
Polymorphic ventricular tachycardia during phase II cardiac rehabilitation in a patient with heart failure: a case report
2020-02-11 14:48:20HeeEunChoiChulKimSeHeumParkDooIlKimKiHunKimDongKieKimSeunghwanKimJinoPark
Journal of Geriatric Cardiology 2020年1期
Hee-Eun Choi, Chul Kim, Se-Heum Park,#, Doo-Il Kim, Ki-Hun Kim, Dong-Kie Kim,Seunghwan Kim, Jino Park
1Department of Rehabilitation Medicine, Inje University College of Medicine, Haeundae Paik Hospital, Busan, South Korea
2Department of Rehabilitation Medicine, Inje University College of Medicine, Sanggye Paik Hospital, Seoul, South Korea
3Department of Internal Medicine, Inje University College of Medicine, Haeundae Paik Hospital, Busan, South Korea
Keywords: Cardiac rehabilitation; Heart failure; Ventricular tachycardia
A 67-year-old man with a history of a prior cardiac arrest with ventricular fibrillation (VF) due to myocardial infarction underwent phase I (inpatient) and II (outpatient) cardiac rehabilitation (CR) exercise training. On the 33thCR session,15 min after the start of exercise training, the patient had syncope with evidence of a polymorphic and wide QRS complex tachycardia on electrocardiogram (ECG) monitoring. The initiation of a polymorphic ventricular tachycardia was evidenced by the coupled premature ventricular complex observed in the ECG monitoring screen (Figure 1).Subsequently, arrhythmia was detected, with a progressive change and twisting pattern in the morphology of the QRS complexes, followed by an almost disorganized activity rapidly leading to VF. We immediately started cardiopulmonary resuscitation (CPR) followed by intravenous infusion of epinephrine in the CR clinic. Defibrillation with 200 J was delivered. After the successful defibrillation, the VF was terminated and the patient recovered his consciousness.He was admitted to the intensive care unit (ICU). The blood test showed that the levels of potassium and calcium (3.8 mmol/L and 8.7 mg/dL, respectively) were in the normal range. However, the magnesium level was 1.6 mg/dL,which was the lowest value measured in this patient. Magnesium supplementation was promptly initiated. After 9 days, the patient underwent successful insertion of an implantable cardioverter defibrillator (ICD). Thereafter, he was discharged with independent gait.
When performing CR, it is important to ensure the safety of patients with heart disease. There are three major safety gears to prevent cardiovascular events during CR. The first is risk stratification for exercise-related cardiovascular events through a medical record review and cardiopulmonary exercise test (CPET). The second is individualized exercise prescription. The third is monitoring of the ECG, blood pressure, heart rate, and symptoms during exercise, conducted by a CR specialist. The patient in this case report was classified as a high-risk patient because of the history of a previous cardiac arrest, VF, and left ventricular ejection fraction (LVEF) < 40%. In addition, he had three-vessel coronary artery disease (Figure 2) but did not undergo percutaneous coronary intervention (PCI) and ICD insertion at the hospital where he was treated for the first cardiac arrest.We presumed that the cardiologist might have determined that conservative treatment with medicine was more appropriate than PCI, because the main causative lesion of myocardial ischemia was chronic total occlusion of the obtuse marginal branch. Further, according to the medical records from the other hospital, ICD insertion was postponed because the patient’s ECG no longer showed sustained ventricular tachycardia and the treatment outcome was expected to be poor during the ICU admission period. These characteristics are not risk stratification criteria for CR participation. This case shows that more careful exercise prescription and exercise monitoring are needed if CR was not sufficiently performed or if an ICD was not inserted in a patient who needed an ICD device. When the current patient had the first cardiac arrest with VF, ICD insertion was considered but postponed at the other hospital because of recurrent pneumonia. When he was transferred to our hospital, he not only had carbapenem-resistant Enterobacteriaceae colonization but was also in a bedridden state. After two months of CR, he could walk independently. He underwent a CPET,which showed a VO2maxof 16.2 mL/kg per min and maximal heart rate of 130 beats/min. The ECG during CPET showed frequent premature ventricular contractions without more serious features including wide QRS complex or QT prolongation. His hemodynamic response was acceptable, and he did not complain of chest pain or other symptoms.
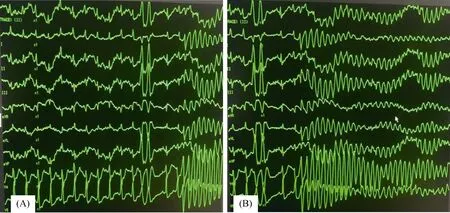
Figure 1. ECG results. (A): A ventricular couplet followed by polymorphic ventricular tachycardia; (B): the QRS complexes was shown a progressive change and twisting pattern.
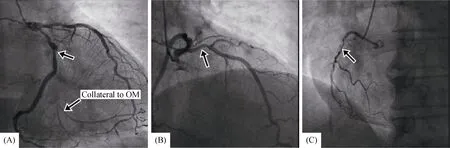
Figure 2. Coronary angiography. (A): Left coronary angiography demonstrating a total occlusion of obtuse marginal branch, arrow indicates occluded marginal branch with collateral artery; (B): left coronary angiography showing a 60% stenosis of left anterior descending artery, arrow indicates stenosed portion of left anterior descending artery; (C) right coronary angiography demonstrating a 80% stenosis of right coronary artery, arrow indicates stenosed portion of right coronary artery.
Studies about the risk of exercise training for patients with cardiovascular disease (CVD) have indicated that about one cardiac arrest in every 115,000 patient-hours of CR and one death in every 750,000 patient-hours of CR participation occur.[1]Since 2000, most of the studies stratified participants according to the risk of exercise-induced cardiac arrest before the initiation of a CR program and conducted ECG monitoring, which resulted in rates of one cardiac arrest in 100,000 patient-hours of CR, one myocardial infarction in 300,000 patient-hours of CR, and 0-1 death in every 300,000-700,000 patient-hours of CR, which are rather low.[2]It is known that the type and intensity of exercise greatly affect exercise-related mortality and ECG monitoring during exercise significantly reduces the incidence of exercise-related myocardial infarction.[3]A study in South Korea reported that no events of acute myocardial infarction, cardiac arrest, and death were found in a total of 13,934 patient-hours of CR.[4]Moreover, cardiovascular events during supervised exercise training are rare, and there are no established predictors of which patients with CVD are likely to experience exercise-related cardiac events.[5]When cardiac resuscitation is immediately performed by a cardiac specialist, the mortality rate can be decreased by six times.[6]In the present case, the patient underwent supervised exercise training conducted by a CR specialist, with ECG monitoring. As soon as cardiac arrest occurred, CPR and defibrillation could be promptly performed. Therefore, the patient was resuscitated without other serious complications.
In conclusion, patients with LVEF < 40%, exercise-induced ischemia, complex ventricular arrhythmias, hemodynamically significant residual coronary stenosis, or cardiac device implants are likely to be at an increased risk and should be considered for careful exercise prescription and supervised exercise training with ECG monitoring.
 Journal of Geriatric Cardiology2020年1期
Journal of Geriatric Cardiology2020年1期
- Journal of Geriatric Cardiology的其它文章
- “One-man” bailout technique for high-speed rotational atherectomy—assisted percutaneous coronary intervention in an octogenarian
- Aspergillus infection of pacemaker in an immunocompetent host: a case report
- Is dual therapy the correct strategy in frail elderly patients with atrial fibrillation and acute coronary syndrome?
- A meta-analysis of 1-year outcomes of transcatheter versus surgical aortic valve replacement in low-risk patients with severe aortic stenosis
- Anemia in patients with high-risk acute coronary syndromes admitted to Intensive Cardiac Care Units
- Prognostic factors in heart failure patients with cardiac cachexia