
“One-man” bailout technique for high-speed rotational atherectomy—assisted percutaneous coronary intervention in an octogenarian
2020-02-11 14:48:20GeorgeKassimisDimitriosPapakonstantinouIoannisTsounosIoannisKanonidis
Journal of Geriatric Cardiology 2020年1期
George Kassimis, Dimitrios Papakonstantinou, Ioannis Tsounos, Ioannis Kanonidis
1Second Department of Cardiology, Hippokration Hospital, Medical School, Aristotle University of Thessaloniki, Thessaloniki, Greece
2St Paul General Hospital, Thessaloniki, Greece
Keywords: Bailout procedure; Calcified coronary lesion; Rotational atherectomy; Single operator technique
Heavily calcified coronary lesions continue to represent a challenge for percutaneous coronary intervention (PCI), as they are difficult to dilate, and it is difficult to deliver and implant drug-eluting stents (DES) properly. Poor stent deployment is associated with high rates of periprocedural complications and suboptimal long-term clinical outcomes.[1]Thanks to the introduction of several adjunctive PCI tools,like cutting and scoring balloons, and to the novel intravascular lithotripsy technology, the treatment of such lesions has become increasingly feasible, predictable and safe.[2]However, 360° concentric superficial calcification with inability to cross the calcified lesion with a balloon mandates the use of rotational or orbital atherectomy,[2]which can be safely performed via the transfemoral or transradial approach.[3,4]In this technical note, we report our initial experience of the “one-man” bailout high-speed rotational atherectomy (HSRA) technique, whereby the operator both advances the HSRA device and keeps the distal wire in place.
An 82-year-old male with an anterior non-ST segment elevation myocardial infarction was admitted in our centre.Past medical history included established ischemic heart disease with previous PCI of a mid-right coronary artery(RCA) stenosis, an abdominal aortic aneurysm repair, hypertension and chronic kidney disease. He was on maximal tolerated optimal medical therapy and coronary angiography(CA) demonstrated a patent RCA stent in a right dominant system, left circumflex artery unobstructed and a critical severely calcified mid left anterior descending (LAD) lesion(Figure 1A and B, white asterisk).
Anad hocangioplasty of mid LAD lesion via the transfemoral approach was offered. Due to an aneurysm of the thoracic aorta, guide catheter (GC) manipulation proved very difficult. Finally, a 6F GC JL5 (Cordis VISTA BRITE TIP?) gave acceptable support. Given the extensive LAD calcific burden on CA, a decision was made to perform plaque modification with non-compliant (NC) or scoring balloons and using the Rotablator?HSRA system (Boston Scientific, Natick, MA, USA) as a bailout technique if needed.
Patient was treated with aspirin and ticagrelor prior to PCI. Intravenous 100 U/kg bolus heparin was administered to maintain the activated clotting time > 250 s. A Fielder XT(ASAHI) crossed the lesion with difficulty. A small 1.2 mm over-the-wire semi-compliant balloon could not pass;therefore, bailout HSRA was performed. The initial wire was exchanged with the Rota-floppy wire (Boston Scientific)using a Quickcross support microcatheter (Spectranetics)(Figure 1C and D). A 1.5 mm burr was selected to reach a burr/vessel ratio approaching 0.6 with an intention to use only a single burr to ablate LAD plaque and facilitate the passage of further devices (Figure 1E). HSRA speed was set at 160,000 r/min. In our center, HSRA is usually performed in conjunction with an intracoronary infusion of a “cocktail”containing verapamil, heparin and nitroglycerine with burr runs < 20 s in duration to avoid burr deceleration. In most of the cases, an assistant is needed to fix and stabilize the Rota-wire in position at the end of the catheterization lab table while the primary operator advances the burr and drive shaft. This part is challenging and the technique requires an operator and assistant who work carefully in sync. However,a qualified and experienced assistant is not always available as in our case, and the primary operator may not want to risk the loss of wire position by accidental movements of an inexperienced assistant. While in theory procedures like ours could be rescheduled to ensure adequate assistance for the primary operator, this can be challenging as in our case and is usually not encouraged. Therefore, we proceeded with the “one-man” technique that allows both delivery and retrieval of an HSRA device with only one skilled primary operator.
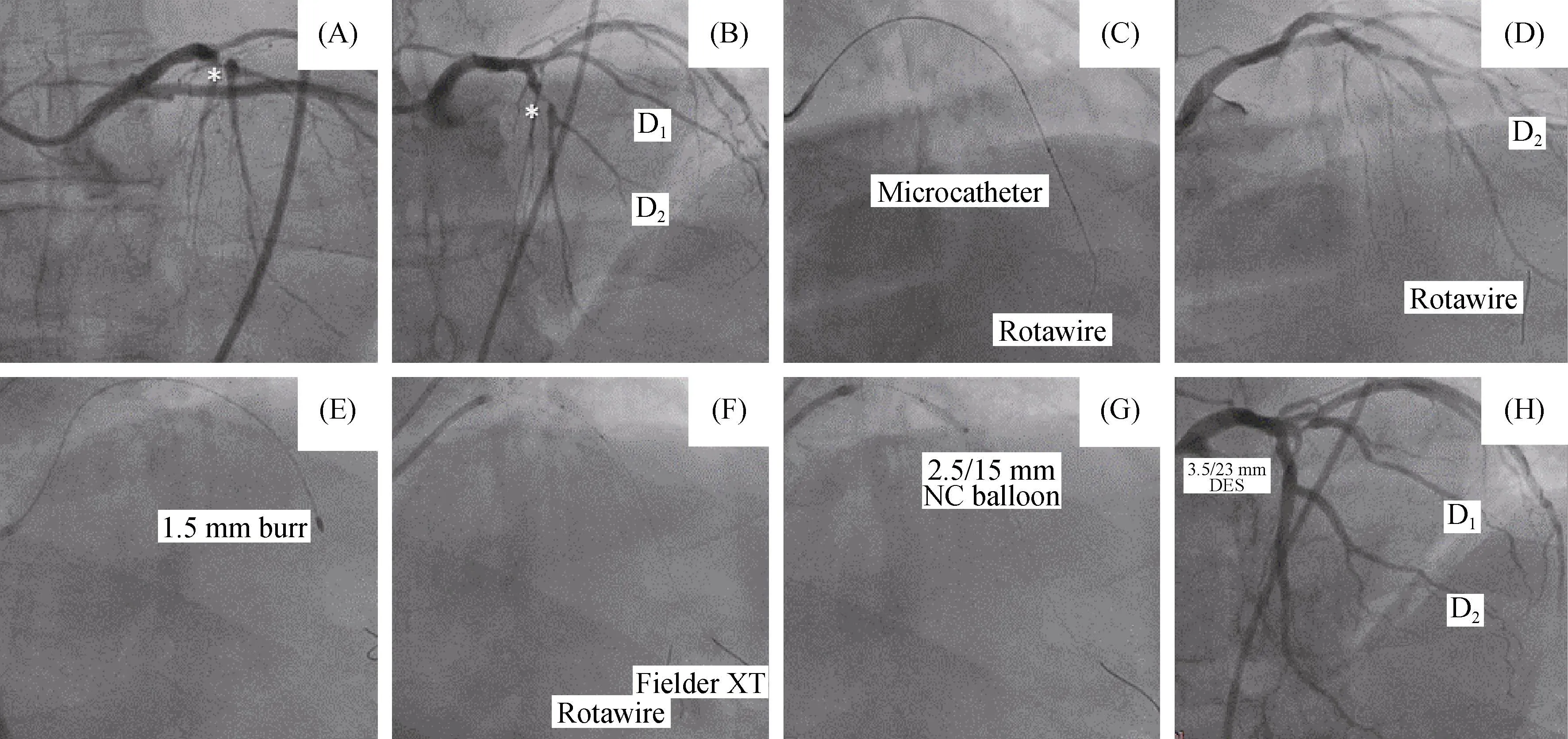
Figure 1. Coronary angiography of left coronary system. (A&B): Left circumflex artery unobstructed with a critical severely calcified mid left anterior descending (LAD) lesion (white asterisk); (C & D): the initial wire was exchanged with the Rota-floppy wire (Boston Scientific) using a Quickcross support microcatheter (Spectranetics); (E): a 1.5 mm burr was selected to reach a burr/vessel ratio approaching 0.6 with an intention to use only a single burr to ablate LAD plaque and facilitate the passage of further devices; (F, G): the LAD lesion was re-crossed with the conventional wire and the rotawire left in place to confirm successful balloon expansion with a 2.5 × 15 mm NC Quantum Apex (Boston Scientific) and then act as a “buddy wire” to facilitate stent placement with 1 DES Eucatech 3.5/23 mm eucaLimus Sirolimus Eluting Coronary Stent System which was finally post-dilated with a 3.5/12 mm NC Quantum Apex at high atm; (H): an excellent angiographical result was achieved.
The burr was tested and primed prior to insertion into the GC while mounted on the wire. After the burr is advanced through the Tuohy Borst valve, the shaft was looped in an“S” configuration and the advancer placed next to the Tuohy Borst as previously suggested.[5]The burr was advanced over the wire with the left hand while the right hand simultaneously pulled the Rota-wire back, while monitoring the wire position under fluoroscopy. Two passes of rotablation were performed into the LAD (Figure 1E). After plaque modification was completed, the burr was removed by the“single-operator” technique by opening the Tuohy Borst valve and just pushing the RA wire at low-speed rotation in Dynaglide mode. The LAD lesion was re-crossed with the conventional wire and the rotawire left in place to confirm successful balloon expansion with a 2.5 × 15 mm NC Quantum Apex (Boston Scientific) and then act as a “buddy wire” (Figure 1F & G) to facilitate initial stent placement with 1 DES Eucatech 3.5/23 mm eucaLimus Sirolimus Eluting Coronary Stent System (Figure 1H) which was finally post-dilated with a 3.5/12 mm NC Quantum Apex at high atm. An excellent angiographical result was achieved.Dual-antiplatelet therapy was scheduled for 1-year post- PCI.
Despite the presence of coronary artery calcification in approximately 38% of people during angiography and 73%with IVUS, coronary atherectomy is used in 3% to 5% in select high-volume centers and < 1% in others.[6,7]
Reasons for underutilization of coronary atherectomy include operator inexperience, the lack of robust long-term clinical data, increased cost and time of the procedure, and unavailability of a reliable assistant to maintain wire position during advancement.[1,8]The “one-man” technique,whereby a single operator advances the HSRA system while simultaneously maintaining wire position, is safe and effective and obviates the need for an assistant who is skilled with this technology.
Learning this technique can be accomplished by initially performing it in uncomplicated cases with focal lesions in straight segments of the vessel in which loss of wire position can be easily corrected by re-advancing the wire. Mastery of this technique can be achieved within the first cases in already sufficiently experienced physicians.
Bailout “one-man” HSRA technique is a feasible, safe,and an effective treatment option for severely calcified lesions when a skilled assistant is not available and removes a barrier to its use.
 Journal of Geriatric Cardiology2020年1期
Journal of Geriatric Cardiology2020年1期
- Journal of Geriatric Cardiology的其它文章
- Polymorphic ventricular tachycardia during phase II cardiac rehabilitation in a patient with heart failure: a case report
- Aspergillus infection of pacemaker in an immunocompetent host: a case report
- Is dual therapy the correct strategy in frail elderly patients with atrial fibrillation and acute coronary syndrome?
- A meta-analysis of 1-year outcomes of transcatheter versus surgical aortic valve replacement in low-risk patients with severe aortic stenosis
- Anemia in patients with high-risk acute coronary syndromes admitted to Intensive Cardiac Care Units
- Prognostic factors in heart failure patients with cardiac cachexia