
Nocturnal hypertension and riser pattern are associated with heart failure rehospitalization in patients with heart failure with preserved ejection fraction
2023-07-29 13:31:16GangHUANGXiaoHanLIUYueZHANGYuXinZHUYunHETianBoWANGZhenZHANGJunBoXU
Journal of Geriatric Cardiology 2023年6期
Gang HUANG?, Xiao-Han LIU, Yue ZHANG, Yu-Xin ZHU, Yun HE Tian-Bo WANG, Zhen ZHANG Jun-Bo XU?
1.Department of Cardiology, the Third People’s Hospital of Chengdu, Sichuan, China; 2.Cardiovascular Disease Research Institute of Chengdu, Sichuan, China; 3.Affiliated Hospital of Southwest Jiaotong University, Sichuan, China; 4.The Second Affiliated Chengdu Clinical College of Chongqing Medical University, Sichuan, China
ABSTRACT BACKGROUND Nocturnal hypertension is reported as a risk factor for cardiovascular disease.This study aimed to explore the potential association between nocturnal hypertension and heart failure (HF) rehospitalization in patients with HF with preserved ejection fraction (HFpEF).METHODS A total of 538 patients with HFpEF from May 2018 to December 2021 were consequently recruited in this study and followed up until they were readmitted for HF or the end of this study.Cox regression analysis was used to reveal the potential association between nighttime blood pressure (BP) levels, nocturnal hypertension and nocturnal BP patterns and HF rehospitalization.Kaplan-Meier curve was used to assess the cumulative event-free survival rate between groups.RESULTS There were 537 patients with HFpEF were included in the final analysis.The mean age of the study population was 77.14 ± 8.68 years, and 41.2% of patients were men.After a median follow-up duration of 10.93 (4.19–21.13) months, 176 patients(32.7%) with HFpEF were readmitted for HF.Cox regression analysis had revealed that nighttime systolic BP level [hazards ratio(HR) = 1.018, 95% CI: 1.008–1.028, P = 0.001], nighttime diastolic BP level (HR = 1.024, 95% CI: 1.007–1.042, P = 0.007), nocturnal hypertension (HR = 1.688, 95% CI: 1.229–2.317, P = 0.001) were associated with HF rehospitalization.Kaplan-Meier analysis had demonstrated that patients with nocturnal hypertension had significantly lower event-free survival rate (log-rank P < 0.001).Furthermore,patients with a riser pattern had a higher risk of HF rehospitalization (HR = 1.828, 95% CI: 1.055–3.166, P = 0.031) and lower eventfree survival rate (log-rank P = 0.003) than those with a dipper pattern.These findings were also confirmed in patients with HFpEF and hyperuricemia.CONCLUSIONS Nighttime BP levels, nocturnal hypertension and a riser pattern are independently associated with HF rehospitalization in patients with HFpEF, and prominently in patients with HFpEF and hyperuricemia.Well controlled nighttime BP levels should be emphasized and considered in patients with HFpEF.
Heart failure (HF) is nowadays becoming a big clinical challenge worldwide with increasing number as the end stage of most cardiovascular diseases, albeit new medications and device-based therapies have been introduced into the treatment of HF continuously for decades.It is reported that the generally estimated prevalence of HF is 1%–2% in general adults in developed countries,[1]and approximately 1.3% in Chinese adults aged ≥ 35 years.[2]However, the absolute number of patients with HF has been consistently increasing, as a result of global population growth, aging and improved survival benefited from advanced medical treatment.The mortality and rehospitalization rate of HF vary from observational and clinical trials.A meta-analysis has reported that the estimated one-year, five-year and ten-year mortality of all HF were about 13.5%, 43.3% and 65.1%, respectively.[3]And another meta-analysis has found that the one-year mor-tality and HF rehospitalization rates were 43.7% and 44.1%, 37.5% and 34.5%, and 47.3% and 38.2% in patients with HF with reduced ejection fraction (HFrEF), HF with middle-ranged ejection fraction and HF with preserved ejection fraction (HFpEF), respectively.[4]
HFpEF accounts for more than half of all HF cases.[5]Moreover, it has been generally considered as a heterogeneous syndrome with different clinical phenotypes,which results in difficulties in diagnosing and understanding its pathophysiological mechanism and prognostic characteristics.Hypertension is one of the most important risk factors for HF and especially it is one of the most common causes of HFpEF.The Treatment of Preserved Cardiac Function Heart Failure with an Aldosterone Antagonist (TOPCAT) study[6]has demonstrated that low diastolic blood pressure (BP) was associated with short-term and long-term mortality in patients with HFpEF.Ambulatory BP monitoring (ABPM)is widely used to investigate the circadian BP rhythm and assess the effects of antihypertensive treatment in patients with hypertension.Nighttime diastolic BP (DBP) and non-dipping BP have been shown to be predictors of chronic HF.[7]And nighttime BP levels and riser pattern have been found to be risk factors for cardiovascular events in Japanese hypertensive patients.[8]
Traditional prognostic factors for outcomes of HFpEF have been somewhat well described, while the potential role of nocturnal hypertension and nighttime BP pattern in HFpEF have not been fully investigated.Hence, this study aimed to explore the potential association between nocturnal hypertension and nighttime BP pattern and clinical outcomes in patients with HFpEF.
METHODS
Study Population
Hospitalized patients aged more than 18 years and diagnosed with HFpEF were included.Patients suffered from acute coronary syndrome in three months, severe valvular heart disease, malignant disease and on hemodialysis or in unstable hemodynamic status were excluded.A total of 538 patients with HFpEF were consequently included in this retrospective observational study.The protocol of this study conforms to the ethical guidelines outlined in the 1975 Declaration of Helsinki and was command approved by the Institutional Review Board of the Third People’s Hospital of Chengdu (No.2022-S-55) in Sichuan, China.
Definitions and Measurements
Hypertension was defined as clinic office systolic BP(SBP) ≥ 140 mmHg and/or DBP ≥ 90 mmHg and/or self-reported treatment of hypertension with antihypertensive medication in the last two weeks according to the Chinese Guidelines for Prevention and Treatment of Hypertension.[9]
Nocturnal hypertension was defined as a nighttime SBP ≥ 120 mmHg and/or nighttime DBP ≥ 70 mmHg based on the Chinese Guidelines for Prevention and Treatment of Hypertension.[9]The nighttime BP dipping was defined as (one min average nighttime SBP/average daytime SBP) × 100%.And the patterns of the nocturnal BP dipping were classified into three patterns: (1) the dipper pattern with the nighttime BP dipping more than 10%; (2)the non-dipper pattern with the nighttime BP dipping between 0 and 10%; and (3) the riser pattern with the nighttime BP dipping less than 0.Since there was limited cases(n= 4) with an extreme dipper pattern (nighttime BP dipping more than 20%), patients with an extreme dipper pattern were classified into those with the dipper pattern for analysis.
ABPM was performed during the first hospitalization by an automatic system with electrical cuff inflation (CF-3001, Chengdu Langrui Medical Science Co., Ltd), which measured SBP and DBP every half an hour during daytime (from 06:00 to 22:00) and every one hour during nighttime (from 22:00 to 06:00) in this study.BP measurement was performed on the opposite side of the dominant arm.Valid 24-hour ABPM recordings comprised those with > 70% of the total BP records, a minimum of twenty-four daytime BP readings, and a minimum of seven nighttime BP readings.[10]
HFpEF was diagnosed based on symptoms, sings and serum biomarker according to the European Society of Cardiology and Chinese guidelines.[11,12]
HF rehospitalization was defined as any rehospitalization during which HF was listed as one primary diagnosis based on typical HF symptoms, signs and increased B-type natriuretic peptide levels for which intravenous diuretics or increased dose of loop diuretics were needed in clinic.
Hyperuricemia was defined as the levels of serum uric acid > 416 μmol/L (7.0 mg/dL) for men and > 357 μmol/L(6.0 mg/dL) for women or if patients with a definite history of hyperuricemia were on allopurinol, benzbromarone or febuxostat therapy.
Follow-up and Outcomes
Patients were followed up until they were readmitted for HF or until May 2022 by researchers through checking the electronic medical records or telephone interview.
Statistical Analysis
Continuous variables and frequencies are expressed as mean ± SD and counts (percentages), respectively.The Student’st-test was used to compare the difference of continuous variables between groups (Kruskal-Wallis test for skewed data) and the Pearson’s chi-squared test was used to compare the difference of frequencies between groups.The Kaplan-Meier analysis (log-rank test)was used to estimate the cumulative incidence of HF rehospitalization between groups.The Cox proportional hazards regression analysis was used to assess the potential associations between nocturnal SBP, nocturnal DBP,nocturnal hypertension, nocturnal BP pattern and HF rehospitalization.All statistical analyses were performed with SPSS 22.0 (SPSS Inc., IBM, Armonk, NY, USA).TwosidedP-value < 0.05 were considered statistically significant.
RESULTS
Baseline Characteristics
There were 537 patients with HFpEF were included in the final analysis.The mean age of all patients was 77.14± 8.68 years and 58.8% of patients were women.More than 77% and 41% of all patients had a history of hypertension and coronary artery disease, respectively.The mean office SBP/DBP and 24-hour ambulatory SBP/DBP levels were 134.93 ± 23.06 mmHg/75.07 ± 13.30 mmHg and 124.03 ± 15.29 mmHg/73.08 ± 8.59 mmHg, respectively.About 37.4% of all patients with HFpEF had nocturnal hypertension.Compared with patients without nocturnal hypertension, patients with nocturnal hypertension were significantly older and had significantly higher body mass index (BMI), office SBP level, 24-hour ambulatory BP levels, daytime and nighttime ambulatory BP levels (Table 1).About 41.2% of patients with HFpEF had a riser pattern.There was no significant difference of office SBP/DBP levels between patients with a dipper pattern and those with a riser pattern of nocturnal hypertension (P= 0.086 andP= 0.280, respectively).However,patients with a riser pattern had significantly lower daytime ambulatory SBP/DBP levels (P= 0.001 andP<0.001, respectively) while higher nighttime ambulatory SBP/DBP levels (bothP< 0.001, Table 2).
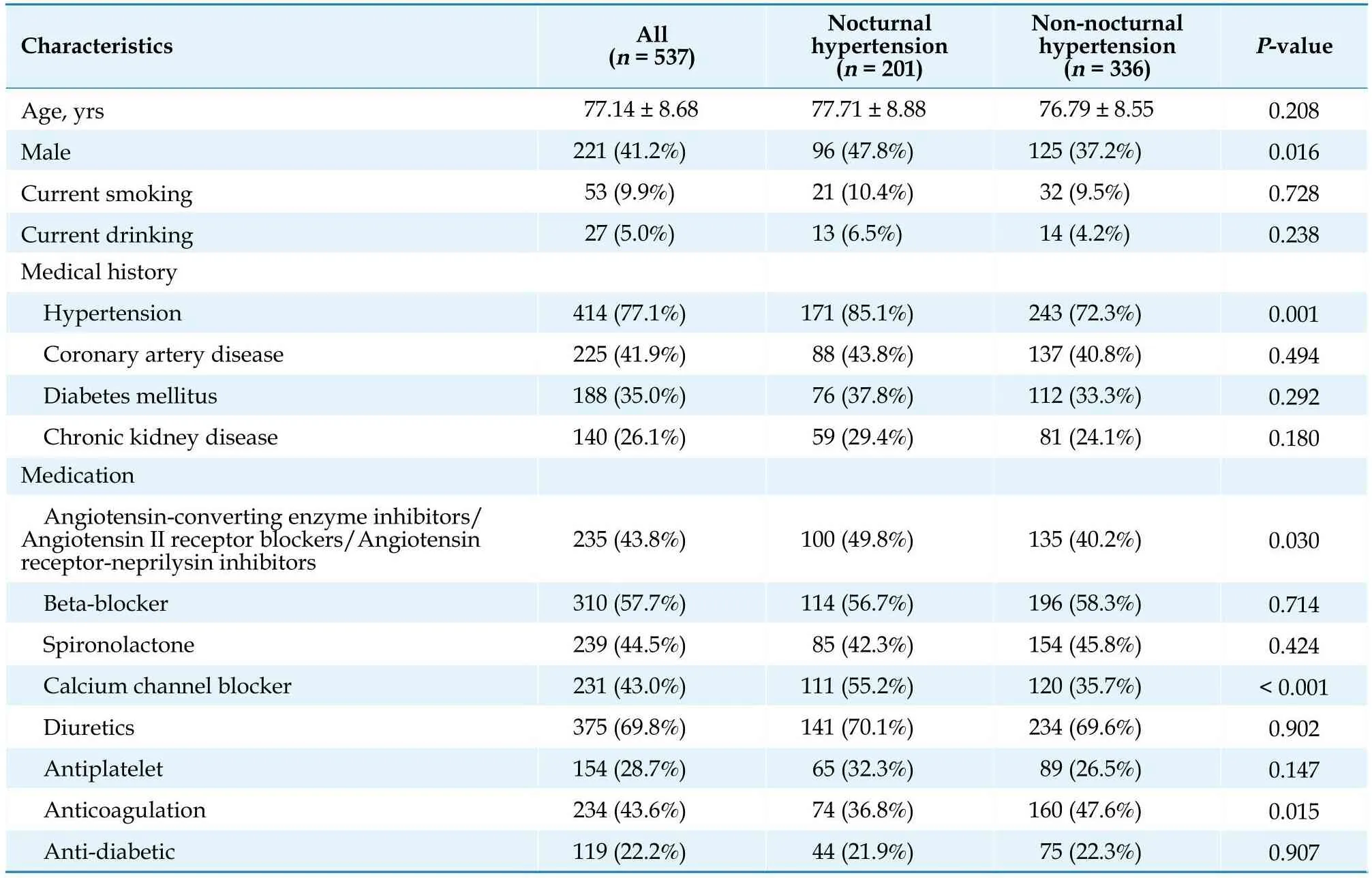
Table 1 Baseline characteristics of patients with heart failure with preserved ejection fraction by nocturnal hypertension.

Table 2 Baseline characteristics of patients with heart failure with preserved ejection fraction by nocturnal blood pressure pattern.
Nocturnal Hypertension in HFpEF
Cox regression analysis was used to reveal the potential association between nocturnal BP and HF rehospitalization in patients with HFpEF.These statistical analyses have found that the nighttime SBP level [hazards ratio (HR) = 1.016,P= 0.001], the nighttime DBP level (HR =1.018,P= 0.031) and nocturnal hypertension (HR = 1.620,P= 0.031) were significantly associated with HF rehospitalization, respectively.After adjusting for age, history of hypertension, history of diabetes mellitus (DM), BMI,blood urea nitrogen (BUN), estimated glomerular filtration rate (eGFR) and hemoglobin, Cox regression analysis has also found that the nighttime SBP level (HR =1.018,P= 0.001), the nighttime DBP level (HR = 1.024,P=0.007) and nocturnal hypertension (HR = 1.688,P= 0.001)were significantly associated with HF rehospitalization(Table 3).

Table 3 Cox regression analysis of nocturnal blood pressure in patients with heart failure with preserved ejection fraction.
Since patients with nocturnal hypertension had approximately 69% higher risk of HF rehospitalization than those without nocturnal hypertension, the associations between different nocturnal BP patterns and HF rehospitalization were further analyzed.In these Cox models,nocturnal hypertension pattern (HR = 1.278,P< 0.001)was found to be associated with HF rehospitalization, and furthermore, patients with a riser pattern (HR = 2.253,P= 0.004) had a significantly higher risk of HF rehospitalization than those with a dipper pattern.After adjusting for age, history of hypertension, history of DM, BMI, BUN,eGFR and hemoglobin, nocturnal hypertension pattern(HR = 1.168,P= 0.028) was still associated with HF rehospitalization in patients with HFpEF and patients with a riser pattern (HR = 1.828,P= 0.031) were more likely to be readmitted for HF than those with a dipper pattern(Table 4).

Table 4 Cox analysis of nocturnal blood pressure pattern in patients with heart failure with preserved ejection fraction.
The median follow-up duration was 10.93 (4.19–21.13)months, and 176 patients (32.7%) with HFpEF were readmitted for HF.In patients with HFpEF, the Kaplan-Meier analysis has revealed that patients with nocturnal hypertension had a significantly lower event-free survival rate than those without nocturnal hypertension (25.5% ±11.3%vs.40.6% ± 8.2%,P< 0.001) (Figure 1A).Furthermore, patients with a riser pattern had a significantly lower event-free survival rate than those with a dipper pattern(28.4% ± 7.2%vs.50.7% ± 15.3%,P= 0.003) or a non-dipper pattern (28.4% ± 7.2%vs.44.6% ± 13.3%,P= 0.005)(Figure 2A).
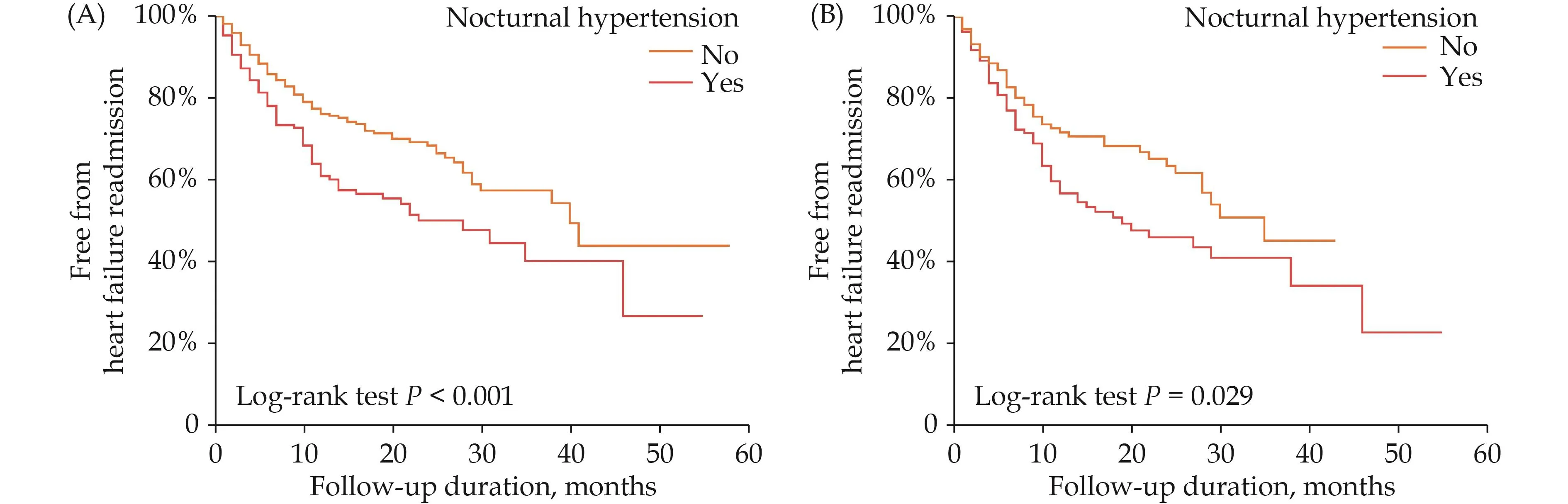
Figure 1 Survival curves by nocturnal hypertension in patients with HFpEF (A) and in patients with HFpEF and hyperuricemia(B).HFpEF: heart failure with preserved ejection fraction.
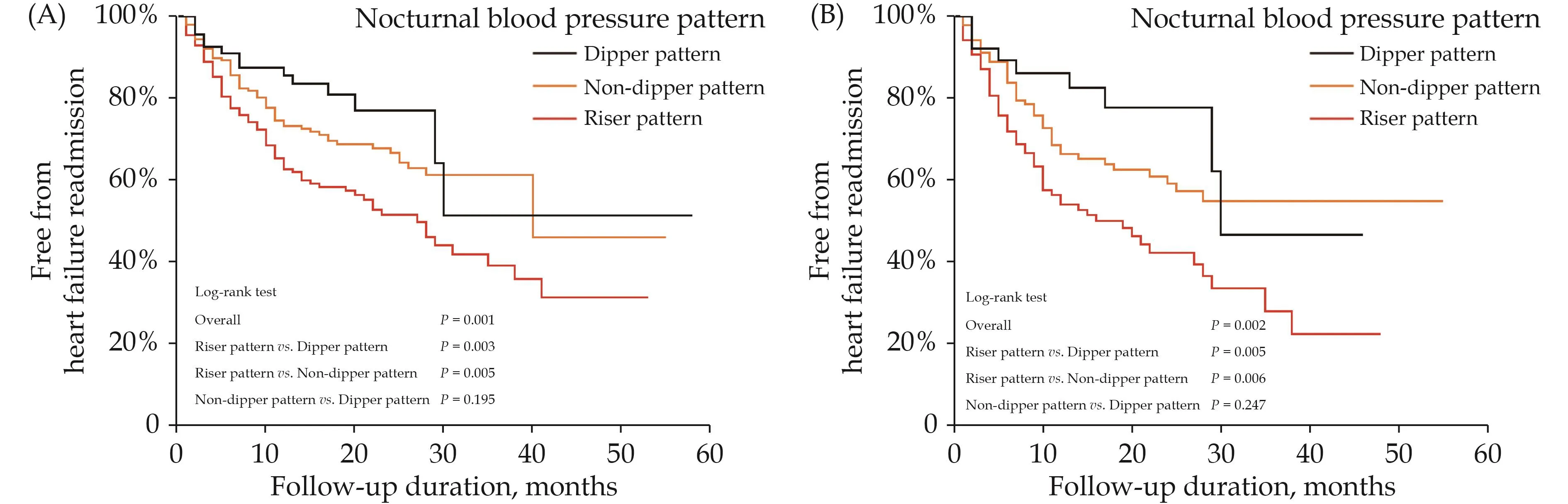
Figure 2 Survival curves by nocturnal blood pressure pattern in patients with HFpEF (A) and in patients with HFpEF and hyperuricemia (B).HFpEF: heart failure with preserved ejection fraction.
Nocturnal Hypertension in HFpEF and Hyperuricemia
Hyperuricemia has been shown to be associated with cardiovascular diseases.Therefore, subgroup analysis were performed in patients with HFpEF and hyperur-icemia (n= 310).Consistently, Cox regression analysis have found the nighttime SBP level (HR = 1.018,P=0.003), the nighttime DBP level (HR = 1.027,P= 0.010) and nocturnal hypertension (HR = 1.594,P= 0.050) were all associated with HF rehospitalization.After adjusting for age, history of hypertension, history of DM, BMI, BUN,eGFR and hemoglobin, nocturnal SBP (HR = 1.019,P=0.003), nocturnal DBP (HR = 1.024,P= 0.028) and nocturnal hypertension (HR = 1.805,P= 0.004) were still associated with HF rehospitalization (Table 5).Moreover,Cox regression analysis have also found that nocturnal hypertension pattern (HR = 1.278,P< 0.001) was associated with HF rehospitalization.Compared to dipper pattern, patients with a riser pattern (HR = 2.501,P= 0.007)had 1.5-fold increased risk of HF rehospitalization.After adjusting for age, history of hypertension, history of DM,BMI, BUN, eGFR and hemoglobin, nocturnal hypertension pattern (HR = 1.236,P= 0.013) and riser pattern (HR =2.038,P= 0.039) were still significantly with an increased risk of HF rehospitalization (Table 6).

Table 5 Cox regression analysis of nocturnal blood pressure in patients with heart failure with preserved ejection fraction and hyperuricemia.

Table 6 Cox analysis of nocturnal blood pressure pattern in patients with heart failure with preserved ejection fraction and hyperuricemia.
In patients with HFpEF and hyperuricemia, consistently, the Kaplan-Meier analysis has revealed that patients with nocturnal hypertension had a lower event-free survival rate than those without nocturnal hypertension(23.0% ± 10.6%vs.36.4% ± 9.4%,P= 0.029) (Figure 1B).Furthermore, patients with a riser pattern had a significantly lower event-free survival rate than those with a dipper pattern (21.2% ± 7.4%vs.46.2% ± 17.5%,P= 0.005)or a non-dipper pattern (21.2% ± 7.4%vs.53.0% ± 5.6%,P= 0.006) (Figure 2B).
DISCUSSION
Main Findings
The main findings of this study are as follows: (1) the nighttime SBP and DBP levels are associated with HF rehospitalization in patients with HFpEF; (2) nocturnal hypertension and a riser pattern are associated with HF rehospitalization in patients with HFpEF; and (3) nocturnal hypertension and a riser pattern are prominently asso-ciated with HF rehospitalization in patients with HFpEF and hyperuricemia.
Hypertension is one common comorbility in patients with HF, especially in HFpEF.Therefore, HFpEF is widely considered as a hypertensive phenotype.It has been reported that more than 50% of patients with HFpEF suffer from hypertension,[13,14]and the rate of hypertensive patients in our study was a little higher.In the Swedish HF study, resistant hypertension was found to be most common in patients with HFpEF with an estimated prevalence of 17%.[15]This study[15]has also demonstrated that resistant hypertension is related with a lower first-time HF rehospitalization and cardiovascular mortality in patients with HF with reduced and mildly reduced EF while not in HFpEF, which is consistent with the current evidence that HFpEF has been considered as a syndrome with apparent phenotypic heterogeneity.
Nocturnal Hypertension in HFpEF
Although a number of treatment approaches have been introduced in the management of HF, approximately 20% of patients with HF would be rehospitalized in the first month after discharge.[16]And particularly, the longterm survival rate of HF remains similar with or even lower than those of some malignant carcinomas.[17]Furthermore, current new medication or device-based therapy focus mostly on patients with HFrEF and there is until now no widely accepted treatments for patients with HFpEF with different clinical phenotypes.The HF rehospitalization rate in this study population was similar high compared to that in other studies,[6,13,14]which was a main burden decreasing the quality of life of patients with HF.There is growing evidence showing that the nighttime BP level and nocturnal hypertension can predict cardiovascular outcomes,[18]and have a better ability than the office BP level.In accordance with findings in Swedish HF study,[15]we have not found that the office BP, daytime BP and 24 h average BP levels were associated with HF rehospitalization in this study population with HFpEF, which implying the office BP, daytime BP and 24 h average BP levels could only partly reflect the whole influence of BP on HF rehospitalization in patients with HFpEF.Nevertheless, the nighttime SBP and DBP levels are significantly associated with HF rehospitalization.The office BP levels are associated with development of the left ventricular hypertrophy in mild hypertension and usually decades after the onset of hypertension, treated hypertension can gradually proceed to HF.The importance of nocturnal hypertension are usually underestimated since it can add more prognostic information in treated hypertensive patients.[8]Furthermore, in line with previous studies,[7,8]nocturnal hypertension has shown to be associated with HF reshospitalization.These results may also benefit from the advantage of ABPM, by which the nighttime BP measurements may be better standardized and less influenced by physical activities.
Despite the prognostic importance of nocturnal hypertension in this study population with HFpEF, our study has also demonstrated that nocturnal BP pattern is significantly associated with an increased risk for HF rehospitalization, which are consistent with previous studies.[19,20]Compared to a dipper pattern, a riser pattern is significantly associated with an approximately 83% increased risk for HF rehospitalization, while non-dipper pattern is not significantly associated with this risk.One previous observational study including 6359 patients with at least one cardiovascular risk factor (93% of patients with hypertension) has demonstrated that the nighttime SBP level and a riser pattern increase the risk of new onset HF in Japanese patients.[8]Another study with a mean follow-up duration of 30 months, including 325 patients with a baseline history of decompensated HF, has also revealed that a riser pattern was significantly associated with all cause and cardiovascular deaths in patients with HFpEF, whereas not in patients with HFrEF.[20]A riser pattern of nocturnal hypertension has been proven to be significantly associated with all-cause mortality in hemodialysis patients with a HR of 2.31.[21]
The potential mechanism underlying the nocturnal hypertension and HF may relate to abnormal sodium exertion by the kidney and impaired nocturnal sympathovagal balance,[18]which could increase the preload and afterload of the heart and result in cardiac morphological and functional remodeling and development of HF.A riser or non-dipper pattern of nocturnal hypertension has been shown to be associated with increased circulating volume influenced by salt intake and individual slat sensitivity.Nevertheless, limiting salt intake and diuretics are more effectively to reduce the nighttime BP than daytime BP levels, and to shift a non-dipper pattern to a dipper pattern of the circadian BP pattern.[22]Since increased BP levels promote a pressure natriuresis, corresponding elevated daytime and nighttime BP levels are needed to effectively exert excess sodium in patients with increased circulating volume.[22]This may be a reasonable explanation for the dyspnea symptom in hypertensive patients with HFpEF.Nighttime BP are usually measured in a supine position and therefore this body position may somewhat contribute to nocturnal hypertension.In a supine position at night, both accumulated peripheral interstitial fluid during the day reenters the circulation at night and increased venous return from the peripheral extremities to the heart can increase left ventricular preload and cardiac stress and therefore result in secreting of natriuretic peptides[23]and trigger acute decompensated HF events during sleep in patients with HFpEF.Moreover, it has been shown that increased activity of sympathetic nervous system at night are associated with the development of HF in hypertensive patients with a riser or non-dipper pattern.[24,25]
Nocturnal Hypertension in Patients with HFpEF and Hyperuricemia
Not surprisingly, in accordance with the findings in patients with HFpEF in this study, we have also found that nocturnal hypertension and a riser pattern were significantly associated with HF rehospitalization in patients both with HFpEF and hyperurecemia.Hyperurecemia has been proven to be associated with cardiovascular diseases in different cohort.Our previous studies have shown that hyperurecemia are associated with atrial fibrillation[26]and metabolic syndrome[27]in Chinese elderly, and cardiovascular diseases clustering among Chinese elderly women.[28]These findings in population with HFpEF with different common comorbilities imply a potential relationship between hyperurecemia and HFpEF.The average age of this study population was nearly 78 years,which was similar with that in the study population in previous studies.[7,20]The EMPEROR-reduced study has found that hyperurecemia is common and associated with more severe disease status in HFrEF.Furthermore, elevated serum uric acid level was an independent predictor of all-cause and cardiovascular mortality and HF hospitalization.[29]Not surprisingly, hyperurecemia is comorbid with more than half of patients with acute decompensated HFpEF and associated with HF rehospitalization and death.[30]It has also been reported that patients with HFpEF and hyperurecemia or gout had a significantly higher first and recurrent all cause hospitalization[31]and increased plasma xanthine oxidoreductase activity has also been reported to be significantly associated with adverse cardiovascular events in patients with HFpEF.[32]All patients with HFpEF are easily comorbid with hypertension and hyperurecemia.Therefore, our study has further analyzed the potential association between nocturnal hypertension and HF rehospitalization in the setting of HFpEF and hyperurecemia and also found that the nighttime BP levels and nocturnal hypertension are also associated with an even higher increased risk of HF rehospitalization than in general patients with HFpEF.These findings emphasize the importance of urgent intervention of nocturnal hypertension and especially those with a riser pat-tern particularly in patients with HFpEF and hyperurecemia.
The treatment strategies for HFrEF is well established and updated continuously, while no evidence based specific and effective therapeutic strategies for HFpEF has been established.[11]The recommended therapies for patients with HFpEF include symptom relieving and treatment of comorbid diseases, especially hypertension.And in hypertensive patients with HFpEF, the BP lowering therapy is an essential and important attempt to decrease HF rehospitalization and cardiovascular mortality.Except for the morning BP level as a treatment target, nighttime BP is also suggested to be considered as another target to maintain a normal circadian rhythm and further improve the BP control and reduce target organ damage and mortality.Potential choices may include diuretics, sodium-glucose cotransporter 2 inhibitor and angiotensin receptor neprilysin inhibitors.This study has revealed the important role of the nighttime BP levels, nocturnal hypertension and the riser pattern as indicators for HF rehospitalization in general patients with HFpEF and in subgroup patients with hyperurecemia.Therefore, the results of this study may facilitate the acknowledgment of nocturnal hypertension in patients with HFpEF and provide a new treatment strategy for HFpEF.
LIMITATIONS
There were several limitations in this study.On the one hand, this is a retrospective study, results of this study should be interpreted with caution.On the other hand, the ABPM was performed during hospitalization, which may not always represent the out clinic daily life of patients with HFpEF.
CONCLUSIONS
The nighttime BP levels, nocturnal hypertension and a riser pattern are predictors of HF rehospitalization in patients with HFpEF.These findings in this study suggest that a proper strategy of nighttime BP control in patients with HFpEF is urgently needed.
ACKNOWLEDGMENTS
This study was supported by the Department of Human Resources and Social Security of Sichuan Province (No.2021-11), the Chengdu Municipal Health Commission (No.2021200 & No.2022392), the Science and Technology Bureau of Chengdu (2019-YF05–00523-SN), and the Fundamental Research Funds for the Central Universities (No.2682022ZTPY029 & No.2682021ZTPY026).All authors had no conflicts of interest to disclose.
 Journal of Geriatric Cardiology2023年6期
Journal of Geriatric Cardiology2023年6期
- Journal of Geriatric Cardiology的其它文章
- Status of cardiovascular disease in China
- Unraveling the mechanisms of a giant coronary sinus
- Iatrogenic pneumopericardium after therapeutic pericardiocentesis for pericardial effusion: a case report
- Target versus sub-target dose of renin–angiotensin system inhibitors on survival in elderly patients with heart failure with reduced ejection fraction: a systematic review and meta-analysis
- Outcomes of catheter-directed thrombolysis versus systemic thrombolysis in the treatment of pulmonary embolism: a metaanalysis
- Down-regulation of the Smad signaling by circZBTB46 via the Smad2-PDLIM5 axis to inhibit type I collagen expression