
Choroidal Tuberculoma in an ImmunocompetentYoung Patient
2011-11-22 02:35:52XiufenYangJunXuandKaiMa
Chinese Medical Sciences Journal 2011年3期
Xiu-fen Yang *,Jun Xu ,and Kai Ma
1Beijing Tongren Eye Center,Beijing Ophthalmology and Visual Sciences Key Laboratory,Beijing Tongren Hospital,Capital Medical University,Beijing 100730,China
2Department of Ophthalmology,Liaocheng Renmin Hospital,Liaocheng,Shandong 252000,China
TUBERCULOSIS (TB) remains one of the leading causes of preventable morbidity and mortality from infectious disease worldwide.1It is a chronic progressive granulomatous infection caused byMycobacteriumtuberculosis (M.tuberculosis).Ocular involvement in patients with systemic TB has traditionally been considered uncommon.The incidence of ocular TB was reported to be 1.46% among 10 524 patients in a TB sanatorium2and there are only few reports of choroidal tuberculoma in the literature.3-5Here we reported a case of choroidal tuberculoma in an immunocompetent young patient with a history of tuberculous pleurisy.
CASE DESCRIPTION
A 20-year-old man presented with diminished vision and dysmorphopsia in his right eye of 2 months duration.His best-corrected visual acuity was 20/200 in the right eye and 20/20 in the left eye.Anterior segment examination was unremarkable in both eyes.Dilated fundus examination of the right eye showed yellowish-white elevated choroidal mass-like lesions (tuberculoma) with indistinct borders varying in elevation and size,extending circumferentially on the temporal side beyond the arcade in the posterior pole.The major choroidal lesion at the superior temporal region to the macula was approximately 6 to 7 disk diameter in size.Two smaller choroidal lesions were seen just inferior to the major lesion.The lesions were accompanied by exudative retinal detachment.The macula was affected with retinal detachment and yellowish-white subretinal exudates.Dilated fundus examination was unremarkable in the left eye.Fluorescein angiography (FA) of the right eye showed early hypofluorescence,later hyperfluorescence,diffuse leakage around the mass,and a pooling of dye during the late phase,corresponding to the exudative retinal detachment.
This patient had a history of tuberculous pleurisy 4 years ago and healed after antituberculosis treatment.At this examination,chest X-ray showed no obvious abnormalities.A purified protein derivative skin test was highly positive (in duration,25 mm).We investigated this patient for HIV screening and the result was negative.The clinical diagnosis of choroidal tuberculoma was therefore suggested.
Then the patient was tentatively treated by a standard regimen of four-drug antitubercular therapy,including isoniazid,rifampicin,ethambutol,and pyrazinamide,monitored by an internist.Two months after the antitubercular therapy,obvious healing was noticed in the right eye,with best corrected visual acuity improved to 40/200.The patient still had the symptom of dysmorphopsia.Fundus photograph showed shrinkage of the choroidal lesions and disappearance of exudative retinal detachment (Fig.1A).Optical coherence tomography (OCT) found an elevation of the choroid lesion and subtle subretinal fluid (Fig.1A).The diagnosis of choroidal tuberculoma was confirmed based on effective response to the treatment.Four months after antitubercular treatment,his best corrected visual acuity improved to 60/200 in the right eye.Fundus photograph showed continued shrinkage of the choroidal lesions (Fig.1B).The major lesion became flattened,while the inferior lesion showed signs of chorioretinal scar.Subretinal fluid was absorbed completely as shown by OCT(Fig.1B).
Four months after the patient had completed a 12-month antituberculosis therapy,the patient still had symptom of dysmorphopsia.Best corrected visual acuity in the right eye was limited to 60/200.Fundus photograph showed further shrinkage of the yellowish lesion with well-defined and pigmented borders surrounded by atrophic retinal pigment epithelium halos (Fig.1C).Choroidal lesions were reduced with signs of retinal fibrosis.
DISCUSSION
Ocular tuberculosis commonly presents in the choroid by hematogenous spread from the primary complex or the secondary lesions.Choroiditis can occur focally or diffusely in variable shapes caused by direct infection or immunologic reaction response to TB antigens (delayed hypersensitivity).The most common presenting manifestation of intraocular TB was reported to be choroidal tubercles and tuberculomas.6Large tuberculoma is frequently unilateral and appears predominantly in the posterior pole,generally presented as yellowish elevated subretinal mass measured from 4 to 14 mm in size and associated with exudative retinal detachment.Choroidal lesions that are close to the macula may lead to destruction and permanent loss of central visual acuity.Histologically,choroidal tuberculoma results from a progressive,liquefied caseation necrosis with rapid multiplication of tubercular bacilli and tissue destruction.7In early stages,the overlying retinal pigment epithelium remains normal but can be disrupted at later stage with the tuberculoma increasing in size.The tubercles/tuberculomas may involve all layers of choroidal tissue with the progression.
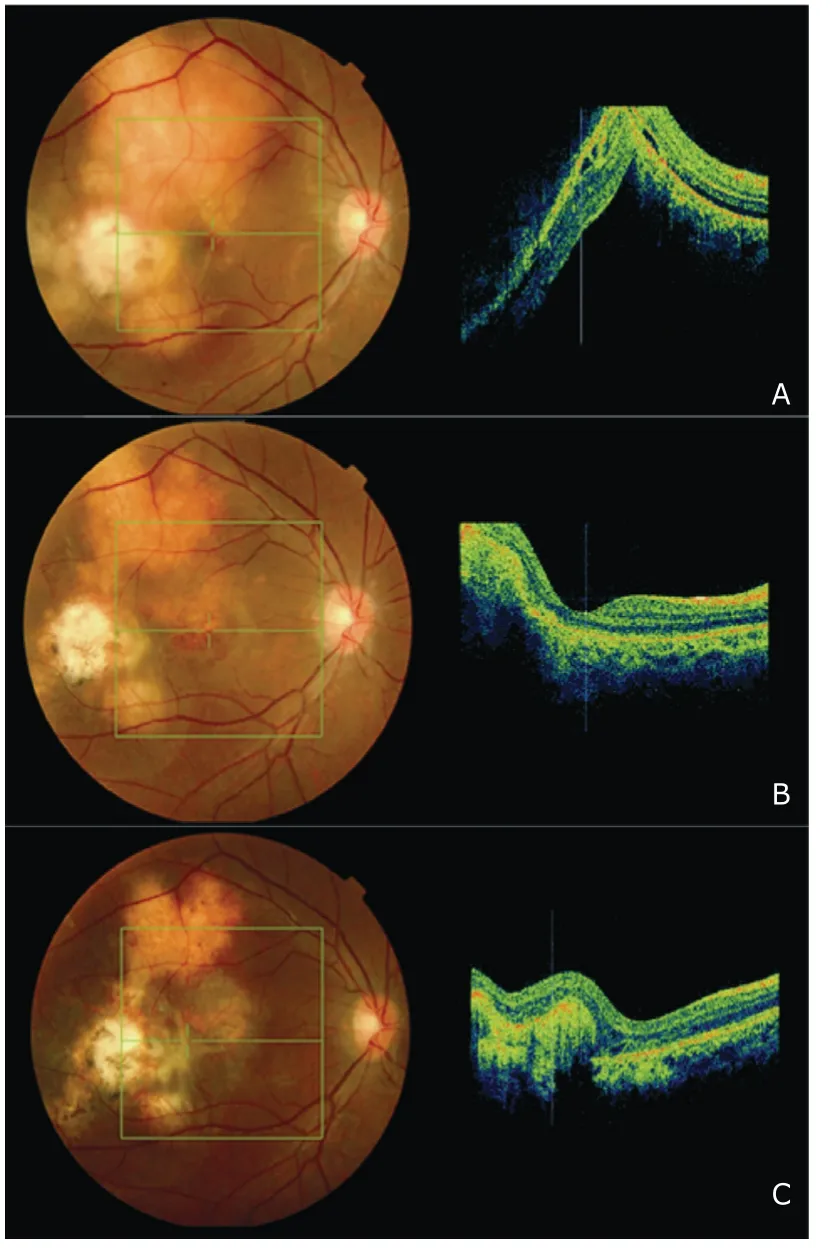
Figure 1.Fundus photographs and optical coherence tomography (OCT) showing the progression of the choroidal tuberculoma in a 20 year-old immunocompetent patient.
The gold standard in the diagnosis of ocular TB has been detection ofM.tuberculosis in the lesions by histological methods or culturing using Lo¨wenstein-Jenson(egg-based) medium.Clinical diagnosis,however,is usually not based on histopathologic or microbiologic evidences as obtaining ocular sample is clinically difficult.The diagnosis of ocular TB is presumptive in majority of the cases in the literature.Ophthalmologists mainly rely on the clinical manifestations,clinical history,systemic examination,and response to treatment.Systemic evaluation includes purified protein derivative skin testing and chest radiography.It is noted,however,that the majority of chest radiographs are normal in TB uveitis.8,9In clinical practice,a tentative diagnosis of choroidal tuberculoma is usually made on the basis of a systemic TB history.The case reported here had a history of tuberculous pleurisy 4 years ago and showed prompt response to antituberculosis therapy,thereby strongly supporting the diagnosis of ocular TB.Unfortunately,the fundus photograph and FA results before the antituberculosis therapy was unavailable when the patient came to us the first time.However,available images could still show the slow recovery after effective treatment.
Most patients with ocular TB require systemic therapy.The principal drugs for antituberculosis include isoniazid,rifampin,pyrazinamide,ethambutol,and streptomycin.No specific local therapy is needed.Visual recovery and tuberculoma involution to a flat inactive scar with or without pigmentation can be obtained after proper treatment.3,5Concomitant corticosteroid use in the treatment of ocular TB is a controversial issue.Additional steroids may be needed in cases of refractory intraocular inflammation,retinal vasculitis and cystoids macula edema.10In this reported case,systemic antituberculosis therapy without the use of steroids was effective for the lesion of intraocular TB.
Given the fact that TB is one of the few causes of uveitis with a definitive effective treatment,early diagnosis and prompt treatment for ocular TB are essential for the effective management and may be sight-saving for the patients.Ophthalmologists should be aware that tuberculous choroiditis can occur in immunocompetent individuals.
1.Espinal MA,Laszlo A,Simonsen L,et al.Global trends in resistance to antituberculosis drugs.N Engl J Med 2001;344:1294-303.
2.Donahue HC.Ophthalmologic experience in a tuberculosis sanatorium.Am J Ophthalmol 1967;64:742-8.
3.Levecq LJ,De Potter P.Solitary choroidal tuberculoma in an immunocompetent patient.Arch Ophthalmol 2005;123:864-6.
4.Ohta K,Yamamoto Y,Arai J,et al.Solitary choroidal tuberculoma in a patient with chest wall tuberculosis.Br J Ophthalmol 2003;87:795-.
5.Gupta V,Gupta A,Arora S,et al.Simultaneous choroidal tuberculoma and epididymo-orchitis caused by Mycobacterium tuberculosis.Am J Ophthalmol 2005;140:310-2.
6.Abu El-Asrar AM,Abouammoh M,Al-Mezaine HS.Tuberculous uveitis.Int Ophthalmol Clin 2010;50:19-39.
7.Gupta A,Gupta V.Tubercular posterior uveitis.Int Ophthalmol Clin 2005;45:71-88.
8.Tabbara KF.Tuberculosis.Curr Opin Ophthalmol 2007;18:493-501.
9.Gupta V,Gupta A,Rao NA.Intraocular tuberculosis-an update.Surv Ophthalmol 2007;52:561-87.
10.Bodaghi B,LeHoang P.Ocular tuberculosis.Curr Opin Ophthalmol 2000;11:443-8.
 Chinese Medical Sciences Journal2011年3期
Chinese Medical Sciences Journal2011年3期
- Chinese Medical Sciences Journal的其它文章
- Sclerosing Cholangitis after Transcatheter Arterial Chemoembolization:a Case Report
- Sutureless Intestinal Anastomosis with a Novel Device of Magnetic Compression Anastomosis△
- Influence of Deleted in Colorectal Carcinoma Gene on Proliferation of Ovarian Cancer Cell Line SKOV-3 In Vivo and In Vitro
- Cytogenetic and Clinical Analysis of 340 Chinese Patients with Primary Amenorrhea
- Serum HIF-1α and VEGF Levels Pre-and Post-TACE in Patients with Primary Liver Cancer
- Effect of Multiple Coatings of One-step Self-etching Adhesive on Microtensile Bond Strength to Primary Dentin