
Primary Combined Intra-articular and Extra-articular Synovial Osteochondromatosis of Shoulder: a Case Report
2014-04-20 01:37:38AshishDevganVinayGuptaNarenderMaguandRajeshRohilla
Chinese Medical Sciences Journal 2014年4期
Ashish Devgan, Vinay Gupta, Narender K Magu, and Rajesh Rohilla
Department of Orthopaedic Surgery, Paraplegia & Rehabilitation, Pt. B.D. Sharma, Post Graduate Institute of Medical Sciences, Rohtak, Haryana 124001, India
PRIMARY synovial chondromatosis is a rare condition in which foci of cartilage develop in the synovial membrane of joints, bursae and tendon sheaths. It typically involves a single large joint in a young adult male.1The ectopic foci of cartilage can result in painful joint effusion, and the generation of loose bodies can cause mechanical symptoms.2,3The etiology of primary synovial chondromatosis remains unknown, but metaplastic theory is the most popular hypothesis. The commonly involved joints are knee, elbow, and hip.4The shoulder is a rare site of synovial chondromatosis2,3,5and the extra-articular involvement even rarer, with only few cases presented in literature. This report presents a rare case of primary combined intra-articular and extra-articular synovial chondromatosis of shoulder joint treated with arthroscopy.
CASE DESCRIPTION
A 22-year-old male visited the authors’ institute with complaints of pain, swelling and restriction of movement of the left shoulder joint since 11 months before. The pain was insidious in onset and aggravated with joint move- ments. The patient also had frequent locking episodes of the left shoulder joint and he used to unlock the joint by himself with little manipulation. There was no history of trauma, fever or other joint pains. Range of motion was terminally restricted, especially abduction and flexion. On shoulder movement gritty sensation could be palpated. Routine blood tests results were normal. Serological tests for rheumatoid arthritis and tuberculosis were negative. There were no degenerative changes in glenohumeral joint. Anteroposterior radiograph of shoulder joint (Fig. 1) revealed multiple calcified nodules in left glenohumeral joint, axillary recess anterior to the humeral head, inferior recess of shoulder joint capsule and the subcoracoid recess. Computed tomography (CT) scan (Fig. 2) showed osteochondral loose bodies in left shoulder joint, some of which were extending in bursal space and in the subcoracoid recess. Magnetic resonance imaging (MRI) confirmed the CT findings. The lesion located in the subcoracoid recess had no connection with the intra- articular lesion.
The patient consented for arthroscopic surgery to remove the intra-articular loose bodies and synovectomy of the joint. In lateral decubitus position, standard arthro- scopy portals were used whilst switching the viewing and working portals depending upon the location of loose bodies. Normal saline was used as irrigation fluid. The loose bodies hidden in recesses were squeezed out into view for removal. Sheathed 5.5-mm cutter was used for synovec- tomy. Portals were closed by single silk sutures. In total 84 loose bodies were removed and sent for histopatho- logical examination, which showed lobules of chondroid tissue along with osseous metaplasia, consistent with synovial chondromatosis without any evidence of malignant transformation.

Figure 1. Plain skiagram of the shoulder (anteroposterior view) showing multiple small round calcified lesions having “popcorn ball like” appearance.
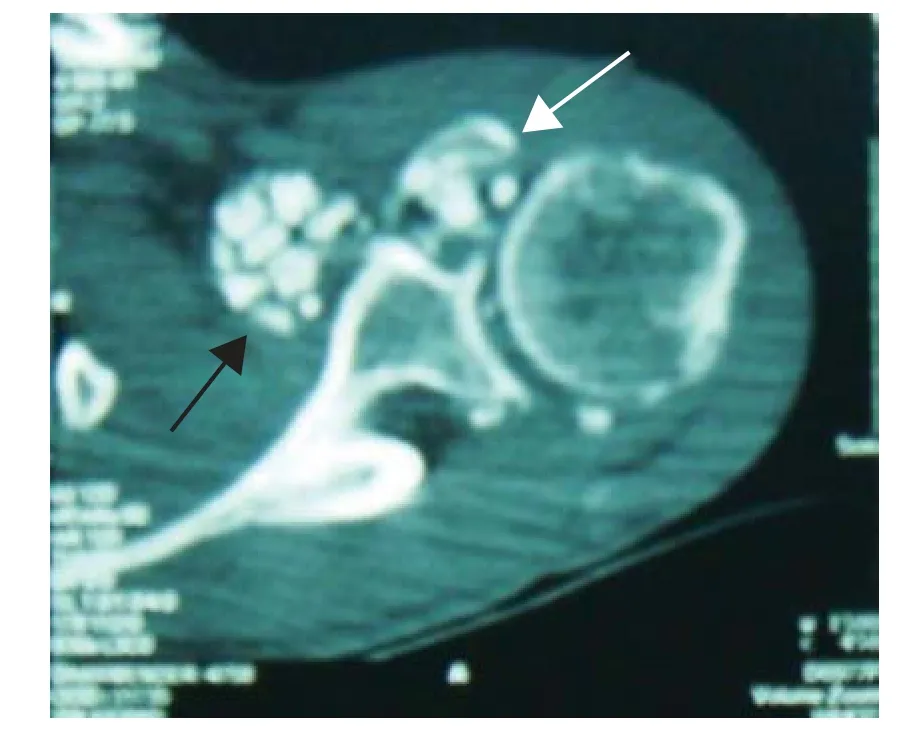
Figure 2. Axial CT scan of the shoulder showing both intra- articular (white arrow) and extra-articular (black arrow) location of loose bodies, the extra-articular ones in the subcoracoid recess.
The extra-articular loose bodies in the subcoracoid recess were not removed as they were asymptomatic. The patient was relieved of his pain and locking episodes after the surgery. The range of movements improved and he returned to his work. At three-and-half year follow-up examination, the patient was asymptomatic, with no clinical or radiological evidence of recurrence of the lesion and the extra-articular loose bodies remained asymptomatic.
DISCUSSION
Synovial chondromatosis is characterized by metaplasia of synovium resulting in formation of multiple osteochondral loose bodies. The etiology is unknown but metaplastic theory is the most favored one.2,6It commonly affects the age group of 20-40 years.6It is twice more common in males than in females.6,7Involvement in this rare disorder is typically mono-articular, with a benign course, affecting knee, elbow, hip and ankle joints (in order of frequency), and the shoulder joint very infrequently.4,5
The clinical course of this condition is characterized by mild pain, effusion of the affected joint and mechanical symptoms of recurrent locking and joint stiffness.7,8Milgram and Hadesman8defined three histological phases of synovial osteochondromatosis: (1) active intrasynovial phase, (2) transitional lesions phase and (3) quiescent (inactive) intrasynovial phase. Complications of the disease are recurrence, secondary osteoarthritis and malignant transformation to synovial chondrosarcoma.3None of these were present in our case. Typical X-ray findings for synovial osteochondromatosis are multiple, smooth, oval shaped, calcified masses within the joint space or in the synovium-lined extra-articular space. They have typical “popcorn ball appearance” of calcified cartilage. Apart from X-rays, MRI, CT, arthrogram, and bone-scanning are also very helpful. The MRI appearance of synovial chondromatosis depends on the pulse sequences used and the presence of calcium. Areas of calcification will have very low signal intensity regardless of pulse sequence. The distribution of the high signal intensity abnormality in the glenohumeral joint, axillary recess and subscapularis bursa in this patient's coronal MRI indicated an intra-articular process. The abundant proliferating cartilage was also localized anteriorly in subcoracoid bursa, an extra-articular location.
Primary synovial chondromatosis of the shoulder itself is a rare entity (5% of the cases) and the involvement of the extra-articular site around shoulder is even rarer with only few cases presented in literature.3,9Kirsti et al6reported a case of primary synovial chondromatosis of subdeltoid/subacromial bursae. Kumar et al5also reported a completely extra-articular primary synovial osteochon- dromatosis of a subdeltoid bursa. Our article reports extremely rare entity of primary combined intra- as well as extra-articular synovial chondromatosis in the shoulder joint where the extra-articular location was in the subcoracoid bursa anteriorly, superficial to the subscapular muscle and not connected with the intra-articular lesion. Although we tried to remove all the intra-articular loose bodies during arthroscopy along with synovectomy, postoperative radiographs showed a few remaining intra- articular loose bodies. We did not remove the extra-articular loose bodies. These remaining intra-articular and the extra- articular loose bodies did not cause any symptoms and the patient gained good painless range of motion.
The treatment of synovial chondromatosis is surgical.2,3,10Loose bodies damage the joint and osteoarthritis com- plicates the untreated joint and impairs the result when treatment is delayed. Therefore, early removal of loose bodies is indicated to prevent further damage to articular surface.4Open or arthroscopic surgery is performed with resection of the diseased synovium and removal of intra- articular loose bodies.2,3,10Chillemi et al2recommended arthroscope-assisted synovectomy and removal of loose bodies in primary synovial chondromatosis of the shoulder and considered it an easy and safe method for management of this disorder. Arthroscopy is a technically demanding procedure and has a steep learning curve, but it is a very safe, effective and reproducible method per se for management of synovial osteochondromatosis. It is a fast, effective, and minimally invasive method with least morbidity and negligible blood loss. It is extremely beneficial in performing a thorough synovectomy of shoulder especially in narrow recesses and corners both anteriorly and posteriorly. In the present case, after the arthroscopic removal of intra- articular loose bodies and synovectomy, the patient regained full range of motion without any postoperative stiffness.
1. Mankin HJ. Synovial Chondromatoses. In: Pathophysiology of orthopaedic diseases. Rosemont: American Academy of Orthopaedic Surgeons; 2006. p. 53-8.
2. Chillemi C, Marinelli M, de Cupis V. Primary synovial chondromatosis of the shoulder: clinical, arthroscopic and histopathological aspects. Knee Surg Sports Traumatol Arthrosc 2005; 13:483-8.
3. Buess E, Friedrich B. Synovial chondromatosis of the glenohumeral joint: a rare condition. Arch Orthop Trauma Surg 2001; 121:109-11.
4. Lim SJ, Chung HW, Choi YL, et al. Operative treatment of primary synovial osteochodromatosis of the hip. J Bone Joint Surg Am 2006; 88:2456-64.
5. Kumar A, Agarwal A, Sahni VK. Primary synovial osteochondromatosis of a subdeltoid bursa. Indian J Orthop 2010; 44:104-7.
6. Kiritsi O, Tsitas K, Grollios G. A case of idiopathic bursal synovial chondromatosis resembling rheumatoid arthritis. Hippokratia 2009; 13: 61-3.
7. McGrory JE, Rock MG. Synovial chondromatosis of the shoulder. Am J Orthop (Belle Mead NJ) 2000; 29:793-5.
8. Milgram JW, Hadesman WM. Synovial osteochondromatosis in the subacromial bursa. Clin Orthop Relat Res 1988; 236: 154-9.
9. Antonogiannakis E, Yiannakopoulos CK, Mataragas I. Osteochondromatosis of the subacromial bursa, arthroscopic treatment of a case and review of literature. EEXOT 2008; 59:67-70.
10. Park JH, Noh HK, Bada LP, et al. Arthroscopic treatment for synovial chondromatosis of the subacromial bursa: a case report. Knee Surg Sports Traumatol Arthrosc 2007; 15: 1258-60.
 Chinese Medical Sciences Journal2014年4期
Chinese Medical Sciences Journal2014年4期
- Chinese Medical Sciences Journal的其它文章
- Inhibition of Xanthine Oxidase Activity by Gnaphalium Affine Extract
- Evaluation of Risk Factors for Arytenoid Dislocation after Endotracheal Intubation: a Retrospective Case-control Study
- Non-enhanced Low-tube-voltage High-pitch Dual-source Computed Tomography with Sinogram Affirmed Iterative Reconstruction Algorithm of the Abdomen and Pelvis
- Squamous Cell Carcinoma of Small Intestine: a Case Report△
- BRAF V600E Mutation as a Predictive Factor of Anti-EGFR Monoclonal Antibodies Therapeutic Effects in Metastatic Colorectal Cancer: a Meta-analysis
- Multiple Myeloma Mimicking Spondyloarthritis: a Case Report