
Table 2. Patient characteristics stratified according to iron deficiency (n = 104).
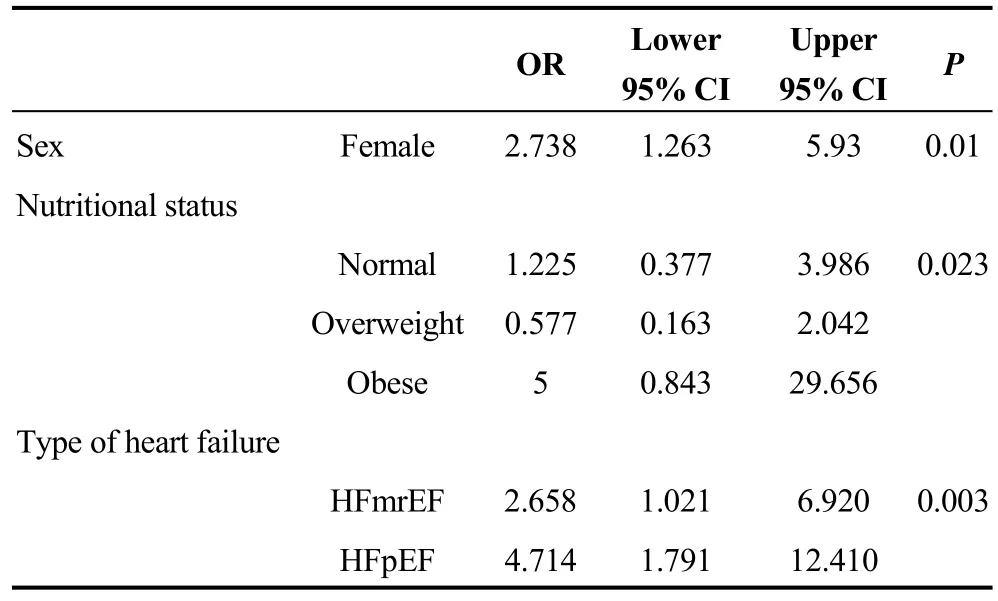
Table 3. Factors associated with iron deficiency, univariate analysis.
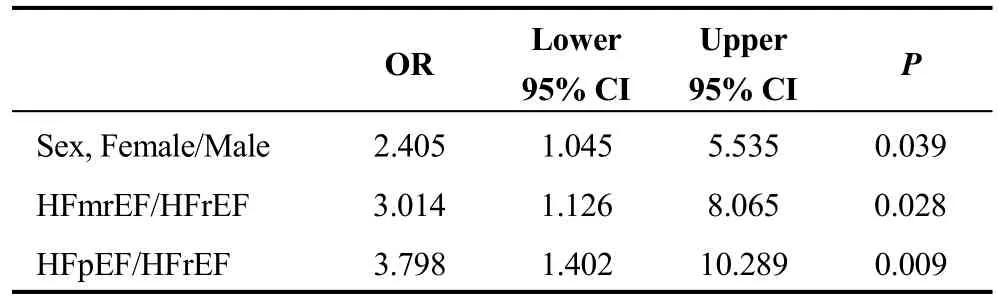
Table 4. Risk of iron deficiency quantified by odds ratio,multivariate analyzes.
For the future, the systematic consideration and correction of the ferric status in heart failure patients, particularly the elderly, could become, in the coming years, an important element in the management.
Acknowledgments
This work was written in collaboration with the geriatric cardiology of the Hospices Civils de Lyon, France. Statistical analysis was performed by the Biostatistics Department of the Hospices Civils de Lyon and the Faculty of Medicine Claude Bernard Lyon 1, Lyon, France.
 Journal of Geriatric Cardiology2018年11期
Journal of Geriatric Cardiology2018年11期
- Journal of Geriatric Cardiology的其它文章
- Atypical electrocardiographic manifestations of ischemia: a case of dynamic Wellens patterns
- Inoperable severe aortic valve stenosis in geriatric patients: treatment options and mortality rates
- Chemical renal artery denervation with appropriate phenol in spontaneously hypertensive rats
- Increased index of microcirculatory resistance in older patients with heart failure with preserved ejection fraction
- Frailty significantly impairs the short term prognosis in elderly patients with heart failure
- Association of invasive treatment and lower mortality of patients ≥ 80 years with acute myocardial infarction: a propensity-matched analysis