
Sutureless Intestinal Anastomosis with a Novel Device of Magnetic Compression Anastomosis△
2011-11-22 02:36:20ChaoFanJiaMaHongkeZhangRuiGaoJianhuiLiLiangYuZhengWuandYiLv
Chinese Medical Sciences Journal 2011年3期
Chao Fan,Jia Ma,Hong-ke Zhang,Rui Gao,Jian-hui Li,Liang Yu,Zheng Wu,and Yi Lv
Department of Hepatobiliary Surgery,the First Affiliated Hospital,Medical School of Xi’an Jiaotong University,Xi’an 710061,China
THE hand-sewn has always been the most traditional method in intestinal anastomosis over the past 160 years.Although the suture materials in wound closure have been developed and the surgical skills have been greatly improved,the hand-sewn anastomosis seems complicated and time-consuming.In addition,the suture material itself is a potential source for foreign body reaction,and will stir chronic inflammation in the anastomosis which would compromise the healing process and initiate secondary anastomotic leakage and stenosis.The staple suturing facilitates the surgical procedure and saves much time,however,retained titanium in anastomosis is still the potential problem.1,2Moreover,its availability is limited by its high cost.Herein,we invented a novel magnetic compression anastomats (MCAs),to explore the feasibility and efficiency of the MCAs in intestinal anastomotic construction.
MATERIALS AND METHODS
Device design
The anastomats were designed by our research center and manufactured by College of Mechanical Engineering,Xi’an Jiaotong University.The anastomats consist of 2 parts designated as the mother part and the daughter part.The magnetic rings made of sintered-type neodymium-ironboron (NdFeB,N52) are the main bodies of the MCAs,which have an outer diameter of 16 mm and 18 mm;inner diameter of 13 mm and 15 mm;width of 3 mm;thickness of 4 mm.The magntic ring is covered with a magnetic shield,which made of superparamagnetic material.The thickness of magnetic shield is 1 mm and bottom thickness is 1.5 mm.Both NdFeB ring and magetic shield were coated with titanium-nitride surface to make sure that the anastomats have good stability and good biocompatibility with body cells.The specific structures of the anastomats are shown in Figs.1 and 2.

Figure 1.Schematic view of the end-to-side intestinal magnetic compression anastomats (MCAs).
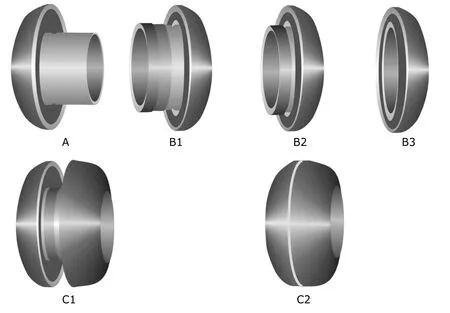
Figure 2.Schematic view of the end-to-end intestinal MCAs.
Animals and grouping
The study protocol was approved by the Institutional Animal Care and Use Committee of our medical college and conducted in accordance with the Guide for the Care and Use of Laboratory Animals published by the National Institutes of Health.
A group of 36 healthy male mongrel canines over 1 year old and more than 15 kg in weight were provided by Experimental Animal Center of Medical College of Xi’an Jiaotong University,and all of them were vaccinated.The mongrel canines were individually housed in 1.5 m3cages,fed with standard chow and free access to water.
The canines were randomly allocated to a study group and a control group (n=18).Both groups were subjected to intestinal anastomosis with either end-to-end or end-toside technique with 9 cases in each subgroup.The mongrel canines in the study and the control groups underwent intestinal anastomosis by MCAs and traditional hand-sewn respectively.At 1 week,1 month and 3 months after surgery,anastomosis time,postoperative complications,bursting pressure of anastomoses,gross appearance,and pathology were evaluated.
Surgical procedure
All canines were intraperitoneally anaesthesized with an injection of 3% sodium pentobarbital liquid (1 mL/kg) after 1-day fast.To avoid postoperative infection,benzylpenicillin sodium was intravenously administered at 100 000 U/kg of body weight 30 minutes before surgery.Water was freely available after recovery from anaesthesia,but solid food was not provided until the 3rd day after operation.All canines continued to receive the prophylactic benzylpenicillin sodium intravenously at 100 000 U/kg of body weight,twice a day for 3 consecutive days.
Surgery was initiated through an upper mid-line laparotomy incision.The procedures are performed by the same surgeons.Roux en Y jejunojejunostomy was performed.The jejunum was incised at 20 cm distal to Treitz's ligament.
End-to-side anastomosis technique:In the control group,end-to-side anastomosis was performed between the proximal jejunal end and jejunum 50 cm distal to the jejunal incision with 3-0 suture (Mersilk?,ETHICON;Johnson &Johnson Medical Ltd.,Shanghai,China).In the study group,the proximal jejunum was purse-string sutured with 4-0 suture (Prolene?,ETHICON,Johnson &Johnson,Somerville,NJ,USA),and the mother part was fixed right there.The daughter part was then placed at 50 cm distal to incision.Gently press mother part against daughter part,the sharp-edged end of central duct of mother part will cut the jejunum wall above daughter part (Fig.3).With the coupling of the two parts,the continuity of jejunum became reconstructed.Then the blind jejunum loop was closed.
End-to-end anastomosis technique:In the control group,end-to-end anastomosis was reconstructed with a double layer closure using 3-0 suture (Mersilk?)in situ.In the study group,both ends of jejunum were purse-string sutured with 4-0 suture (Prolene?).The two parts of the end-to-end MCAs were fixed at the proximal and distal jejunal ends,respectively.Once the mother part and daughter part coupled together,the end-to-end anastomosis was completed (Fig.4).
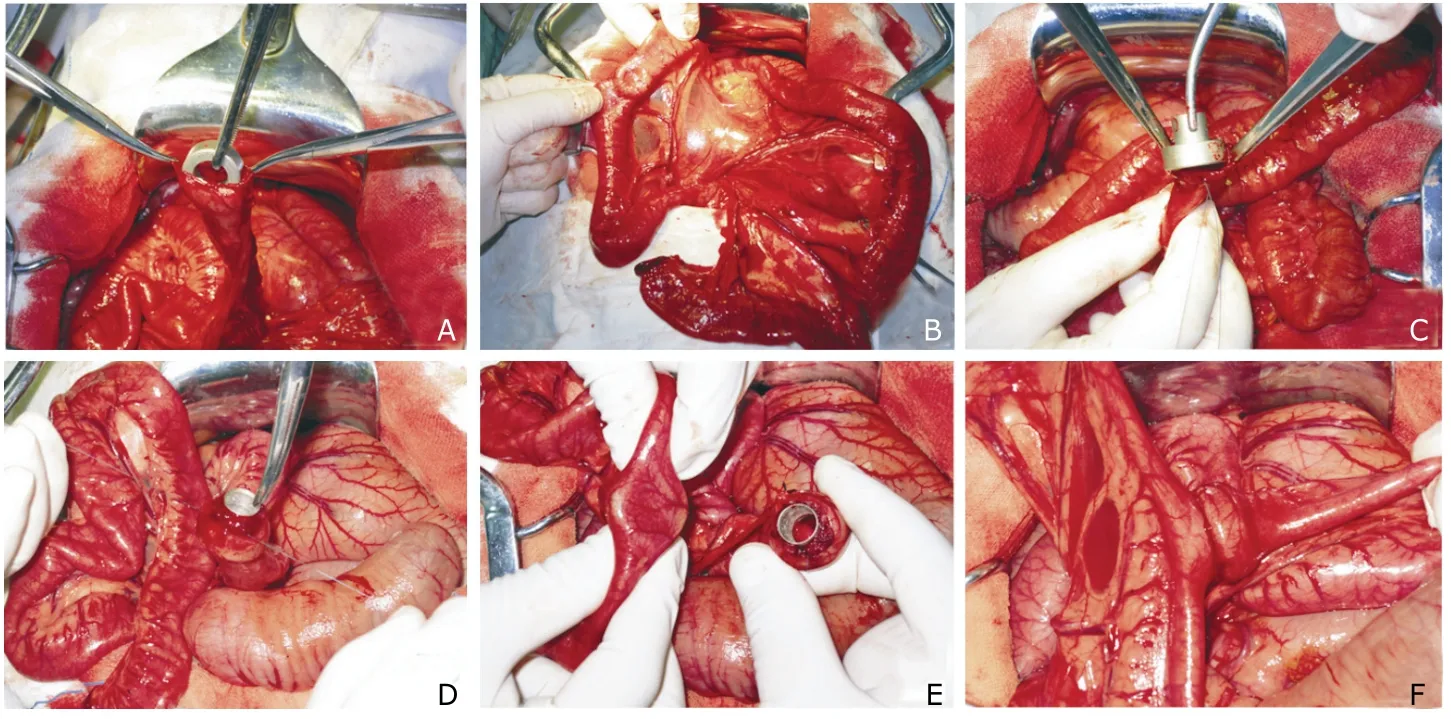
Figure 3.Surgical procedure of end-to-side intestinal anastomosis with MCAs.
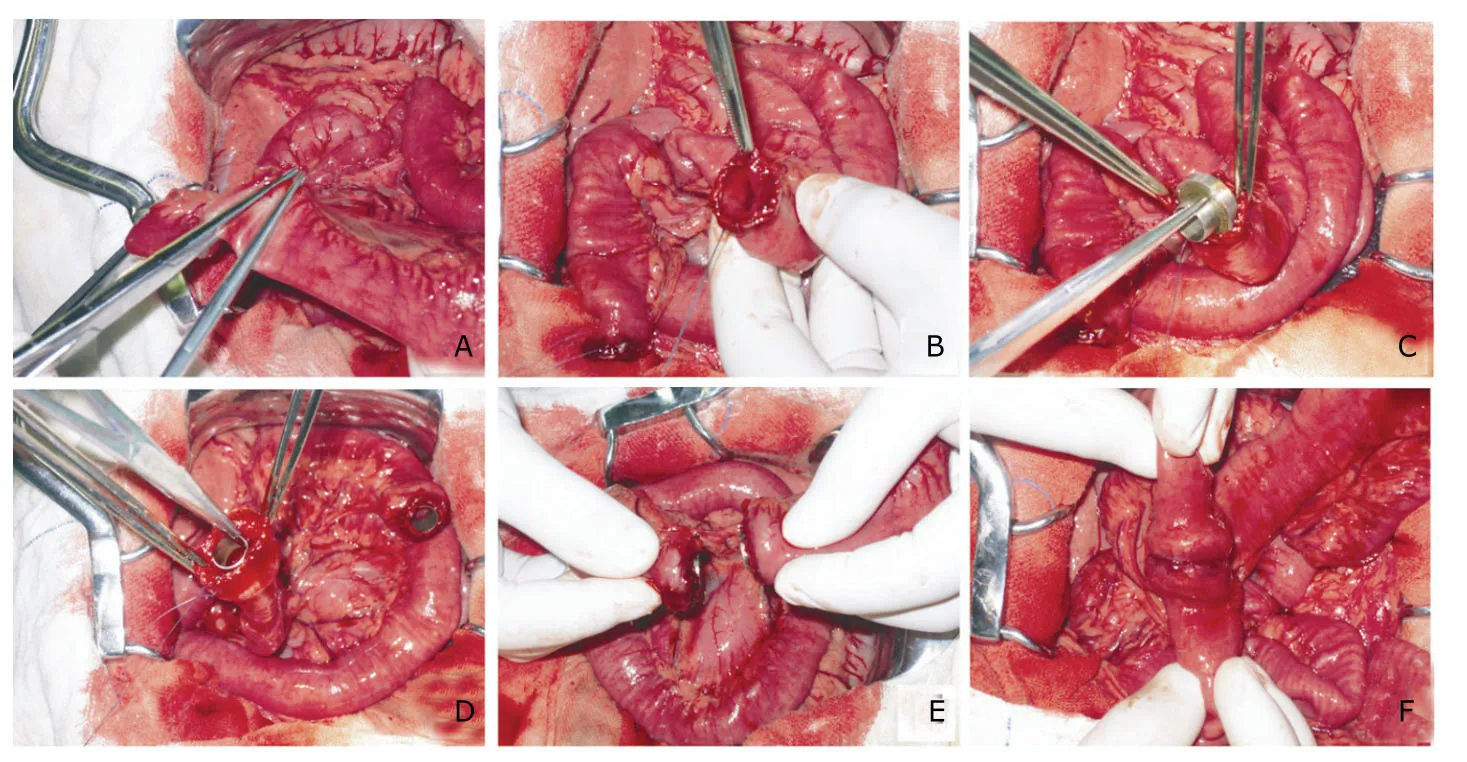
Figure 4.Surgical procedure of end-to-end intestinal anastomosis with MCAs.
Evalution of anastomosis time
The anastomosis time was defined as from the very beginning of anastomotic construction to completing the continuity of the intestine.The time spent on each anastomosis was recorded.
X-ray examination
After operation,plain abdominal X-ray was immediately taken to confirm the accurate coupling of the MCAs.The routine X-ray test was daily carried out to verify the passage of the MCAs in the digestive tract until it disappeared in the photograph.The expulsion time was recorded according to the time of the devices disappearing from X-ray photographs .
Bursting strength test
The bursting strength was measured by a sphygmomanometer.One end of anastomotic specimen was attached to the sphygmomanometer and submerged in water,and a catheter was introduced through the other end and hold in place by a tightened suture.For end-to-side anastomosis,the third end of specimen should be ligated with silk suture or clamped by hemostatic forcep.The intraluminal pressure was then gradually increased and the readings were recorded as air first bubble rise to the surface of the water.The maximum hydraulic pressure when the specimen ruptures,was recorded.
Pathological examination
At each time-point,6 canines (3 for end-to-end and 3 for end-to-side modalities) would be sacrificed in both groups,and anastomotic specimens were harvested.After gross observation,all samples were fixed in 10% formalin at pH 7.0 and processed according to standard histological procedures.Sections of 4–6 μm thickness were stained with haematoxylin and eosin.
Statistical analysis
Data were expressed as mean±SD.Differences between groups were analyzed by the Independent-Samples T Test,Mann-Whitney U Test,and Fisher’s Exact Test,respectively.In all of the tests,the significant level was set atP<0.05.
RESULTS
Anastomosis time
The mean anastomosis time of MCAs was significantly less than that of traditional hand-sewn method (8.50 ± 1.95vs.31.1 ± 4.32 minutes,P<0.001).The anastomosis time of end-to-side (7.80±2.17vs.30.90±4.28 minutes,P<0.001)and end-to-end intestinal anastomoses in the study group(9.20±1.48vs.31.20±4.60 minutes,P<0.001) was significantly shortened compared with the control group.Because two purse-string sutures required to fix two parts of MCAs,the anastomosis time of end-to-end anastomosis with MCAs was slightly longer than that of end-to-side anastomosis.
Postoperative complications
No intestinal obstruction and anastomotic stricture ocurred in both groups during the follow-up period.Four canines revealed blood stools with 2 animals in each group.The blood in the stool of three canines after hemostasis and gastric acid suppression therapy disappeared.One canine in the control group died on postoperative day 6 because of the descending colon hemorrhage,and autopsy revealed that multiple red-black punctate mucosal hemorrhages in the descending colon.In addition,another 3 canines died within one week after operation.Two canines died of jejunal intussusceptions located just at the site of the end-to-side jejunojejunal anastomosis.One of them received traditional hand-sewn and the other one underwent magnetic compression anastomosis.One canine in the study group died of anastomotic leakage because of failure of coupling.The total mortality rate of the 36 mongrel canines was 11% (2/18 in the study groupvs.2/18 in the control group) and the incidences of postoperative complications were 22% (4/18) and 16% (3/18) for the study and control groups respectively (P>0.05).
Expulsion time of MCAs
MCAs disappeared from X-ray photographs between 3 and 5 days postoperatively,and the mean time was 3.70±1.01 and 3.50±0.79 days for end-to-side subgroup and end-toend subgroup respectively (P>0.05).The necrotic tissue at the site of anastomotic ring formed by two kinds of techniques could be observed.HE staining manifested the tissue structures disappeared.
Bursting strength
The mean bursting strength was 133.6 ± 22.86 mm Hg in the study group and 91.2±18.47 mm Hg in the control group after 1 week’s follow-up (P<0.05).However,1 and 3 months after surgery,the bursting strengths of anastomotic specimens obtained from canine both in the control group and the study group were above 300 mm Hg.
Gross appearance of anastomosis
Gross appearance of the anastomosis from mongrel canines undergoing traditional hand-sewn was different from that receiving magnetic compression anastomosis (Fig.5).The mucosa at the anastomosis site constructed by MCAs was relatively smoother and flatter (Figs.5D,5E,5F),and it was hard to find the anastomotic line at the 3rd month after surgery (Fig.5F).The retained silk knots can be observed in the mucosa at the anastomosis site undergoing traditional hand-sewn during the follow-up period (Figs.5A,5B,5C).At 1 week after surgery,the retained suture knots were tightened,and the anastomotic line appeared red for foreign body reaction (Fig.5A).After 1 month,the suture retained in anastomosis became loose and disorderly (Fig.5B).After 3 months,almost all the suture knots disappeared from the mucosa (Fig.5C).
Histological appearance of anastomosis
The anastomosis in the study group (Figs.6D,6E,6F)seemed to heal much better and quicker than that in the control group (Figs.6A,6B,6C).Histological examination of the anastomoses in the study group revealed the mucus layer was continuous with a relatively smooth surface.There was an absence of the silk-related foreign body granulomas and slight infiltration of the inflammation cells in the muscular layer and serous layer.Healing was completed at the anastomosis in the study group by 3 months of follow-up,and there was continuity of serosal,submucosal,and mucosal layers without ischemia or necrosis (Fig.6F).
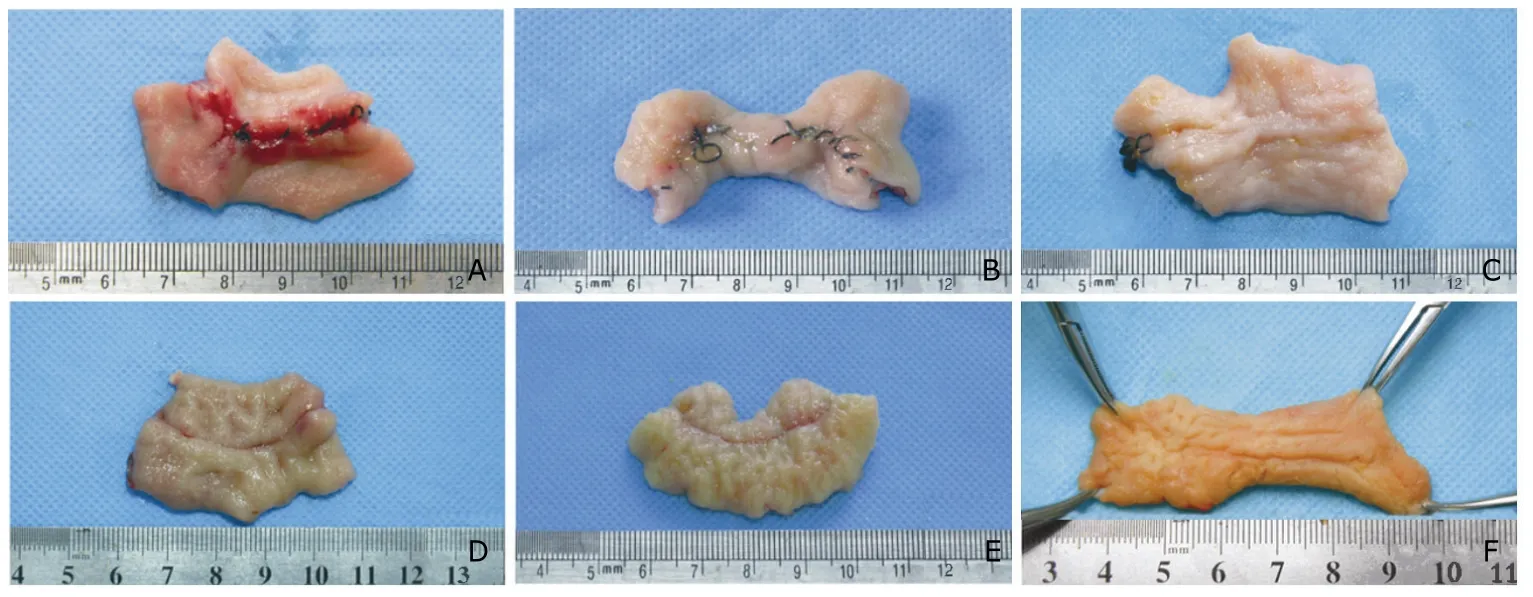
Figure 5.Gross images of the anastomoses from mongrel canines undergoing traditional hand-sewn (A,B,C) and magnetic compression anastomosis (D,E,F).
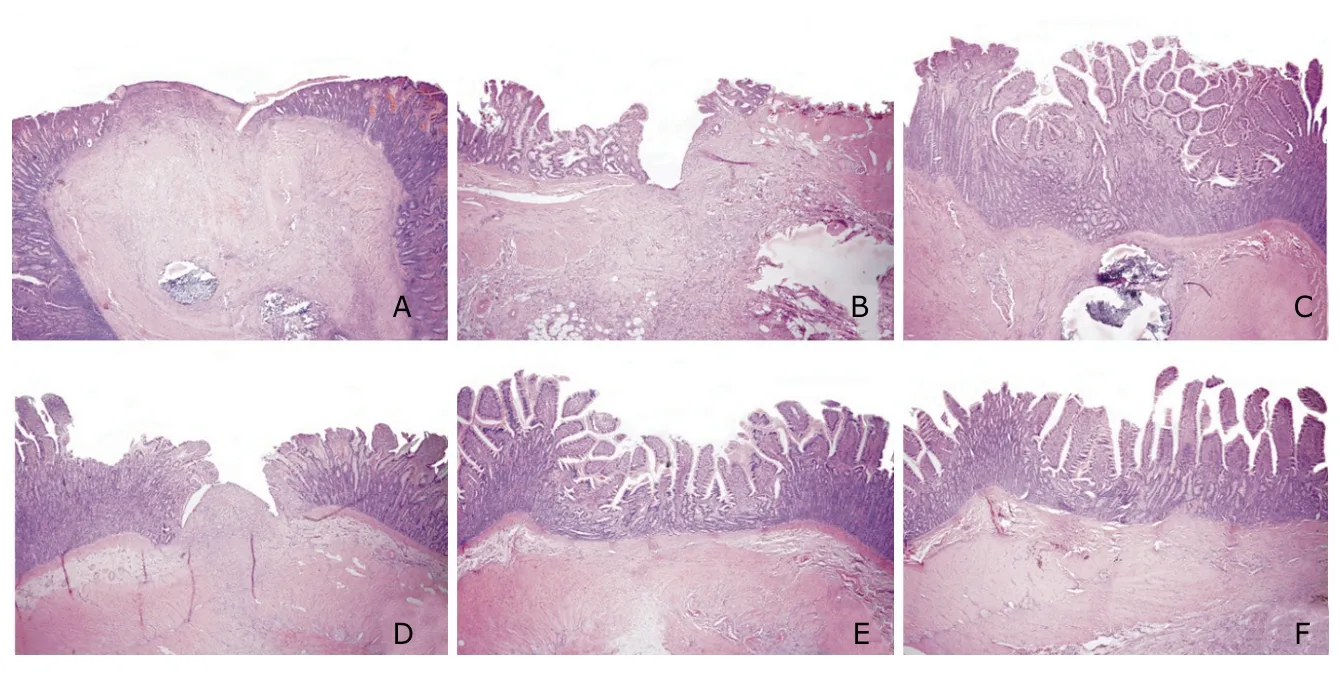
Figure 6.Histological images of the anastomosis from mongrel canines undergoing traditional hand-sewn (A,B,C) and magnetic compression anastomosis (D,E,F).HE ×40
DISCUSSION
Throughout two centuries’ history of intestinal construction,hand-sewn and stapled anastomosis have been two types of the most influential techniques.Although they have been widely used in clinical practice,they could not meet all criteria of ideal anastomotic technique,which should be easy and fast to be performed,feasible to be carried out at any time,easy to learn and to teach,safe,and as inexpensive as possible,most importantly,the constructed anastomosis should not contain any foreign materials.3,4
Magnamosis is one kind of compressive anastomosis technology,just like other compressive devices,which are used for connecting severed portions of hollow viscera to form sandwich.The magnamosis has been used to resolve certain clinical dilemmas in some case reports,5-7and it has been proved that the magnamosis is equivalent or superior to anastomoses created by traditional suture or staple techniques.8However,relative research on magnamosis was rare and the histological observation on anastomoses was seldom reported.In this study,we introduced one novel MCAs and certified the advantages in construction of the intestinal anastomoses over hand-sewn method.
The magnets of our MCAs are of sintered NdFeB,which is the third generation of rare earth permanent magnetic material,and have good cost/benefit ratio.The magnetic shields can concentrate the magnetic line of magnet on the polar region,where mother and daughter part would couple together.Such design of structure not only strengthens the bond between two parts,but also avoids the interaction of other part of anastomat.Thereafter,multiple anastomoses construction with such MCAs would be used without the worry of bowel leakage and fistula ocurring9-11when they pass through digestive tract.
A potential advantage of this technique is the costs.3,12The MCAs used in the experiment were manufactured by our partner,College of Mechanical Engineering,and the cost was controlled within 100 RMB.
According to our study,the duration difference in anastomotic construction between two groups was significant.The anastomosis time taken in MCAs group was within 6 minutes,which was less than one third of time taken in hand-sewn group,even comparable of circular stapler of 7.7 minutes (range,5 to 12 minutes).13The significantly shortened anastomotic time can not only reduce the possibility of infection,but also improve the survival rate of patients in emergency instances.
Leakage has happened in MCAs group.The reason was that we failed to identify the poles of the magnets when assembling the MCAs.Therefore,two parts of the MCAs rejected each other and could not couple together.Owing to nontechnical defect,such misadventure would be eliminated by professional manufacture of MCAs.
Although the incidences of mortality and morbidity after operation were similar between the control group and the study group,we still regarded the MCAs was much safer in intestinal anstomosis because bursting strength was significant higher measured in the study group at 1 week of follow-up,and early strengthened anastomosis with MCAs means fast wound healing and less risk to being anastomotic leakage.14In the control group,however,the suture produces a significant inflammatory response during lag phase and proliferation phase,and the activated bowel-wall collagenase degrades the collagen within the wound,eroding the foundation in which sutures are anchored.15Moreover,in remodeling phase,the silk suture can increase the risk of anastomotic stenosis16and limit the expansion of anastomosis with fluctuations of pressure,potentially induce the likelihood of obstruction.8
Although the magnamosis is safe and simple,the mucosal tears and failure of anastomat coupling still happened in the study group.Appropriate purse-string suture should never be underestimated during the operation,and the stitch distance should be 2.5-3 mm and border distance should be 1.5-2 mm in this procedure.The successful purse-string suture makes the stump edges around the central duct of mother part without mucosal tearing,and guarantees the watertight compression of intestinal stumps in MCAs without leakage happening.The Prolene was recommended in purse-string suture because of its smooth surface and high fracture strength.Accurate coupling of the two parts of MCAs can prevent misadventures in alignment and orientation.To make the parallel coupling of the two parts of anastomat during anastomosis,the abdominal X-ray examination routinely taken after operation should always keep in mind.One case of dislocation of anastomat was identified upon X-ray on the 2nd day postoperatively.Fortunately,there was no bowel leakage and the anastomat was not still retainedin situ.After a slightly adjustment,the anastomat was found in the feces in next day and the canine was uneventful in the following days.
By virtue of small size and simple application,if relative auxiliary tools,such as purse-string suture clamp and MCAs holding device could be used at the same time,the standardization of magnamosis with MCAs would be improved a lot,and the clinical application in intestinal anatomosis would be much easier.Thereafter,the MCAs can be introduced by digestive endoscopy,percutaneous and laparoscopic techniques,and even natural orifice transluminal endoscopic surgery.
In short,as we have already proved in the experiment,the novel MCAs not only meet the requirements of intestinal anastomosis:hemostatic,circumferentially air-tight,and having inverted edges,17but also have the advantage of simple manufacturing,cheap price,shortened healing duration,minor inflammation and excellent alignment of wall layers,which make the magnanosis nearly an ideal modality and should be introduced in clinical application as soon as possible.
ACKNOWLEDGEMENTS
We thank all members of Surgical Dream Works for their assistance.
1.Buchberg BS,Masoomi H,Bergman H,et al.The use of a compression device as an alternative to hand-sewn and stapled colorectal anastomoses:is three a crowd? J Gastrointest Surg 2011;15:304-10.
2.Lim CBB,Goldin RD,Darzi A,et al.Characterization of materials eliciting foreign body reaction in stapled human gastrointestinal anastomoses.Br J Surg 2008;95:1044-50.
3.Pahlman L,Ejerblad S,Graf W,et al.Randomized trial of a biofragmentable bowel anastomosis ring in high-risk colonic resection.Br J Surg 1997;84:1291-4.
4.Thiede A,Geiger D,Dietz UA,et al.Overview on compression anastomoses:biofragmentable anastomosis ring multicenter prospective trial of 1666 anastomoses.World J Surg 1998;22:78-87.
5.Zaritzky M,Ben R,Zylberg GI,et al.Magnetic compression anastomosis as a nonsurgical treatment for esophageal atresia.Pediatr Radiol 2009;39:945-9.
6.Marubashi S,Nagano H,Yamanouchi E,et al.Salvage cystic duct anastomosis using a magnetic compression technique for incomplete bile duct reconstruction in living donor liver transplantation.Liver Transp 2010;16:33-7.
7.Ashikawa K,Komoriyama H,Kumano R,et al.Magnetic compression anastomosis for rectal anastomotic stenosis:report of a case.Br J Surg 2010;97:S79-S80.
8.Jamshidi R,Stephenson JT,Clay JG,et al.Magnamosis:magnetic compression anastomosis with comparison to suture and staple techniques.J Pediatr Surg 2009;44:222-8.
9.Honzumi M,Shigemori C,Ito H,et al.An intestinal fistula in a 3-year-old child caused by the ingestion of magnets:report of a case.Surg Today 1995;25:552-3.
10.Oestreich AE.Worldwide survey of damage from swallowing multiple magnets.Pediatr Radiol 2009;39:142-7.
11.Pryor HI,Lange PA,Bader A,et al.Multiple magnetic foreign body ingestion:a surgical problem.J Am Coll Surg 2007;205:182-6.
12.Galizia G,Lieto E,Castellano P,et al.Comparison between the biofragmentable anastomosis ring and stapled anastomoses in the extraperitoneal rectum:a prospective,randomized study.Int J Colorectal Dis 1999;14:286-90.
13.White RN.Modified functional end-to-end stapled intestinal anastomosis:technique and clinical results in 15 dogs.J Small Anim Pract 2008;49:274-81.
14.Wang Y,Cai X,Cai H,et al.Experimental study of colonic anastomosis with a degradable stent in a porcine model.Am J Surg 2010;199:833-9.
15.Ballantyne GH.The experimental basis of intestinal suturing—effect of surgical technique,inflammation,and infection on enteric wound-healing.Dis Colon Rectum 1984;27:61-71.
16.Owens MW,Grisham MB.Cytokines increase proliferation of human intestinal smooth-muscle cells—possible role in inflammation-induced stricture formation.Inflammation 1993;17:481-7.
17.Kaidar-Person O,Rosenthal RJ,Wexner SD,et al.Compression anastomosis:history and clinical considerations.Am J Surg 2008;195:818-26.
 Chinese Medical Sciences Journal2011年3期
Chinese Medical Sciences Journal2011年3期
- Chinese Medical Sciences Journal的其它文章
- Sclerosing Cholangitis after Transcatheter Arterial Chemoembolization:a Case Report
- Choroidal Tuberculoma in an ImmunocompetentYoung Patient
- Influence of Deleted in Colorectal Carcinoma Gene on Proliferation of Ovarian Cancer Cell Line SKOV-3 In Vivo and In Vitro
- Cytogenetic and Clinical Analysis of 340 Chinese Patients with Primary Amenorrhea
- Serum HIF-1α and VEGF Levels Pre-and Post-TACE in Patients with Primary Liver Cancer
- Effect of Multiple Coatings of One-step Self-etching Adhesive on Microtensile Bond Strength to Primary Dentin