
Normalization of plasma growth hormone alleviated malignant ventricular tachycardia in acromegaly
2018-10-15 04:03:20ZhiHaoLIUKangLIYanShengDINGJianXingQIUStevenSiyaoMengMohetaboerMominShengCongLIUTieCiYIJianPingLI
Journal of Geriatric Cardiology 2018年8期
Zhi-Hao LIU, Kang LI, Yan-Sheng DING, Jian-Xing QIU, Steven Siyao Meng, Mohetaboer Momin, Sheng-Cong LIU, Tie-Ci YI, Jian-Ping LI, 3,*
?
Normalization of plasma growth hormone alleviated malignant ventricular tachycardia in acromegaly
Zhi-Hao LIU1, Kang LI1, Yan-Sheng DING1, Jian-Xing QIU1, Steven Siyao Meng2, Mohetaboer Momin1, Sheng-Cong LIU1, Tie-Ci YI1, Jian-Ping LI1, 3,*
1Department of Cardiology, Peking University First Hospital, Beijing,China2University of Rochester Medical Center, Rochester, NY,United States3Key Laboratory of Molecular Cardiovascular Sciences of Ministry of Education,Health Science Center, Peking University, Beijing, China
J Geriatr Cardiol 2018; 15: 547?550. doi:10.11909/j.issn.1671-5411.2018.08.003
Acromegaly;Growth hormone; IGF-1; Ventricular tachycardia
Acromegaly is an insidious endocrine disease characterized by chronic elevation of growth hormone (GH) and insulin-like growth factor-1 (IGF-1).[1]Persistent excess secretion of GH and IGF-1 damages both cardiac structure and function, leading to acromegalic cardiomyopathy, which is one of the most common causes of increased mortality in acromegaly and can result in an average of 10-year reduction in life expectancy.[2,3]In patients with acromegaly, approximately 3% have been reported having a unique cardiomyopathy characterized by biventricular hypertrophy, myocardial necrosis, lymphocytic infiltration, interstitial fibrosis.[4]The manifestations of acromegalic cardiomyopathy include systolic or diastolic cardiac dysfunction as well as fatal arrhythmias.[5,6]This case report focuses on ventricular tachycardia (VT) in a patient with acromegaly. After normalization of plasma GH levels with therapy, ventricular tachycardia was resolved.
A 59-year-old man was hospitalized after several episodes of transient amaurosis and palpitation for two weeks. Electrocardiograph revealed ventricular tachycardia with a maximum heart rate of over 200 bpm during the episode of palpitation (Figure 1). He had taken amiodarone (600 mg/d) and metoprolol (47.5 mg/d) for half a month before being hospitalized.
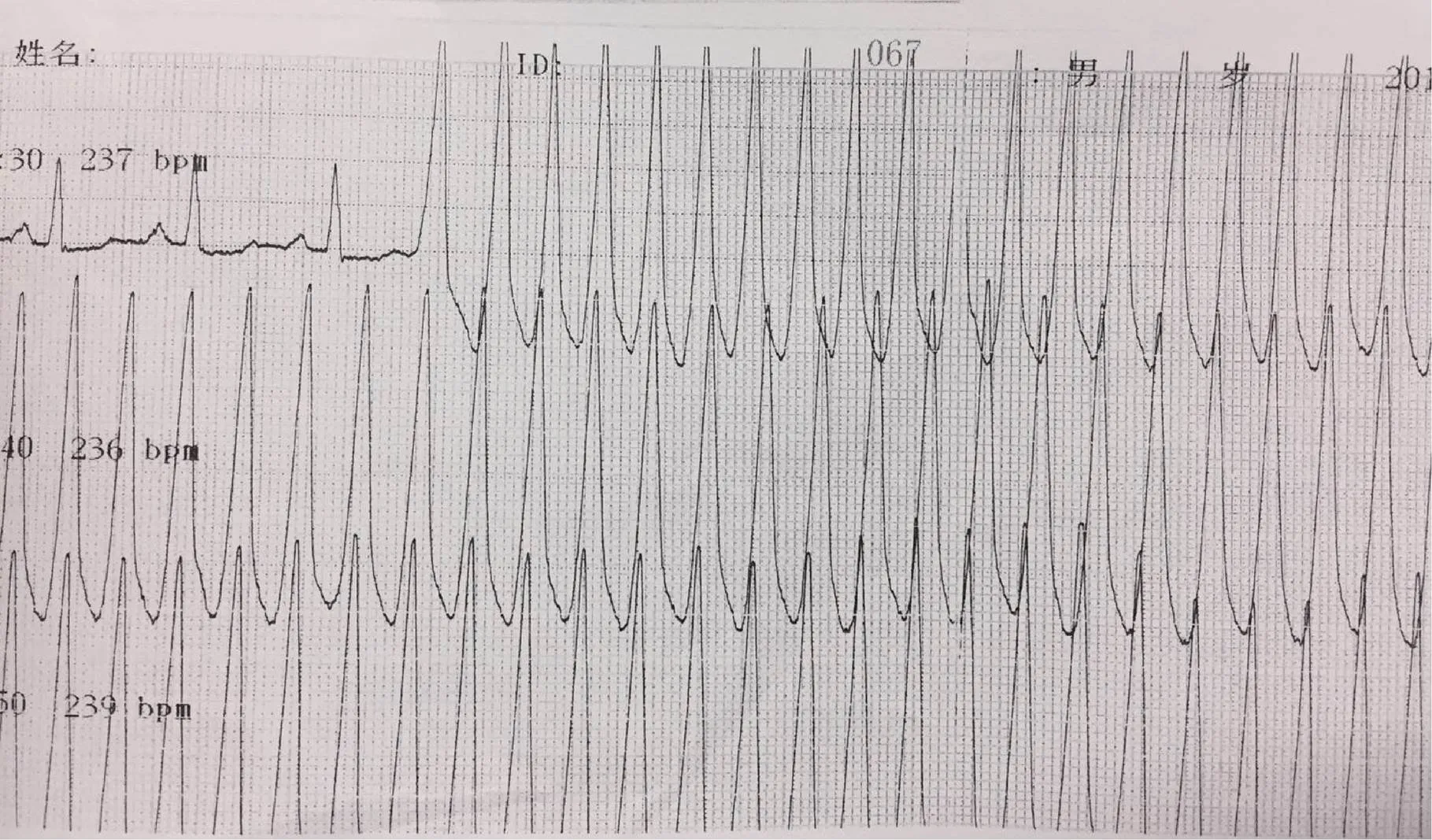
Figure 1. Surface lead 2 electrocardiogram in emergence room showed sustained ventricular tachycardia.
At first sight of his characteristically enlarged jaw, and the enlarged, swollen hands and feet (Figure 2), a diagnosis of acromegaly was suspected. Laboratory tests showed remarkably elevated levels of plasma GH and IGF-1 of 14.3 ng/mL (normal range: 0.03–2.47 ng/mL) and 863 ng/mL (normal range: 81–238 ng/mL), respectively. Pituitary magnetic resonance imaging (MRI) revealed a pituitary adenoma (Figure 3). Other associated manifestations of acromegaly were also found in this patient, such as diabetes mellitus, enlarged organs, obstructive sleep apnea and hypertension. Therefore, the patient was diagnosed with acromegaly. Subsequently, we performed several examina- tions to evaluate whether the heart was affected. Ultrasonic cardiogram indicated (1) symmetric thickening of the left ventricular wall, (2) enlarged left atrium and left ventricle, and (3) marginal decreased left ventricle ejection fraction (49.7%). Cardiac MRI showed similar information with UCG and found focal fibrosis of left ventricular apex and interventricular septum. Holter monitoring showed multiple polymorphic ventricular premature contractions (13033 beats/24h) and non-sustained ventricular tachycardia. Electrophysiological examination failed to induce ventricular tachycardia (one possible hypothesis is the protective influence of amiodarone). We recommended a subsequent cardiac biopsy, but the patient refused.

Figure 2. Characteristic appearance of patients with acromegaly: increased head circumference, enlarged jaw, swollen soft tissues of heads, thicken lips,.
Figure 3. Pituitary adenoma (red arrows) found from cerebral magnetic resonance image.
We suspected ventricular tachycardia was associated with acromegaly in this patient. Under intensive monitoring with an automated external defibrillator, a neurosurgeon performed the transsphenoidal surgical resection of pituitary adenoma for him. Seven days after surgery, plasma GH of the patient decreased dramatically from 12.35 ng/mL to 2.66 ng/mL. The patient stopped taking anti-arrhythmia drugs due to nocturnal bradycardia. At one year postoperative follow-up, the plasma GH was normal and plasma IGF-1 decreased to a marginal normal level (242 ng/mL). Surprisingly, the patient had no more episodes of syncope or amaurosis. Sustained and non-sustained ventricular tachycardia could not be observed on holter monitoring. Furthermore, the frequency of premature ventricular contractions also decreased dramatically (Table 1). Cardiac MRI showed left ventricular wall thickness and left ventricle end diastolic diameter reverted to an acceptable range but the focal fibrosis remained unchanged.
Acromegalic cardiomyopathy is an important complication of acromegaly.[11]Due to the lack of specific cardiac manifestations, if acromegaly is not diagnosed, acromegalic cardiomyopathy cannot easily be differentiated from other cardiomyopathies. Thus ventricular tachycardia in acromegaly patients is commonly misdiagnosed as idiopathic ventricular tachycardia or ventricular tachycardia secondary to dilated cardiomyopathy or hypertrophic cardiomyopathy. As a result, physicians will prescribe anti-arrhythmia drugs or implantable cardioverter defibrillator (ICD) implantation for the patient instead of treating the underlying acromegaly. The absence of anti-growth hormone therapy results in further cardiac damage, so cardiac arrhythmias persist.
We searched Pubmed with the key words ‘ventricular tachycardia’ and ‘a(chǎn)cromegaly’. Only 4 case reports were found describing acromegalic ventricular tachycardia. We summarized the features of these cases in Table 2.[7–10]All the cases were middle-aged males. It is not clear if males are more easily affected or if there is a sex-based mechanism for acromegalic cardiomyopathies. After anti-growth hormone therapy, most reported patients recovered from cardiac dysfunction and ventricular tachycardia.[7–9]But in one patient, syncopal ventricular tachycardia recurred 5 years after receiving transsphenoidal surgery and subsequent normalization of his plasma GH levels.[10]ICD was implanted in this patient to treat his ventricular tachycardia. Another patient also received ICD for severe heart failure. So ICD is not necessary in every patient with acromegalic cardiomyopathy. According to the most updated guidelines, ICD is recommended in patients with irreversible, non- ischemic cardiomyopathy (Class IA).[12]Obviously, acromegalic cardiomyopathy is a reversible disease. So, when we make the decision on ICD implantation, several issues need to be taken into consideration, including cardiac function, recurrence of fatal ventricular tachycardia, and severity of fibrosis. Previous studies indicate that infiltration of inflammatory cells and hypertrophy of cardiomyocytes resolve, while interstitial fibrosis remain unchanged after anti-growth hormone treatment, which may account for the reason why fatal arrhythmias still recur in some cases.[13,14]So fibrosis could provide an important information in clinical decision-making. In the reported cases, cardiac MRI had never been used in the diagnosis of acromegalic cardiomyopathy. In our case, cardiac MRI not only detect the hypertorphy of the ventricle, but also revealed the cardiac fibrosis.

Table 1. Follow-up databases of the patient.
BNP: brain natriuretic peptide; BP: blood pressure; cTNI: cardiac troponin I; FG: fasting glucose; GH: growth hormone; HbA1c: glycated hemoglobin; IGF-1: insulin-like growth factor-1; PVC: premature ventricualr contraction; VT: ventricular tachycardia.
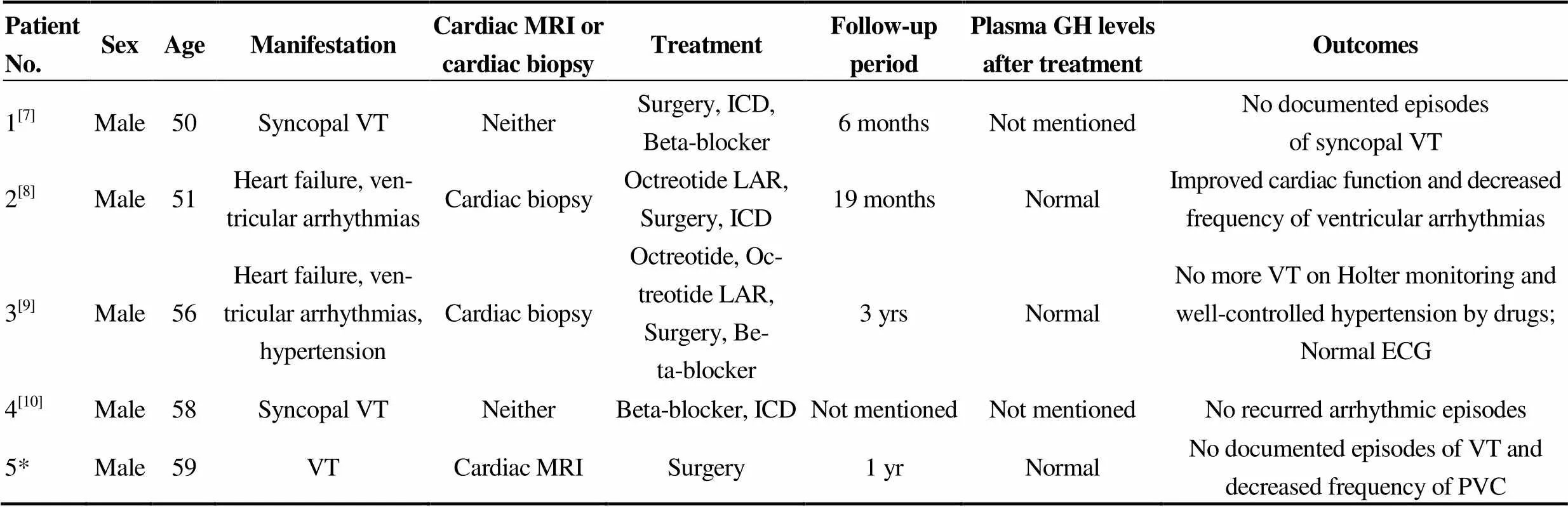
Table 2. Summery of reported cases.
ECG: electrocardiograph; GH: growth hormone; ICD: implantable cardioverter defibrillator; LAR, long-acting release; MRI: magnetic resonance imaging; PVC: premature ventricualr contraction; VT: ventricular tachycardia. *Our patient.
In summary, we herein report a case of acromegaly with recurrent malignant ventricular tachycardia. We emphasize the importance of recognizing and diagnosing the underlying disease when we are treating patients with arrhythmias, as the arrhythmia could be cured without taking anti-arry-thmia drug, or implementation of ICD. Since such case of ventricular tachycardia associated with acromegaly are extremely rare, we need to review more cases in order to formulate effective treatment plans for these patients.
1 Frara S, Maffezzoni F, Mazziotti G,The modern criteria for medical management of acromegaly.2016; 138: 63–83.
2 Maffei P, Martini C, Mioni R,The cardiac complications of acromegaly.2003; 26: 20–27.
3 Melmed S. Acromegaly pathogenesis and treatment.2009; 119: 3189–3202.
4 Matta MP, Caron P. Acromegalic cardiomyopathy: a review of the literature.2003; 6:203–207.
5 Sharma MD, Nguyen AV, Brown S,Cardiovascular disease in acromegaly.2017; 13: 64–67.
6 Rodrigues EA, Caruana MP, Lahiri A,Subclinical cardiac dysfunction in acromegaly: evidencefor a specific disease of heart muscle.1989; 62:185–194.
7 An Z, He YQ, Liu GH,Malignant ventricular tachycardia in acromegaly: a case report.2015; 133: 55–59.
8 Yokota F, Arima H, Hirano M,Normalisation of plasma growth hormone levels improvedcardiac dysfunction due to acromegalic cardiomyopathy with severe fibrosis.2010;2010.
9 Kitamura T, Otsuki M, Yamaoka M,The temporary drop of serum octreotide concentration deteriorated ventricular tachycardia in an acromegalic patient.2013; 60: 1165–1169.
10 Arias MA, Pachón M, Rodríguez-Padial L,Ventricular tachycardia in acromegaly.2011; 30: 223–226.
11 Colao A, Ferone D, Marzullo P,Systemic complications of acromegaly: epidemiology, pathogenesis, and management.2004; 25: 102–152.
12 Al-Khatib SM, Stevenson WG, Ackerman MJ,2017 AHA/ACC/HRS Guideline forManagement of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society.2017; 2017: e39–e110.
13 Nishiki M, Murakami Y, Sohmiya M,Histopathological improvement of acromegalic cardiomyopathy by intermittent subcutaneous infusion of octreotide.1997; 44: 655–660.
14 Legrand V, Beckers A, Pham VT,Dramatic improvement of severe dilated cardiomyopathy in an acromegalic patient after treatment with octreotide and trans-sphenoidal surgery.1994; 15: 1286–1289.
Correspondence to: 13521531013@163.com
 Journal of Geriatric Cardiology2018年8期
Journal of Geriatric Cardiology2018年8期
- Journal of Geriatric Cardiology的其它文章
- Rare combination of dilated cardiomyopathy and ankylosing spondylitis in a family
- Patent foramen ovale in an old patient with ischemic stroke following carotid surgery
- Natriuretic peptide family as diagnostic/prognostic biomarker and treatment modality in management of adult and geriatric patients with heart failure: remaining issues and challenges
- Subclinical hypothyroidism is associated with lipid-rich plaques in patients with coronary artery disease as assessed by optical coherence tomography
- Five-year major clinical outcomes between first-generation and second- generation drug-eluting stents in acute myocardial infarction patients underwent percutaneous coronary intervention
- Correction of hypovitaminosis D improved global longitudinal strain earlier than left ventricular ejection fraction in cardiovascular older adults after orthopaedic surgery