
Combined hepatic segment color rendering technique improves the outcome of anatomical hepatectomy in patients with hepatocellular carcinoma
2023-10-30 10:36:20JiYeChenJunHnZhiWeiLiuXinLeiXinPengFeiWngShouWngCi
Ji-Ye Chen ,Jun Hn ,Zhi-Wei Liu ,Xin-Lei Xin ,Peng-Fei Wng ,Shou-Wng Ci ,b,c,?
a Faculty of Hepato-Pancreato-Biliary Surgery, The First Medical Center, Chinese PLA General Hospital, Beijing 100853, China
b Institute of Hepatobiliary Surgery of Chinese PLA, Beijing 100853, China
c Key Laboratory of Digital Hepatobiliary Surgery of Chinese PLA, Beijing 100853, China
Hepatocellular carcinoma (HCC) is the third most common cause for cancer-related death worldwide,especially in China [1] .Hepatectomy is considered one of the most potentially curative therapies for HCC [2] . As HCC is capable of vascular invasion and metastasis via the portal venous system,anatomical resection is often performed to reduce tumor recurrence. This process involves resecting the tumor-bearing portal branches and the corresponding hepatic parenchyma [3] . Certain comparative studies have demonstrated better overall survival and disease-free survival with the use of anatomical resection when compared with nonanatomical resection [4–6] .
However,accurate intraoperative demarcation of the hepatic segmental boundary is essential for implementing anatomical resection. To precisely demarcate the boundary of the target hepatic segment on the liver surface and the boundary in the parenchyma,our group modified the technique of sustained methylene blue staining. In this technique,the feeding pedicle of the hepatic segment to be resected using the intrahepatic Glisson’s sheath method is first identified. Subsequently,the corresponding portal vein of the feeding pedicle is punctured,methylene blue is injected,and the vein is ligated to achieve continuous methylene blue staining effect. Although this procedure may improve the accuracy of selecting the operative boundary during hepatic parenchymal transection,it has some limitations. In some cases,there may be multiple main trunks feeding the relevant segments or the feeding pedicles may be located far from the hilum. In such instances,it is quite difficult to locate the feeding pedicles one by one via the intrahepatic Glissonean approach. In our experience,complete staining of the target hepatic segment was achieved only in 98 of 106(92.5%) cases [7] .
To improve the success rate of complete staining of the target hepatic segment and simplify the operation,we used sustained methylene blue staining technique combined with ultrasoundguided portal vein puncture staining and Glisson’s pedicle transection technique to perform anatomical hepatectomy. This study aimed to summarize our preliminary experience and evaluate the clinical feasibility and safety of this technique for the resection of hepatic segments or subsegments,i.e.,segments 2-8.
From April 2016 to March 2019,anatomic hepatectomy was performed in 50 HCC patients at the Faculty of Hepato-Pancreato-Biliary Surgery,Chinese PLA General Hospital. Our study was approved by the Medical Ethics Committee of the Chinese PLA General Hospital (S2018-111). Written informed consent was provided by all study subjects,and all relevant investigations were performed in strict adherence to the principles of theDeclarationofHelsinki.
The preoperative liver function was evaluated by blood test and indocyanine green (ICG,Yichuang Pharmaceutical,Dandong,China)retention at 15 min. All patients underwent three-phase enhanced computed tomography (CT,General Electric Company,Boston,MA,USA) and magnetic resonance imaging (MRI,General Electric Company). The 3D reconstruction (IQQA-liver System,EDDA Technology Incorporation,Princeton,NJ,USA) was performed to evaluate the anatomical relationship between the tumor and the related adjacent hepatic vessels to ensure that the entire range of the portal venous territory,including the tumor,was covered.
A J-shaped incision was created on the upper-right abdominal quadrant as per the routine procedure. The abdominal cavity was thoroughly examined to ensure absence of any extrahepatic lesions. Intraoperative ultrasound (Noblus,Hitachi,Tokyo,Japan)was performed to confirm the absence of intrahepatic metastasis that had not been preoperatively detected. The hepatoduodenal ligament was preseted with a blocking band. The corresponding left and/or right hepatic pedicle of the segment to be resected was obtained by opening the hepatic hilum and dissecting outside the Glisson’s sheath. As per the preoperative images,the branches of the next hepatic pedicle were continued to be separated. If the portal drainage area to be resected was supplied by multiple hepatic pedicles or if the location of the hepatic pedicles was detected to be deep inside the hepatic parenchyma,it was deemed difficult to determine all the hepatic pedicles to be resected using a simple method through the intrahepatic Glisson’s sheath along the hepatic hilum. We accordingly combined the technique of ultrasoundguided portal vein puncture staining of methylene blue (Jichuan Pharmaceutical,Jiangsu,China) and Glisson’s pedicle transection to demarcate the boundary of the target hepatic segment. Subsequently,the perihepatic ligament was divided,and the blood flow into the liver was blocked. Hepatic parenchyma was resected along the dying boundary. The anatomical resections of S8 segment and S6 + S5d segments were illustrated in Figs. 1 and 2,respectively.

Fig. 2. The tumor located in S6 + S5d segments of liver. A: Preoperative imaging confirmed that the tumor was located in S6 + S5d segments. There were multiple hepatic pedicles supplying S6,which were closely related to tumor. B: During the operation,the right posterior hepatic pedicle was dissected out of the Glisson’s sheath,and the artery clamp was tried to block to mark the ischemic boundary of the right posterior lobe of the liver. C: The dorsal hepatic pedicle of S5 was dissociated by the technique through the intrahepatic Glisson’s sheath. The portal vein of the hepatic pedicle was punctured with indwelling needle under direct vision. After the blood flow out,5 mL methylene blue was injected,and the dorsal branch of S5 was ligated immediately. D: Intraoperative ultrasound was performed to find the portal vein branches of S7.Under the guidance of ultrasound,the portal vein of S7 was punctured with 20G needle,and 5 mL methylene blue was injected into the portal vein. E: The S6 boundary was demarcated by the staining method. F: The target hepatic segment was completely removed along the blue staining boundary (including the inner boundary of hepatic parenchyma). G: Tumor specimens after surgery.
A total of 50 patients with Child-Pugh grade A were treated using anatomical hepatectomy. The mean largest tumor diameter was 4.9 ± 2.9 cm. The clinical data of all patients are listed in Table 1 .
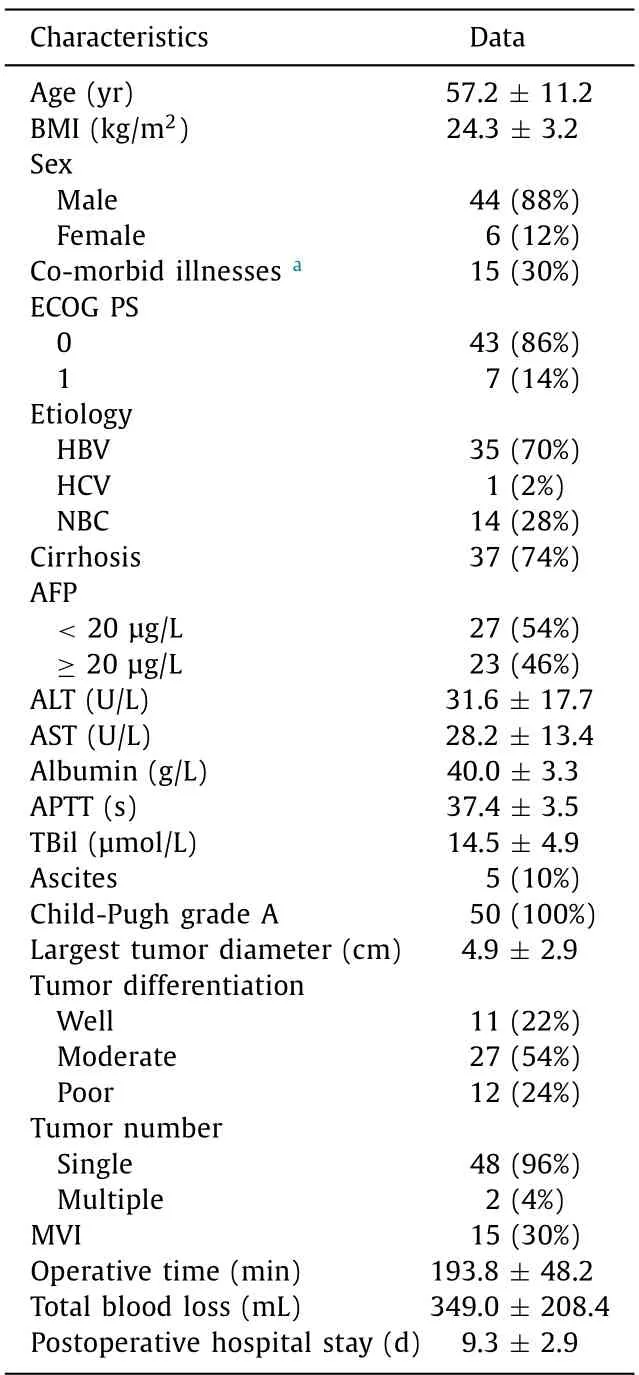
Table 1Baseline data and characteristics of patients( n = 50).
The success rate of staining was 100%. The surgical off-section was accurately selected because of the lasting staining effect.Among the treated cases,27 underwent segmental hepatectomy (2 of S4,9 of S5,4 of S6,5 of S7,and 7 of S8),3 underwent subsegmental resection (1 of S4b and 2 of S8d),and 20 underwent combined hepatic (sub) resection (2 of S5 + S8,4 of S5 + S6,7 of S6 + S7,1 of S6 + S7 + S8,2 of S5 + S8d,1 of S6 + S5d,1 of S6 + S5v,1 of S8 + S5d,and 1 of S6 + S7 + S8d). The mean operative time was 193.8 ± 48.2 min,and the average intraoperative blood loss was 349.0 ± 208.4 mL. No complications beyond Clavien-Dindo grade III were noted,and there was no postoperative mortality. The mean hospital stay was 9.3 ± 2.9 days.
HCC tends to invade the portal vein and form tumor thrombus and satellite. HCC has the biological characteristics of spreading along the portal vein branches of the tumor-bearing hepatic segment [3] . Segmental hepatectomy can completely remove the lesions and preserve the remaining liver function to the maximum extent. Hence,this procedure is considered the best surgical treatment for HCC [ 5,6 ]. It has been reported that anatomical segmental hepatectomy significantly improves the prognosis of patients withHCC,and the 5-year survival rate can reach 60%-65% [4–6] . Our previous study confirmed the superiority of anatomical segmental hepatectomy over other methods in the treatment of HCC [7] .
However,accurate demarcation of the hepatic segment boundary,which is important for performing anatomical segmental hepatectomy,is a major challenge for hepatobiliary surgeons. At present,there are some commonly used clinical techniques. Makuuchi [8] injected methylene blue into the portal vein branch of the target hepatic segment under the guidance of intraoperative ultrasound,and the corresponding hepatic segments were stained. Glisson’s pedicle transection hepatectomy has been well implemented in clinical practice [9] . However,the boundary of the hepatic segments demarcated by these methods can only be displayed on the surface of the liver,and the boundary of the hepatic parenchyma cannot be accurately judged. Owing to this limitation,we modified the technique of methylene blue staining [7] . However,this technique is relatively difficult and complex,especially for patients with multiple hepatic pedicle blood supply or deep positioning of hepatic pedicle. Therefore,it is difficult to be universally applied in clinical practice.
In view of the these limitations,we combined the existing techniques using sustained methylene blue staining with ultrasoundguided hepatic portal vein puncture staining and Glisson’s pedicle transection technique to perform anatomical hepatic segment resection. This method has several advantages. First,compared with the single sustained methylene blue staining,the combined application of hepatic segment color rendering technique improves the success rate of hepatic segment staining. Most of the cases were complicated combined hepatic segmental (subsegment) resection and/or central regional hepatic segment resection (such as S5 and S8). In such instances,it is difficult to achieve satisfactory results of hepatic segment staining with single routine technique.The staining rate with our method was 100%. Second,the combined application of hepatic segment color rendering technique can reduce the surgical difficulties and improve the safety. Third,after locating the target hepatic pedicle,either via the extrahepatic dissection or the technique of Glisson’s pedicle transection,the method of ligating the hepatic pedicles after injecting methylene blue was used to reveal the boundary of the hepatic segment in the parenchyma and enhance the surgical precision. Moreover,microvascular invasion,which is well-acknowledged as a predictor of HCC recurrence,accounted for 30% in this cohort [10] . Anatomical resection is known for complete removal of the tumor-bearing portal territory. Patients with unfavorable tumor characteristics,such as microvascular invasion,are likely to be benefitted from our novel hepatic segment color rendering technique for anatomical resection [11] .
Accurate preoperative image evaluation,especially 3D reconstruction technique,is of immense importance in clinical practice.It is imperative to preoperatively define the supply hepatic pedicle and the portal vein drainage area of the hepatic segment to be resected. Furthermore,based on the location of the tumor and the anatomical characteristics of the corresponding hepatic segment,the individualized application of hepatic segment color rendering technical scheme was selected. For resection of hepatic segments located in the central region,the extrahepatic anatomy technique along the Glisson’s sheath combined with Glisson’s pedicle transection technique is routinely used to locate the corresponding hepatic pedicle. If the blood supply of the hepatic segment to be resected comes from multiple branches of the portal vein or if the tumor is located between two hepatic segments,it is diffi-cult to identify all the hepatic pedicles. The extrahepatic anatomy technique along the Glisson’s sheath combined with intraoperative ultrasound-guided portal vein puncture and staining technique is usually applied to define the boundary of the hepatic segment to be resected.
The staining of the hepatic parenchyma was sustained because the Glisson’s pedicle was ligated after the methylene blue injection [7] . Staining the boundary on the liver surface combined with the hepatic parenchyma on the inside helped in navigating the anatomical resection. However,methylene blue staining in some hepatic parenchyma diminished toward the end of the operation. In recent years,some researchers have introduced fluorescent ICG to stain the target hepatic segment for intraoperative navigation. Owing to dye diffusion,low depth of tissue penetration,and fluorescence contamination from the hilar ductal arterial communication,the application of fluorescent ICG needs to be improved [ 12,13 ]. In the above situation,intrasegmental hepatic veins are located using intraoperative ultrasound to establish the resection boundaries,which requires the surgeons to possess excellent ultrasound skills and familiarity with intrahepatic anatomy.At present,real-time virtual sonography can display real-time intraoperative ultrasound images and the corresponding multiplanar reconstruction images of preoperative CT and/or MRI side-by-side on a television monitor synchronously [ 14,15 ]. Such a display aids the surgeon in locating the intrahepatic vessels and bile ducts and is of great help in performing accurate anatomical hepatectomy.Augmented reality is another rapidly evolving 3D technology based on the combination of high-quality preoperative imaging data and serves as a digital surgical platform that integrates 3D image reconstruction and geometric analysis [16] . The real-time technologies mentioned above have the potential to improve hepatobiliary surgical procedures. However,the liver can move freely and change its shape during the surgery,which makes the precise identification of the internal anatomy of the tumor sites or vessels difficult based on static images. Adapting the real-time navigation system to our combined hepatic segment demarcation technique is being investigated in detail by our group.
Over the past two decades,the laparoscopic approach to the surgical management of HCC has received widespread attention [ 17,18 ]. Laparoscopic anatomical hepatectomy comprises a small but growing percentage of total laparoscopic hepatectomies [19] . Ultrasound provides good guidance for identifying the portal veins and hepatic veins,but laparoscopic vision hinders real-time utilization under two dimensions [20] . Therefore,defining the intrahepatic duct in the laparoscopic view is a challenging issue while performing anatomical hepatectomy.Our group has been trying to apply the hepatic segment color rendering technique reported herein under laparoscopic conditions and shares our clinical experience here.
In summary,the currently available hepatic segment boundary demarcation techniques have their own limitations. In the field of anatomical hepatectomy,these techniques do not complement each other. We should combine these techniques in our clinical practice. The present study shows that the combined hepatic segment color rendering technique mode is safe and reliable in anatomical hepatic segment resection. This technique warrants further investigation to improve the long-term survival of patients with HCC.
Acknowledgments
None.
CRediT authorship contribution statement
Ji-YeChen:Conceptualization,Methodology,Writing – original draft.JunHan:Data curation,Formal analysis,Funding acquisition,Methodology,Writing – original draft.Zhi-WeiLiu:Data curation,Methodology.Xian-LeiXin:Data curation.Peng-FeiWang:Data curation.Shou-WangCai:Conceptualization,Methodology,Supervision,Writing – review & editing.
Funding
This study was supported by a grant from the National Natural Science Foundation of China (82102861).
Ethical approval
This study was approved by the Medical Ethics Committee of the Chinese PLA General Hospital (S2018-111). Written informed consent was obtained from all enrolled patients,and all relevant investigations were performed according to the principles of theDeclarationofHelsinki.
Competing interest
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
 Hepatobiliary & Pancreatic Diseases International2023年5期
Hepatobiliary & Pancreatic Diseases International2023年5期
- Hepatobiliary & Pancreatic Diseases International的其它文章
- Right hepatectomy with a cholangiojejunostomy and hepaticojejunostomy for unilobar Caroli’s syndrome
- Total three-dimensional laparoscopic radical resection for Bismuth type IV hilar cholangiocarcinoma
- A surgical technique using the gastroepiploic vein for portal inflow restoration in living donor liver transplantation in a patient with diffuse portomesenteric thrombosis
- Full laparoscopic anatomical liver segment VII resection with preferred Glissonean pedicle and dorsal hepatic approach
- Targeting mitochondrial transcription factor A sensitizes pancreatic cancer cell to gemcitabine
- Pathogen detection in patients with perihilar cholangiocarcinoma:Implications for targeted perioperative antibiotic therapy