
Migraine prevention by noninvasive electrical fastigial nucleus stimulation: a multi-center, randomized, double-blind,sham-controlled trial
2016-04-09 08:53:47JuanYangShuOuJieZhangWeiweiDongJianWangJinheLou
Juan Yang, Shu Ou, Jie Zhang, Wei-wei Dong, Jian Wang,, Jin-he Lou
1 Department of Neurology, Chengdu Second People’s Hospital, Chengdu, Sichuan Province, China
2 Department of Neurology, the Second Affiliated Hospital of Chongqing Medical University, Chongqing, China
3 Department of Neurology, Chongqing Fourth People’s Hospital, Chongqing, China
4 Department of Neurology, the First Affiliated Hospital of Chongqing Medical University, Chongqing, China
5 Department of Neurology, Chongqing People’s Hospital, Chongqing, China
BACKGROUND
Migraine is a primary pain characterized by recurrent episodes of moderate to severe headache. The pain generally affects one side of the head, is pulsating, lasts for 4-72 hours, is often accompanied by nausea, vomiting, and sensitivity to light, sound or smell, and is worsened after physical activity (Headache Classi fication Subcommittee of the International Headache Society, 2004). Global prevalence of migraine is appropriately 15%, with approximately 100 million people worldwide affected (Vos et al., 2012) and a higher prevalence in females than males (19% vs. 11%)(Vos et al., 2012). Moreover, migraine prevalence in Asian populations is lower than in European and American, but is still over 10% (Wang, 2003). Anti-epileptic drugs, antidepressants, calcium antagonists, and β-receptor blockers reduce the frequency and intensity of migraines (Gilmore and Michael, 2011; Jackson et al., 2012; Loder et al., 2012;Silberstein et al., 2012; Shamliyan et al., 2013). However,their use is limited because of strict medication times and high costs (Lipton et al., 2001), as well as potential adverse reactions including myocardial ischemia, disturbed sleep,sexual dysfunction, dry mouth, obesity, tremor, hair loss,and fetal birth defects (Silberstein et al., 2004; Bartleson and Cutrer, 2010; Gilmore and Michael, 2011). In addition,ergotamine overdose may increase migraine frequency and intensity (Headache Classi fication Subcommittee of the International Headache Society, 2004; Tepper and Tepper,2010). Thus, migraine patients have to weigh the adverse reactions of several drugs against repeated headache episodes. For migraine patients with frequent attacks, intense pain, and poor drug control, non-drug measures may help prevent migraine.
Cerebellar bioelectrical stimulation is a non-invasive physical therapy. The neuroprotective effects of electrical fastigial nucleus stimulation (FNS) were first con firmed by Reil et al. (1998) from Cornell University. FNS pretreatment can prevent subsequent cerebral ischemic injury, with the underlying mechanism reported to be related to FNS inhibition of peri-infarction depolarizing waves (PIDs) (Golanov and Zhou, 2003). FNS has also been shown to improve cerebrovascular microcirculation and regional cerebral blood flow (Nakai et al., 1983; Reis et al., 1991; Yamamoto et al., 1993; Zhang and Iadecola, 1993; Chronicle and Mulleners, 1996), inhibit in flammatory reactions by reducing the release of in flammatory factors (Galea et al., 1998a, b),alleviate cerebral edema and nerve injury, reduce neuronal necrosis and apoptosis in the ischemic region (Golanov et al., 1998; Glickstein et al., 1999), reduce infarct volume(Yamamoto et al., 1993; Golanov et al., 1996; Reis et al.,1998), stabilize brain excitability (Chronicle and Mulleners, 1996), and exhibit neuroprotective effects and promote the recovery of neurological de ficits (Golanov and Zhou,2003). Accordingly, we have used FNS to treat various brain injuries (Table 1).
The pathological mechanism underlying migraine remains poorly understood, but most authors assume that cortical spreading depression (CSD) and trigeminal nerve vasculitis co-mediate the occurrence of migraine. CSD refers to the phenomenon of neuronal activation followed by inhibition,speci fically, neurons propagate on the cortical surface at 2-5 mm/min for 15-30 minutes, leading to destruction of cellular ionic gradients and resulting in inhibition of neuronal activity. An imaging study con firmed the changes in cerebral blood flow and cerebral activity in patients with migraine(with or without aura), which suggest the presence of CSD(Sprenger and Borsook, 2012). CSD activates the trigeminal vascular system, increases sensitivity, and consequently initiates a series of nerve, vascular and in flammatory events that finally induce migraine (Gasparini et al., 2013; Karatas et al., 2013; Cui et al., 2014). As a pathogenic factor,CSD likely plays a key role in the occurrence of migraine.Therefore, FNS for CSD and in flammation inhibition can theoretically prevent migraine. Previous observational studies have demonstrated that non-invasive FNS prevents migraines with good safety (Huo and Yu, 2001; Lin et al.,2002; Wang et al., 2007). However, in these studies, the sample sizes are small, only a few institutions are included,and the trial protocol is not rigorous enough. Consequently,the data obtained are not reliable.
In this study, we will validate the ef ficacy of electrical cerebellar FNS for the prevention of migraine using a multicenter, randomized, double-blinded placebo-controlled trial.
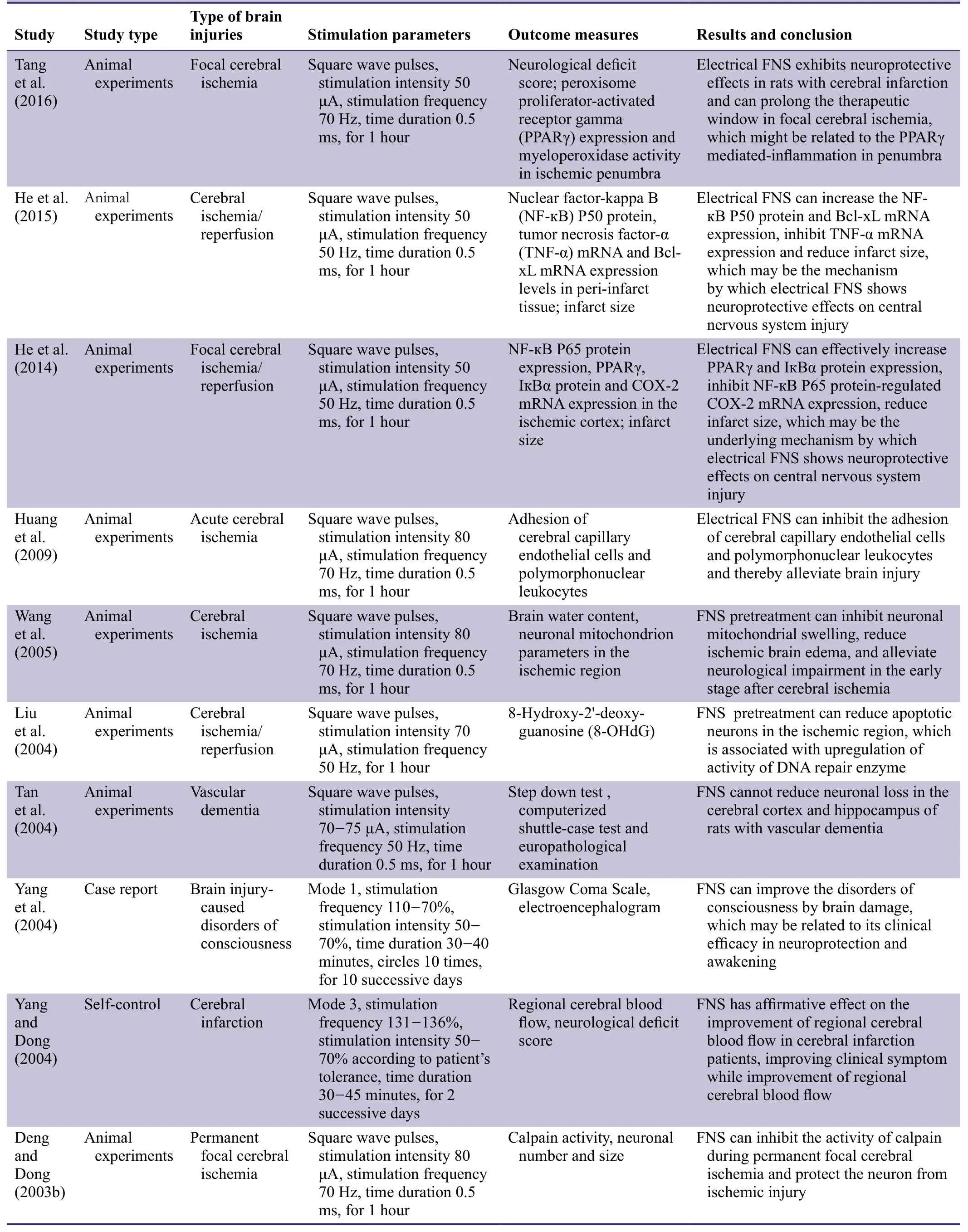
Table 1: Previous studies addressing the treatment of acute massive cerebral infarction using nimodipine
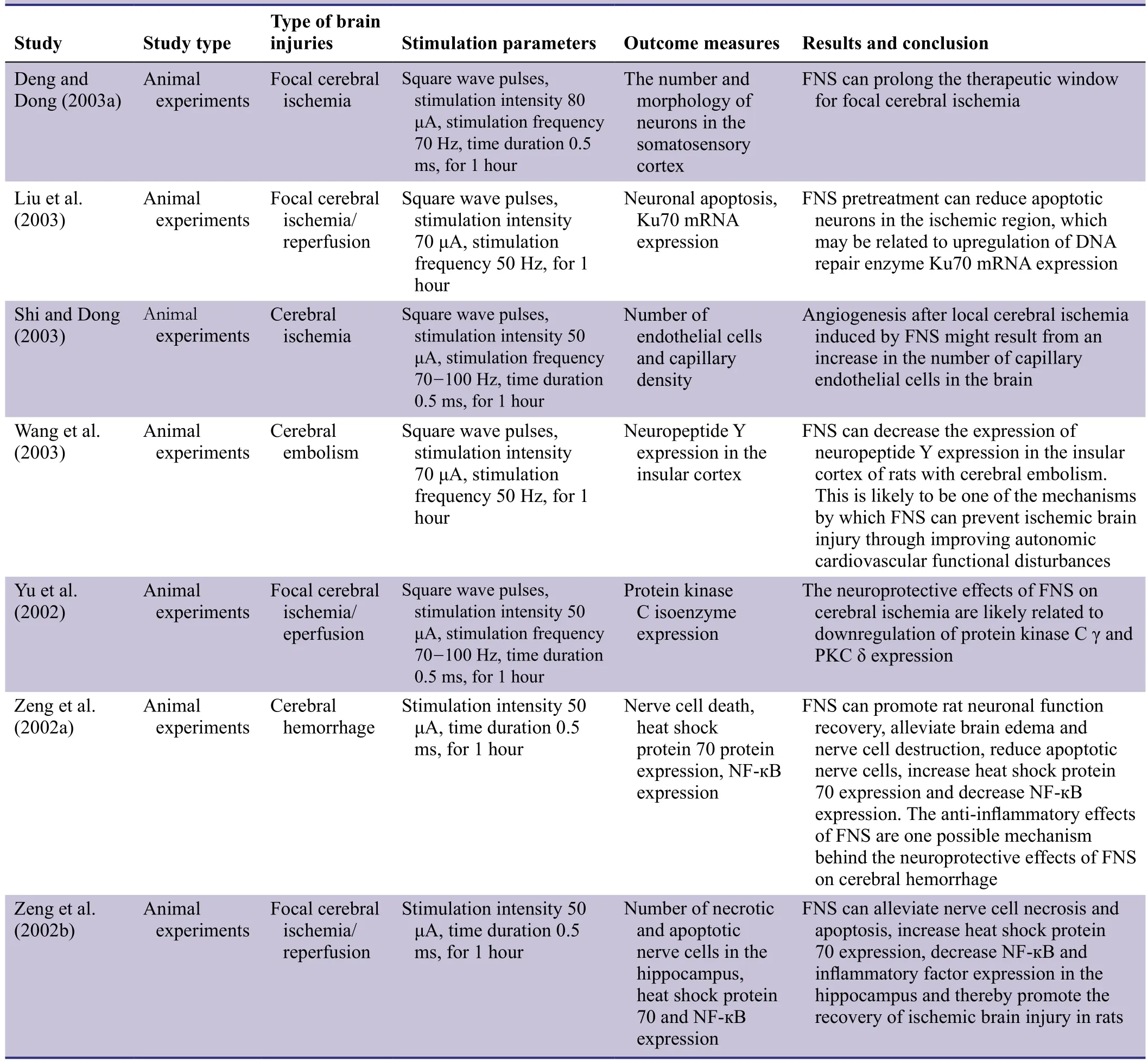
Table 1: Continued
METHODS/DESIGN
Study design
A multi-center, randomized, double-blind, sham-controlled trial.
Study setting
The trial will be performed at Chengdu Second People’s Hospital, the Second Af filiated Hospital of Chongqing Medical University, Chongqing Fourth People’s Hospital, the First Af filiated Hospital of Chongqing Medical University, and Chongqing People’s Hospital, China.
Study procedure
The study is designed to validate the ef ficacy and safety of non-invasive FNS on prevention of migraine. Patients with migraine were screened against our inclusion and exclusion criteria (see below). Eighty eligible patients were randomly allocated to FNS and sham-stimulation groups. The flow chart of the trial protocol is shown in Figure 1.
Study participants
Inclusion criteria
Patients satisfying all the following criteria were considered for admission to the trial:
· Diagnosed with migraine according to The International Classi fication of Headache Disorders: 2ndedition (Headache Classi fication Subcommittee of the International Headache Society, 2004)
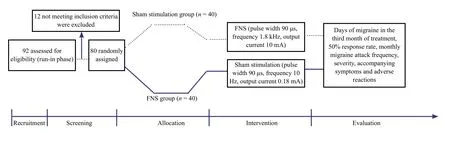
Figure 1: Flow chart of the study protocol.
· Age 18-65 years
· First onset age ≤ 50 years old
· Course of disease ≥ 1 year
· In the remission stage, with a migraine attack frequency≥ twice per month
· Voluntarily participating in the trial with provision of informed consent regarding the trial procedure
Exclusion criteria
Patients presenting with any of the following criteria were excluded from the trial:
· Have taken anti-migraine drugs such as β receptor blockers, calcium antagonists, anti-epileptic drugs, antidepressants, or serotonin receptor antagonists in the previous 3 months
· Have used at least three types of preventive drugs such as β receptor blockers, calcium antagonists, anti-epileptic drugs, antidepressants, or serotonin receptor antagonists
· Headaches related to drug abuse (use of painkillers because of headaches lasting more than 10 days)
· Alcohol and/or other drug abuse
· Taking hormone therapy
· Severe mental disorder
· Complicated by severe primary cardiovascular, hepatic,renal, or hematopoietic system diseases
· Pregnant or lactating
Withdrawal criteria
Patients will be withdrawn from the trial because of any of the following conditions:
· Patients do not meet the inclusion criteria but conform to the exclusion criteria and are recruited because of errors
· Patients do not receive treatment according to the therapeutic regimen or cannot provide complete information
· Patients cannot participate in the trial because of severe adverse events
· Patients need to take emergency measures because of complications or a worsened pathological condition
· Poor patient compliance, and consequently receive treatment for < 80% of required days or take other treatments
Sample size
From the perspective of safety issues, according to our preliminary experiments, the effective rate in the shamstimulation group was 15%, while in the FNS group was 55%. To test for signi ficant differences between shamstimulation and FNS groups, the signi ficance level was α= 5% (two-sided), with the power being β = 90%.According to the formula ,

uαand uβare u values corresponding to α and β, while p1and p2are the calculated frequency values for two samples,with p being the merged value of two sample frequencies.Accordingly, n = 28 was calculated. Taking into account a ‘lost to follow-up’ rate of 20%, n = 34 was calculated as the lowest sample size for each group. Therefore, n = 40 was used as the sample size for each group.
Recruitment
Migraine patients were recruited from five hospitals to participate in the trial through various public invitation methods including advertisements, posters, and lea flets. The invitation posters or lea flets were posted in the waiting room,rest room, and entrance of hospital buildings. Participants interested in participating in the trial contacted the person in charge by telephone or e-mail. After providing written and 3rdmonth of treatment; and 50% response rate, i.e.,percentage of patients having at least a 50% reduction of monthly migraine days in the 3rdmonth of treatment.informed consent, all potential participants were screened according to our inclusion and exclusion criteria.
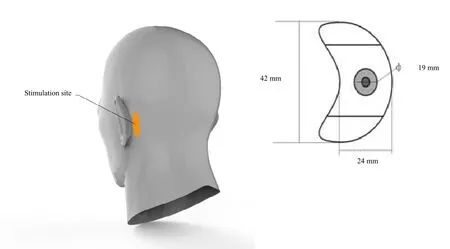
Figure 2: Position of the stimulation electrode placed on the mastoid area behind the ear
Randomization
Eligible patients will be observed for 1 month for baseline collection prior to grouping. Patients suffering from two or more migraine attacks per month will be allocated to the FNS or sham-stimulation groups on a 1:1 ratio.
Blinding
Treatment allocation will not be disclosed until the end of the trial and will be performed according to the principle of block randomization. Noninvasive FNS equipment and sham-stimulation equipment look the same, and have the same manual and parameters. Therefore, FNS and shamstimulation equipment cannot be distinguished.
Interventions
FNS group
After cleaning the skin, the stimulating electrode (Chongqing Haikun Medical Appliance Co., Ltd., Chongqing, China)will be positioned in the mastoid bone behind the ear. The size of the electrode is 42 mm × 24 mm with a conductive area of Φ19 mm (Figure 2). The stimulation parameters include: pulse width 90 μs, frequency 1.8 kHz, and output current 10 mA. Participants will receive FNS once a day for 45 minutes, for 3 successive days.
Sham-stimulation group
The sham-stimulation parameters include: pulse width 90 μs, frequency 10 Hz, and output current 0.18 mA. Participants will receive FNS once a day for 45 minutes, for 3 successive days.
Outcome measures
Primary outcome measures
Change in monthly migraine days between the run-in month
Secondary outcome measures
(1) Change in average monthly migraine days across 3 months of treatment.
(2) Monthly migraine days in the 3rdmonth of treatment.
(3) Severity of migraine as determined by the visual analogue scale (VAS) score, with score 0 indicating no pain and score 10 representing most pain (Collins et al., 1997),in the 3rdmonth of treatment; accompanying symptoms include migraine aura, nausea/vomiting, extreme sensitivity to light, sounds, or smells, and use of analgesics.
(4) Change in monthly anti-migraine drug use between the run-in month and 3rdmonth of treatment.
(5) Migraine disability assessment (MIDAS) questionnaire score. The questionnaire is designed to examine headachecaused disability in working and daily life. The questionnaire score is calculated by the sum of days in the last 3 months in which the patient missed work or school; did not perform household work; missed family, social, or leisure activities; or experienced a reduction in work or school productivity by half or more because of headache (Stewart et al., 1999).
(6) Adverse reactions including local skin irritation, pain,or other discomfort.
Patient’s baseline characteristics are shown in Table 2 and the schedule for outcome assessments is shown in Table 3.
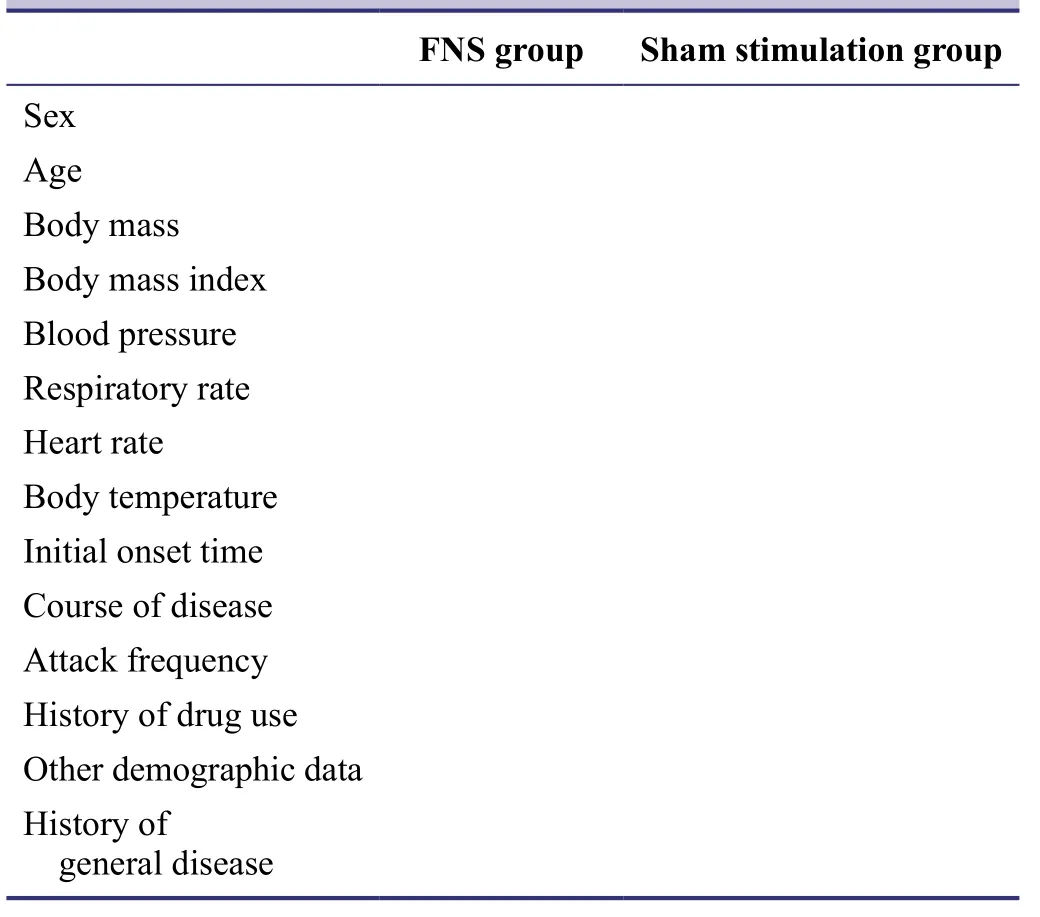
Table 2: Patient’s baseline data
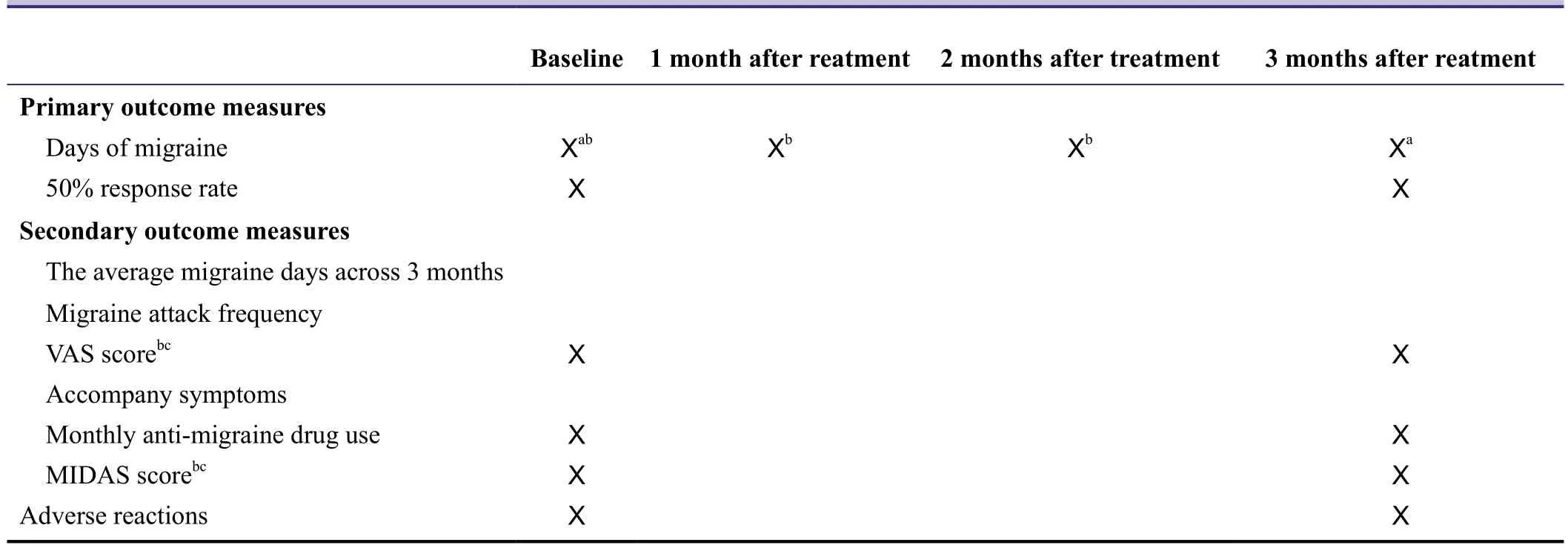
Table 3: Schedule of outcome assessments
Data collection, management, analysis, and open access
Two persons will not participate in recruitment of participants, and will be responsible for collecting patients’migraine diaries (containing number of FNS applications and duration of a single stimulation, and which will be completed by the patients themselves), and creating a database. During treatment, patients will be followed up once per month. After blinded auditing and collation,the created database will be locked by the researcher in charge and will not be altered. All information relating to this trial will be stored by Chengdu Second People’s Hospital. The electronic database will be fully disclosed to a professional statistician for statistical analysis, and the results reported to the researcher in charge. An independent data-monitoring committee will monitor data collection and management to ensure a scienti fic, rigorous, real, and complete research process. Anonymized trial data will be published at http://www. figshare.com.
Statistical analysis
All data will be statistically analyzed using SPSS 11.5 software. Accompanying symptoms and adverse reactions will be expressed as percentages and tested using the chi-square test. The remaining results will be expressed as the mean ±SD. The Mann-Whiney U test will be used for comparisons of primary and secondary outcome measures between FNS and sham-stimulation groups. The non-parametric Sign test will be used for comparisons of monthly changes in indices between the 3rdmonth of treatment and run-in month, as well as between average outcomes across 3 months and the run-in month. A level of P < 0.05 will be considered statistically signi ficant.
Auditing
Trial progression will be reported to the ethics committee of Chengdu Second People’s Hospital, China every 6-12 months, and the trial status updated in the registration database.
Confidentiality
All information relating to this trial will be stored in a secure, locked place for future viewing, and not disclosed to any non-authorized person. Researchers participating in this trial will adhere to the con fidentiality and privacy agreements.
DISCUSSION
In this trial, to reduce the body surface sensation of current stimulation, intermediate frequency peak currents will be superimposed, with the largest current peak being 10 mA, and leading to a current change of 1-1.2 mA. This low-frequency signal will be modulated within 13-45 Hz.Within this frequency range, current change and modulated signal do not cause an obvious body surface sensation of current stimulation, and only a slight squeezing sensation is felt. The intermediate frequency signal is an exponential decay signal, with ‘a’ (0 < a < 1) as the base. Nonpolar differential exponential waveform is composed of positive and negative pulse waves with equal charge. Negative exponential pulses play a role in nerve fiber depolarization,while positive pulses have a charge-balancing role, resulting in an ingested static charge of 0 and leading to the lowest production of electrical stimulation-caused adverse electrochemical reactions. To reduce single pulse energy, under the condition of a constant pulse width of 90 μs, reduced base value accelerates decay and alleviates the squeezing sensation. When subjected to sham-stimulation, a patient’s body surface sensation will be periodically point-touch sensitive. Therefore, patients and physicians cannot distinguish between FNS and sham-stimulation, which ensures double-blinded clinical signi ficance of the results. Thus, our results will clarify the ef ficacy of daily FNS treatment in the prevention of migraine, and objectively provide effective theoretical evidence for the clinical application of FNS.
Trial status
Data summary and statistical analysis are undergoing at the time of submission.
Conflicts of interest
None declared.
Author contributions
JW conceive and design the trial protocol. SO, JZ, WWD and JHL are the head of each trial center. JY write the manuscript. All authors approve the final version of this manuscript for publication.
Plagiarism check
This paper was screened twice using CrossCheck to verify originality before publication.
Peer review
This paper was double-blinded and stringently reviewed by international expert reviewers.
Bartleson JD, Cutrer FM (2010) Migraine update. Diagnosis and treatment. Minn Med 93:36-41.
Chronicle E, Mulleners W (1996) Visual system dysfunction in migraine: a review of clinical and psychophysical findings. Cephalalgia 16:525-535.
Collins SL, Moore RA, McQuay HJ (1997) The visual analogue pain intensity scale: what is moderate pain in millimetres? Pain 72:95-97.
Cui Y, Kataoka Y, Watanabe Y (2014) Role of cortical spreading depression in the pathophysiology of migraine. Neurosci Bull 30:812-822.
Deng ZK, Dong WW (2003a) The effect of fastigial nucleus electrical stimulation on the therapeutic window of opportunity for in tervention of focal cerebral ischemia. Zhonghua Yixue Zazhi 83:1173-1175.
Deng ZK, Dong WW (2003b) The effect of fastigial nucleus electrical stimulation on the activity of calpain during permanent focal cerebral lschemia. Zhongguo Linchuang Shenjing Kexue 11:250-253.
Galea E, Glickstein SB, Feinstein DL, Golanov EV, Reis D (1998a)Stimulation of cerebellar fastigial nucleus inhibits interleukin-1beta-induced cerebrovascular in flammation. Am J Physiol 275:H2053-2063.
Galea E, Golanov EV, Feinstein DL, Kobylarz KA, Glickstein SB,Reis DJ (1998b) Cerebellar stimulation reduces inducible nitric oxide synthase expression and protects brain from ischemia. Am J Physiol 274:H2035-2045.
Gasparini CF, Sutherland HG, Grif fiths LR (2013) Studies on the pathophysiology and genetic basis of migraine. Curr Genomics 14:300-315.
Gilmore B, Michael M (2011) Treatment of acute migraine headache. Am Fam Physician 83:271-280.
Glickstein SB, Golanov EV, Reis DJ (1999) Intrinsic neurons of fastigial nucleus mediate neurogenic neuroprotection against excitotoxic and ischemic neuronal injury in rat. J Neurosci 19:4142-4154.
Golanov EV, Zhou P (2003) Neurogenic neuroprotection. Cell Mol Neurobiol 23:651-663.
Golanov EV, Yamamoto S, Reis DJ (1996) Electrical stimulation of cerebellar fastigial nucleus fails to rematch blood flow and metabolism in focal ischemic infarctions. Neurosci Lett 210:181-184.
Golanov EV, Liu F, Reis DJ (1998) Stimulation of cerebellum protects hippocampal neurons from global ischemia. Neuroreport 9:819-824.
He LY, Luo Y, Wang J, Dong WW (2015) Effect of electrical stimulation to cerebellar fastigial nucleus on cerebral ischemia-reperfusion injury in Rats. Zhongguo Kangfu Lilun yu Shijian 21:1012-1015.
He LY, Zhang B, Luo Y, Dong WW, Wang YL (2014) Effects of electrical stimulation to cerebellar fastigial nucleus on expressions of NF-кB, PPARγ, IкBα and COX-2 mRNA under cerebral ischemia/reperfusion in rats. Zhongguo Kangfu Yixue Zazhi 29:107-112.
Headache Classi fication Subcommittee of the International Headache Society (2004) The International Classi fication of Headache Disorders: 2ndedition. Cephalalgia 24 Suppl 1:9-160.
Heurteaux C, Lauritzen I, Widmann C, Lazdunski M (1995) Essential role of adenosine, adenosine A1 receptors, and ATP-sensitive K+channels in cerebral ischemic preconditioning. Proc Natl Acad Sci U S A 92:4666-4670.
Huang W, Xu MM, Chen X, Dong WW, Xie P (2009) Experimental study of effects of FNS on intercellular adhesion in acute cerebral ischemia in rats. Chongqing Yixue 38:1993-1998.
Huo S, Yu WH (2001) Curative effects of electrical cerebellar fastigial nucleus stimulation on migraine. Xiandai Kangfu 25:88.
Jackson JL, Kuriyama A, Hayashino Y (2012) Botulinum toxin A for prophylactic treatment of migraine and tension headaches in adults: a meta-analysis. JAMA 307:1736-1745.
Karatas H, Erdener SE, Gursoy-Ozdemir Y, Lule S, Eren-Ko?ak E,Sen ZD, Dalkara T (2013) Spreading depression triggers headache by activating neuronal Panx1 channels. Science 339:1092-1095.
Lin BR, Wang T, Hu WK (2002) Electro-stimulation on cerebellum fastigial nucleus for migraine in 40 cases. Shanghai Zhongyiyao Zazhi 36:26-27.
Lipton RB, Diamond S, Reed M, Diamond ML, Stewart WF (2001)Migraine diagnosis and treatment: results from the American Migraine Study II. Headache 41:638-645.
Liu JL, Dong WW, Li JP (2003) Effect of fadtigial nucleus electrical stimulation on Ku expression in rat with focal cerebral ischemia and reperfusion. Zhongguo Linchuang Shenjing Kexue 11:117-120.
Liu JL, Li JP, Dong WW (2004) Fastigial nucleus electrical stimulation protecting against ischemia-reperfusion induced oxidative DNA damage in rat brain. Zuzhong yu Shenjing Jibing 11:147-150.
Loder E, Burch R, Rizzoli P (2012) The 2012 AHS/AAN guidelines for prevention of episodic migraine: a summary and comparison with other recent clinical practice guidelines. Headache 52:930-945.
Nakai M, Iadecola C, Ruggiero DA, Tucker LW, Reis DJ (1983)Electrical stimulation of cerebellar fastigial nucleus increases cerebral cortical blood flow without change in local metabolism:Evidence for an intrinsic system in brain for primary vasodilation.Brain Res 260:35-49.
Reis DJ, Berger SB, Underwood MD, Khayata M (1991) Electrical stimulation of cerebellar fastigial nucleus reduces ischemic infarction elicited by middle cerebral artery occlusion in rat. J Cereb Blood Flow Metab 11:810-818.
Reis DJ, Kobylarz K, Yamamoto S, Golanov EV (1998) Brief electrical stimulation of cerebellar fastigial nucleus conditions longlasting salvage from focal cerebral ischemia: conditioned central neurogenic neuroprotection. Brain Res 780:161-165.
Shamliyan TA, Choi JY, Ramakrishnan R, Miller JB, Wang SY, Taylor FR, Kane RL (2013) Preventive pharmacologic treatments for episodic migraine in adults. J Gen Intern Med 28:1225-1237.
Shi ZH, Dong WW (2003) Role of fastigial nuclei stimulation on angiogenesis in rats with local cerebral ischemia. Zhongfeng yu Shenjing Jibing Zazhi 20:250-252.
Silberstein SD, Neto W, Schmitt J, Jacobs D; MIGR-001 Study Group (2004) Topiramate in migraine prevention: Results of a large controlled trial. Arch Neurol 61:490-495.
Silberstein SD, Holland S, Freitag F, Dodick DW, Argoff C, Ashman E (2012) Evidence-based guideline update: Pharmacologic treatment for episodic migraine prevention in adults: Report of the Quality Standards Subcommittee of the American Academy of Neurology and the American Headache Society. Neurology 78:1337-1345.
Sprenger T, Borsook D (2012) Migraine changes the brain: neuroimaging makes its mark. Curr Opin Neurol 25:252-262.
Stewart W, Lipton R, Kolodner K, Liberman J, Sawyer J (1999)Reliability of the migraine disability assessment score in a population-based sample of headache sufferers. Cephalalgia 19:107-114.
Takaba H, Nagao T, Yao H, Kitazono T, Ibayashi S, Fujishima M(1997) An ATP-sensitive potassium channel activator reduces infarct volume in focal cerebral ischemia in rats. Am J Physiol 273:R583-586.
Tan XL, Dong WW, Yang QD (2004) The prophylactic and curative effects of electrical stimulation of cerebellar fastigial nucleus on vascular dementia in rats. Zuzhong yu Shenjing Jibing 11:349-352.
Tang WJ, Dong WW, Xie P, Cheng PF, Bai SJ, Ren YF, Wang G,Chen XY, Cui C, Zhuang XX, Huang W (2016) Effect of precondition cerebella fastigial nucleus electrical stimulation within and beyond the time window of thrombolytic on ischemic stroke in rats. Disan Junyi Daxue Xuebao 38:27-31.
Tepper SJ, Tepper DE (2010) Breaking the cycle of medication overuse headache. Cleve Clin J Med 77:236-242.
Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M,Shibuya K, Salomon JA, Abdalla S, Aboyans V, Abraham J, Ackerman I, Aggarwal R, Ahn SY, Ali MK, AlMazroa MA, Alvarado M, Anderson HR, Anderson LM, Andrews KG, et al. (2012) Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380:2163-2196.
Wang H, Han XR, Zhang N (2007) Curative ef ficacy of electrical cerebellular fastigial nucleus stimulation in the treatment of migraine. Zhongguo Shiyong Shenjing Jibing Zazhi 10:114.
Wang J, Dong WW, He W (2005) Effect of preconditioning electrostimulation of fastigial nucleus on neuronal mitochondrion of rat early after cerebral ischemia. Zhonghua Wuli Yixue yu Kangfu Zazhi 27:9-13.
Wang SJ (2003) Epidemiology of migraine and other types of headache in Asia. Curr Neurol Neurosci Rep 3:104-108.
Wang YM, Liu XD, Dong WW, Luo XD, Yang ZC (2003) Effects of electric stimulation of the cerebellar fastigial nucleus on the expression of insular cortex neuropeptide Y in rats with cerebral embolism. Disan Junyi Daxue Xuebao 19:1751-1754.
Yamamoto S, Golanov EV, Reis DJ (1993) Reductions in focal ischemic infarctions elicited from cerebellar fastigial nucleus do not result from elevations in cerebral blood flow. J Cereb Blood Flow Metab 13:1020-1024.
Yang J, Dong WW (2004) The effect of fastigial nucleus stimulation on cerebral blood flow of cerebral infarction patients. Xiandai Yiyao Weisheng 20:3-4.
Yang J, Dong WW, Zhong SH (2004) Clinical research of fastigial nucleus electrical stimulation in treatment of disorders of consciousness by brain damage. Chongqing Yike Daxue Xuebao 29:383-385.
Yu G, Dong WW, Luo Y, Peng GG (2002) Effect of fore-stimulation of cerebellar fastigial nucleus on cerebral PKC γ and PKC δ expression in cerebral ischemia-reperfusion rats. Zhenci Yanjiu 27:10-13.
Zeng JQ, Yu G, Dong WW (2002a) Expression of in flammatory factors in ischemic penumbra after experimental cerebral haemorrhage and the effects of fastigial nucleus stimulation (FNS).Chongqing Yixue 31:394-396.
Zeng JQ, Dong WW, Yu G (2002b) Expression of HSP70 and NF-κB in hippocampus CA1 of rat brain after focal cerebral ischemia/reperfusion and the effects of fastigial nucleus stimulation (FNS).Zhongguo Laonian Xue Zazhi 22:289-291.
Zhang F, Iadecola C (1993) Fastigial stimulation increases ischemic blood flow and reduces brain damage after focal ischemia. J Cereb Blood Flow Metab 13:1013-1019.
 Asia Pacific Journal of Clinical Trials:Nervous System Diseases2016年3期
Asia Pacific Journal of Clinical Trials:Nervous System Diseases2016年3期
- Asia Pacific Journal of Clinical Trials:Nervous System Diseases的其它文章
- Evaluation of cardiac autonomic status using QTc interval in patients with leprosy
- Efficacy of spontaneous laughter in the post-operative treatment of pain and anxiety in children: study protocol for a randomized controlled trial
- Effect of pre-incisional anterior scalp block on intraoperative opioid consumption in adult patients undergoing elective craniotomy to remove tumor: study protocol for a randomized double-blind trial
- Effects of lung protective ventilation on pulmonary function,inflammation, and oxidative stress in patients undergoing craniotomy: study protocol for a multi-center, randomized,parallel, controlled trial
- Effects of cognitive behavioral therapy on white matter fibers of patients with obsessive-compulsive disorder as assessed by diffusion tensor imaging: study protocol for a parallel group,controlled trial
- Scalp acupuncture twisting manipulation for treatment of hemiplegia after acute ischemic stroke in patients: study protocol for a randomized, parallel, controlled, single-blind trial