
Evaluation of cardiac autonomic status using QTc interval in patients with leprosy
2016-04-09 08:53:50JayeshSolankiAmeeThesiaHitaMehtaChinmayShahHemantMehta
Jayesh D. Solanki, Amee M. Thesia, Hita H. Mehta, Chinmay J. Shah Hemant B. Mehta
1 Department of Physiology, Government Medical College, Bhavnagar, Gujarat, India
2 Third Year MBBS Student, Government Medical College, Bhavnagar, Gujarat, India
3 Department of Skin and VD, Government Medical College, Bhavnagar, Gujarat, India
INTRODUCTION
Leprosy has been shown to affect almost all the systems of human body and leads to an abnormality of function of the autonomic nerves innervating various parts (Suzuki et al., 2012). Leprosy is the most common neuromuscular disease (Nations et al., 1990) and leprosy patients in India account for over half of the world’s leprosy cases (Singal and Sonthalia, 2013). There is no leprosy patient without involvement of the peripheral nervous system (Cabalar et al., 2014). Yet, every year, thousands of patients develop permanent peripheral nerve damage owing to leprosy but autonomic involvements are not counted in the history sheet of leprosy patients (Jacob and Franco-Paredes, 2008). Neuropathies, including motor, sensory or autonomic function alterations, are the hallmark of leprosy (Freeman, 2005).Neuropathy studies mainly focus on sensory or motor dysfunctions (Leprosy Neuropathy-Medscape Reference,2015), but few neuropathy studies are reported on cardiac autonomic neuropathy (Charosky et al., 1983; Mora-Brambila et al., 2006; Cabalar et al., 2014). Dispersion of ventricular depolarization is reportedly increased in leprosy patients owing to invasion of cardiac autonomic nerves(Kale et al., 1984; Ulvi et al., 1996). There is a decreasing area of interest in leprosy because of its decreased global prevalence and incidence. Cardiac autonomic neuropathy can lead to repolarization abnormality (Zhao et al., 2010),which if left unaddressed can progress to life-threatening arrhythmia (Stevens et al., 2013), finally resulting in sudden cardiac death. This can be diagnosed by QTc (QT corrected for heart rate) interval, a simple, objective, validated tool based on simple electrocardiogram (ECG) using Bazett’s formula (Bazett, 1920). To the best of our knowledge, there are few studies on the prevalence of cardiac autonomic neuropathy in leprosy patients in our region. In this study,we evaluated cardiac autonomic status using QTc interval in patients with leprosy and investigated the correlates.
SUBJECTS AND METHODS
Subjects
A cross-sectional case-control study was performed at Leprosy Clinic, Department of Dermatology, Government Medical College Hospital, Indian using a simple ECG machine (BPL Company, Kolkata, West Bengal, India,model CARDIART 108T DG). Thirty patients with leprosy were recruited from Leprosy Clinic, Department of Dermatology, Government Medical College Hospital, Indian.These patients underwent an initial assessment including demographic data, history of disease and medication, bacteriological picture, skin features and neuropathy pro file.Thirty age- and sex-matched healthy controls who visited the general outdoor patient departments of the same hospital for either physical fitness or minor ailments were also included in this study.
Inclusion criteria
Potential participants were screened against the following criteria:
· Taking regular treatment like outdoor patients
· Age of 15-70 years and of either sex
· Absence of lepra reaction during the study
· Having ability to walk with no major malformations
· Provision of written informed consent
Exclusion criteria
Patients presenting with one of the following were excluded:
· Taking irregular treatment
· Taking drugs that prolong QTc interval (Kilborn and Woosley, 2001)
· Taking drugs that affect autonomic nervous system
· Having type 2 diabetes mellitus, cardiovascular disorder, renal failure, cancer, acquired immune de ficiency syndrome, tuberculosis, or cardiac arrhythmia
· Having a pacemaker implanted
· Refusal of informed consent
Potential healthy controls were also screened against the above inclusion and exclusion criteria for recruitment of patients except absence of leprosy or any other disease.Prior permission from concerned departments was followed by approval of institutional review board of Government Medical College, Indian. Written informed consent regarding participation of this trial and the objective of this study was obtained from each participant.
Measurements
After general data collection and medical history evaluation,cardiac risk assessment was performed using self-made pre-validated questionnaires. Symptoms of neuropathy were inquired and the leprosy patients were classi fied into paucibacillary and multibacillary by dermatologists as per WHO criteria (World Health Organization Expert Committee on Leprosy,1988).
QTc measurement: A standard 12-lead ECG (ECG Machine, BPL-Model: 108T DIGI, Hi-Tech Equipments, Inc.Kolkata, West Bengal, India) was recorded. Precisely, subjects were asked to lie in the supine position and ECG lead II with minimum 10 waveform complexes was recorded.QT interval and RR interval were measured manually from the ECG strip for 10 successive readings. QT interval was measured using tangent method (Lanjewar et al., 2004). RR interval was measured from one R-wave peak to another R-wave peak. QTc intervals were derived using Bazett’s formula and the average across 10 results was taken as QTc value for each subject. Two cases were discarded since lead II had artefact or shallow T wave as well as dif ficult measurement of the QT.
Bazett’s formula:
No correction was used, if heart rate was less than 60.
De fining norms: QTc interval value > 0.43 second in males and > 0.45 second in females was considered abnormal(Moss, 1999).
Sample size
Sample size was calculated by software RaoSoft (Raosoft,Inc. free online software, Seattle, WA, USA) for population of the district 25 lakhs with 0.73/10000 prevalence of leprosy in India. A size of 30 yielded 99.5 % con fidence level, keeping 0.5% margin of error.
Statistical analysis
The data were transferred on Excel spreadsheet, descriptive data was expressed as the mean ± standard deviation and categorical data as number. All calculations were done by Graph Pad In Stat 3 software (demo version free software of GraphPad Software, Inc. CA, USA). The observed difference in mean distribution of QTc intervals was compared by Student’s t-test or Mann Whitney U test. We evaluated strength of association between QTc and various parameters by calculating odds ratio, keeping con fidence interval of 95%, taking QTc > 0.43 second in males and QTc > 0.45 second in females as positive outcome and QTc ≤ 0.43 sec-ond in males and QTc ≤ 0.45 second in females as negative outcome. Categorical data were assessed by Fisher’s exact test for signi ficance. Any observed difference was considered statistically signi ficant with P value < 0.05.
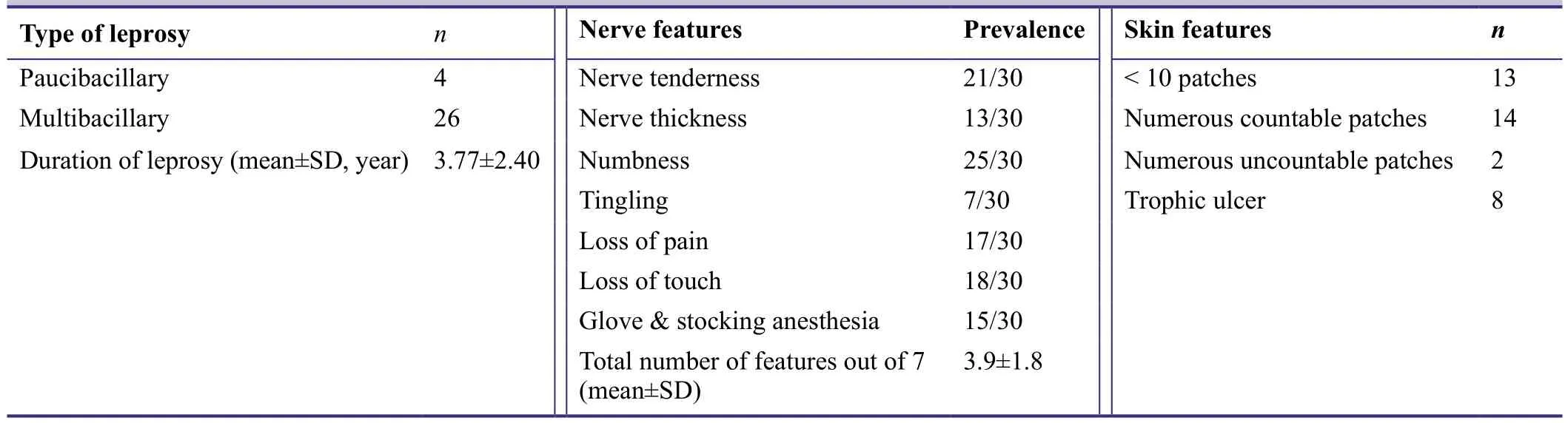
Table 2: Clinical characteristics of case group (n = 30)
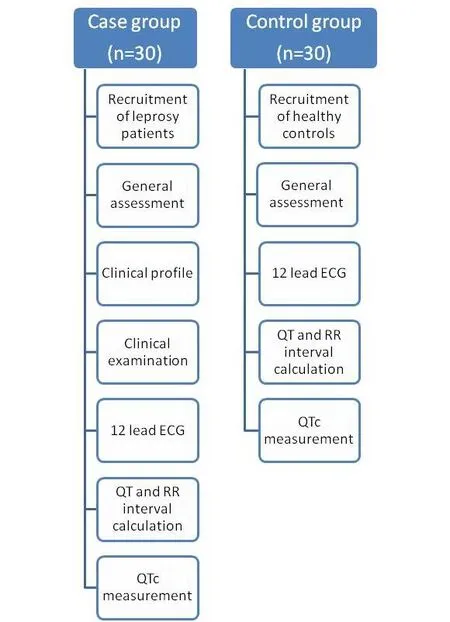
Figure 1: Flow diagram of the study procedure.
RESULTS
Patient characteristics
Thirty leprosy patients (case group) and 30 age- and sexmatched apparently healthy controls (control group) were included in this study (Figure 1). There were 19 males and 11 females in each group. Subjects in the control group were signi ficantly younger than those in the case group (Table 1).

Table 1: Baseline data of case and control groups
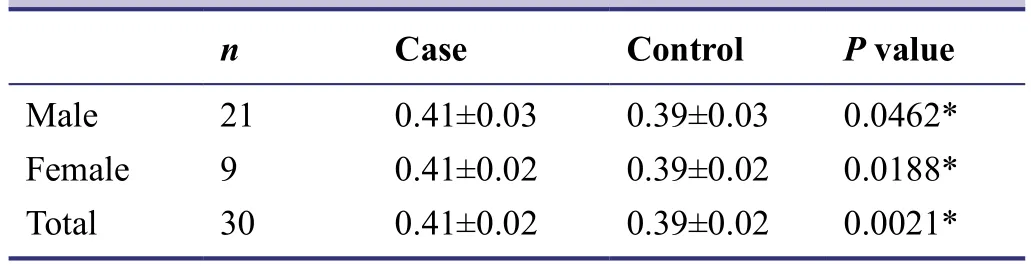
Table 3: Quantitative comparison of QTc interval (second)between case and control groups
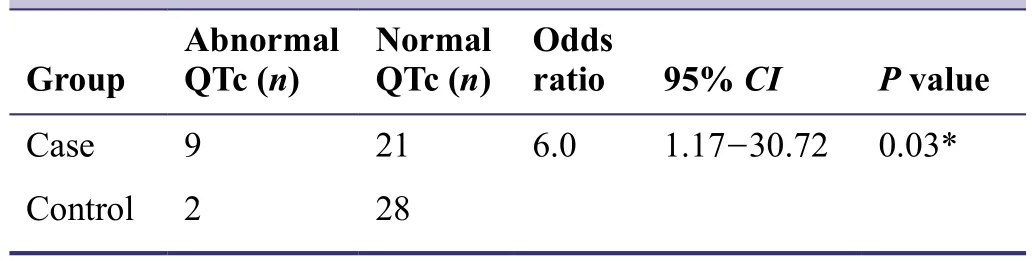
Table 4: Calculation of risk (odds ratio) for prolonged QTc interval due to leprosy
Clinical profile
Clinical pro file of leprosy patients in the case group is shown in Table 2.
QTc interval
QTc interval was signi ficantly greater in case group than in the control group (P < 0.05) (Table 3).
Quantitative comparison was performed using Fisher’s exact test by de fining abnormal QTc as value > 0.43 second in males and value > 0. 45 second in females. The odds ratio of prolonged QTc in the case group was 6 times as great as that in the control group, with signi ficant statistical signi ficance (Table 4).

Table 5: Effects of age, duration of disease, number of nerve features and number of skin patches on QTc interval in the case group
QTc association
We evaluated the effects of age, duration of disease, number of total nerve features and number of skin patches quantitatively on QTc interval. It indicates that QTc correlated with none of these although there were a large number of patients with age > 40 years, disease duration > 4 years,nerve features > 4 or skin patches > 10 (Table 5).
Presence or absence of individual skin or nerve feature did not make signi ficant difference of QTc value in leprosy patients (Table 6).
DISCUSSION
In this study, we studied the clinical pro file of 30 middleaged leprosy patients who had predominantly multibacillary pro file with the mean duration of disease of 4 years. Nearly half of these patients had more than 10 skin patches and nerve features on average presented in 2 out of 3 cases,indicative of severe clinical pro file of leprosy. Our results showed that leprosy patients had signi ficantly greater QTc values than age- and sex-matched controls, which are consistent with previous studies (Agarwal and Aggarwal, 1984;Ulvi et al., 1996). This can be explained by clinical pro file,predominance of multibacillary type and comparatively high mean duration of disease. Our results also revealed that leprosy patients had 6 times odds ratio as great as that in age- and gender-matched controls. QTc prolongation underscores repolarization abnormality which is explained by cardiac autonomic neuropathy. The risk becomes even more obvious considering the mean age of 40 years and the fact that prolonged QTc is a risk for torsades de pointes and sudden cardiac death (Stevens et al., 2013). Anti-leprosy drugs, though taken for months together, are not known to affect QTc interval and this further potentiates the role of Leprae bacilli. To the best of our knowledge, simple ECG based detection of QTc prolongation has not been cited much, our study perhaps highlights it. QTc interval has beenused as a simple non-invasive marker of abnormal cardiac autonomic status for diseases like hypertension (Maule et al., 2008) and diabetes mellitus (Subbalakshmi et al., 2010).We found the same inference in leprosy patients, but in a small sample size through a cross-sectional study.
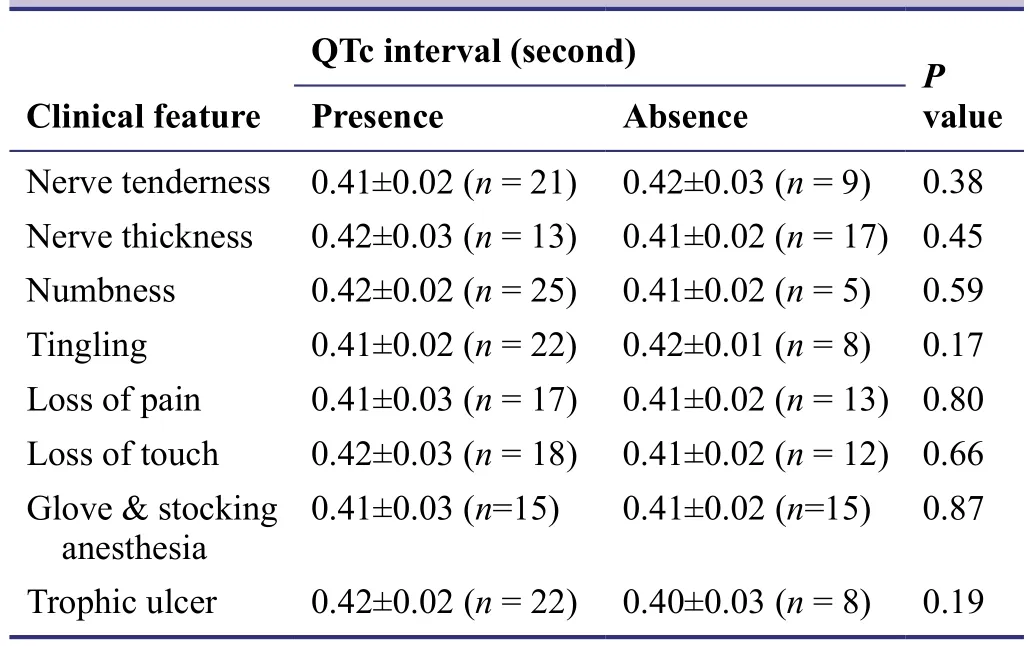
Table 6: Effect of presence of individual nerve and skin feature on QTc interval in the case group
We found that QTc interval was prolonged in female leprosy patients than in male leprosy patients, which is consistent with other studies (Villareal et al., 2001; Nielsen et al., 2014) focusing on some other common neuropathies.Age did not correlate with QTc, and this occurs because of the average age is 40 years. However, for other causes of cardiac autonomic neuropathy, age has a signi ficant positive correlation (Nielsen et al., 2014). The number of skin patches does re flect the severity of sensory or motor neuropathy, but it did not affect QTc in our study. Our results showed that nerve features were unrelated to QTc values.These two facts indicate that peripheral neuropathy is not running parallel to cardiac neuropathy, just in support of a previous study (Ulvi et al., 1996). Invasion of somatic nerve precedes that of cardiac autonomic nerve (Kale et al., 1984). 2/3 of cases had clinically evident somatic neuropathy while only 1/3 of cases had cardiac neuropathy as revealed by QTc prolongation, which is consistent with a previous study (Agarwal and Aggarwal, 1984). 10% of normal subjects have prolonged QTc values (Lionetti, 2005)but 27% prevalence in our case was signi ficantly greater than that in normal controls. In this study, female leprosy patients accounted for only 1/3 of the total leprosy cases and they were at a greater risk of prolonged QTc interval than males. As leprosy is not prevalent in western countries in the world, few studies are performed regarding this issue.Assessment of neuropathy is mostly done for peripheral nerves using sensory modalities (Kar et al., 2013). More studies are necessary to determine the prognostic value of the repolarization dispersion parameters in the prediction of sudden autonomic complication in leprosy patients. Our study was limited by a small sample size, cross-sectional nature, no follow-up observation, and subjective QTc measurement. Nevertheless, this study revealed high prevalence of prolonged QTc that is independent of peripheral neuropathy or skin features, unaffected by age, duration or other disease features.
Taken together, we observed high prevalence of abnormally prolonged QTc with female disadvantage in the middle-aged leprosy patients having predominantly male gender and multibacillary bacteriological pro file. Leprosy imposed 6 times risk for prolonged QTc as great as that for age- and gender-matched healthy controls. QTc value, a feature of cardiac autonomic neuropathy, did not correlate with age, duration or clinical pro file for leprosy and peripheral neuropathy. Leprosy patients are at risk for cardiac autonomic neuropathy as evidenced by QTc, and in-depth studies are needed to con firm this conclusion.
Conflicts of interest
None declared.
Author contributions
JDS, HHM, CJS, and HBM designed the trial protocol. AMT collected data. JDS and HHM wrote the manuscript. AMT,HHM and JDS participated in trial design and conduction.All authors approved the final version of the manuscript.
We are grateful to Department of Physiology and Dermatology, Government Medical College, India for allowing us to perform this study.
Plagiarism check
This paper was screened twice using CrossCheck to verify originality before publication.
Peer review
This paper was double-blinded and stringently reviewed by international expert reviewers.
Agarwal S, Aggarwal SK (1984) Electrocardiographic changes in multi bacillary leprosy. Ind J Lepr 56:569-574.
Bazett HC (1920) An analysis of the time-relations of electrocardiograms. Heart:353-370.
Cabalar M, Yayla V, Ulutas S, Senadim S, Oktar AC (2014) The clinical & amp; neurophysiological study of leprosy. Pak J Med Sci 30:501-506.
Charosky CB, Gatti JC, Cardama JE (1983) Neuropathies in Hansen's disease. Int J Lepr Other Mycobact Dis 51:576-586.
Freeman R (2005) Autonomic peripheral neuropathy. Lancet 365:1259-1270.
Jacob JT, Franco-Paredes C (2008) The stigmatization of leprosy in India and its impact on future approaches to elimination and control. PLoS Negl Trop Dis 2:e113.
Kale HD, Zawar PC, Chawhan RN, Kulkarni GR (1984) Cardiac dysautonomia in lepromatous leprosy. Indian J Lepr 56:563-568.
Kar S, Krishnan A, Singh N, Singh R, Pawar S (2013) Nerve damage in leprosy: An electrophysiological evaluation of ulnar and median nerves in patients with clinical neural de ficits: A pilot study. Indian Dermatol Online J 4:97-101.
Kilborn MJ, Woosley RL (2001) Registry for torsades de pointes with drug treatment exists. BMJ 322:672-673.
Lanjewar P, Pathak V, Lokhandwala Y (2004) Issues in QT interval measurement. Indian Pacing Electrophysiol J 4:156-161.
Leprosy Neuropathy-Medscape Reference. Available from emedicine.medscape.com/ article/1165419.[Last accessed on 8 July 2015] .
Lionetti V (2005) Relationship between QT interval and cardiovascular risk factors in healthy young subjects. J Hum Hypertens 19:623-627.
Maule S, Rabbia F, Perni V (2008) Prolonged QT interval and reduced heart rate variability in patients with uncomplicated essential hypertension. Hypertens Res 31:2003-2010.
Mora-Brambila AB, Trujillo-Hernández B, Coll-Cardenas R, Huerta M, Trujillo X, Vásquez C, Olmedo-Buenrostro BA, Millan-Guerrero RO, Elizalde A (2006) Blink re flex, H-re flex and nerveconduction alterations in leprosy patients. Lepr Rev 77:114-120.
Moss AJ (1999) The QT interval and torsade de pointes. Drug Safety 21:5-10.
National Leprosy Eradication Programme (NLEP) - Progress Report for the year 2013-14. [accessed on July 6, 2015]. Available from:http://nlep.nic.in/pdf/Progress%20report%2031st%20March%20 2013-14.pdf.
Nations SP, Katz JS, Lyde CB, Barohn RJ (1990) Amersterdam, the Netherlands: Excerpta Medica.
Nielsen JB, Graff C, Rasmussen PV, Pietersen A, Lind B, Olesen MS, Struijk JJ, Hauns? S, Svendsen JH, K?ber L, Gerds TA,Holst AG (2014) Risk prediction of cardiovascular death based on the QTc interval: evaluating age and gender differences in a large primary care population. Eur Heart J 35:1335-1344.
Singal A, Sonthalia S (2013) Leprosy in post-elimination era in India: dif ficult journey ahead. Indian J Dermatol 58:443-446.
Stevens S, Reinier K, Chugh S (2013) Increased left ventricular mass as a predictor of sudden cardiac death: Is it time to put it to the test? Circ Arrhythm Electrophysiol 6:212-217.
Subbalakshmi NK, Adhikari PM, Sathyanarayana KN (2010) In fluencing factors of QTc among the clinical characteristics in type 2 diabetes mellitus. Diabetes Res Clin Pract 88:265-272.
Suzuki K, Akama T, Kawashima A, Yoshihara A, Yotsu RR, Ishii N(2012) Current status of leprosy: epidemiology, basic science and clinical perspectives. J Dermatol 39:121-129.
Ulvi H, Yi?iter R, Yolda? T, Dolu Y, Müngen B (1996) Autonomic and Electrocardiographic Examination in Patients with Chronic and Inactive Lepromatous Leprosy and Compared Peripherie Nerve Conduction Studies. Indian J Lepr 68:49-54.
Villareal RP, Woodroof AL, Massumi A (2001) Gender and cardiac arrhythmias. Tex Heart Inst J 28:265-275.
World Health Organization Expert Committee on Leprosy (1988)7th report. Geneva: World Health Organization.
Zhao Z, Yuan Z, Ji Y, Wu Y, Qi Y (2010) Left ventricular hypertrophy ampli fies the QT, and Tp-e intervals and the Tp-e/QT ratio of left chest ECG. J Biomed Res 24:69-72
 Asia Pacific Journal of Clinical Trials:Nervous System Diseases2016年3期
Asia Pacific Journal of Clinical Trials:Nervous System Diseases2016年3期
- Asia Pacific Journal of Clinical Trials:Nervous System Diseases的其它文章
- Efficacy of spontaneous laughter in the post-operative treatment of pain and anxiety in children: study protocol for a randomized controlled trial
- Effect of pre-incisional anterior scalp block on intraoperative opioid consumption in adult patients undergoing elective craniotomy to remove tumor: study protocol for a randomized double-blind trial
- Effects of lung protective ventilation on pulmonary function,inflammation, and oxidative stress in patients undergoing craniotomy: study protocol for a multi-center, randomized,parallel, controlled trial
- Effects of cognitive behavioral therapy on white matter fibers of patients with obsessive-compulsive disorder as assessed by diffusion tensor imaging: study protocol for a parallel group,controlled trial
- Migraine prevention by noninvasive electrical fastigial nucleus stimulation: a multi-center, randomized, double-blind,sham-controlled trial
- Scalp acupuncture twisting manipulation for treatment of hemiplegia after acute ischemic stroke in patients: study protocol for a randomized, parallel, controlled, single-blind trial