
Colorectal cancer burden,trends and risk factors in China:A review and comparison with the United States
2022-11-15 03:12:54QianruLiHongliangWuMaomaoCaoHeLiSiyiHeFanYangXinxinYanShaoliZhangYiTengChangfaXiaJiPengWanqingChen
Qianru Li ,Hongliang Wu ,Maomao Cao ,He Li ,Siyi He ,Fan Yang ,Xinxin Yan,Shaoli Zhang,Yi Teng,Changfa Xia,Ji Peng,Wanqing Chen
1Office of Cancer Screening,National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital,Chinese Academy of Medical Sciences and Peking Union Medical College/Chinese Academy of Medical Sciences Key Laboratory for National Cancer Big Data Analysis and Implement,Beijing 100021,China;2Department of Anesthesiology,National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital,Chinese Academy of Medical Sciences and Peking Union Medical College,Beijing 100021,China;3Department of Cancer Prevention and Control,Shenzhen Center for Chronic Disease Control,Shenzhen 518020,China
Abstract Objective:China and the United States (the U.S.) have the heaviest colorectal cancer (CRC) burden with considerable variations in temporal trends.This study aims to analyze the temporal patterns of CRC burden and its risk factors in China and the U.S.across the past three decades.Methods:Data were extracted from the Global Burden of Disease (GBD) Study in 2019,including cases,deaths,disability-adjusted life-years (DALYs),age-standardized rate (ASR),and summary exposure value (SEV) of CRC in China and the U.S.between 1990 and 2019.Annual average percentage changes (AAPCs) of CRC burden were calculated using the Joinpoint regression model.The mortality in CRC attributable to potential risk factors was characterized by countries,gender,and age groups.Results:In 2019,there were 607,900 and 227,241 CRC cases,and 261,777 and 84,026 CRC deaths in China and the U.S.,respectively.The age-standardized incidence rate (ASIR) was 30.55 per 100,000 in China and 41.86 per 100,000 in the U.S.,and the age-standardized mortality rate (ASMR) was 13.86 per 100,000 in China and 14.77 per 100,000 in the U.S.CRC incidence,mortality,and DALY rate in the U.S.showed downward trends in the past three decades (AAPC=-0.47,-1.06,and -0.88,respectively),while upward trends were observed in China(AAPC=3.11,1.05,and 0.91,respectively).Among the cause of CRC,the leading risk factor contributing to CRC death was low milk in China and smoking in the U.S.,respectively.Conclusions:From 1990 to 2019,the burden of CRC in China increased dramatically,particularly for males and middle-aged and elderly people.The management of the major risk factors associated with the high burden of CRC should be enhanced.
Keywords: Colorectal cancer;burden;trends;China;the U.S.
Introduction
Colorectal cancer (CRC) is the third most common cause of cancer-related death worldwide (1). Data from GLOBOCAN 2020 showed that there were more than 1,900,000 new cases and 935,000 deaths,accounting for one-tenth of the cancer cases and deaths (2).The distribution of CRC burden varies considerably among human development index (HDI) regions,with more than two-thirds of all new cases and about 60% of all deaths occurring in countries with a high or very high HDI (3).Moreover,large disparities in temporal trends in CRC burden have also been observed in recent years.Countries in middle-to-high HDI have experienced a rapid increase in incidence and mortality,while some countries with the highest HDI,such as the United States (the U.S.) and Europe,display stable or decreasing trends (4).The driving forces underlying this pattern are ill-defined but may partly reflect geographical variation in the prevalence of modifiable CRC risk factors and CRC screening uptake (5).Sufficient evidence has verified smoking,alcohol intake,body fatness,and red and processed meat consumption as the main risk factors for CRC onset.Additionally,some CRC-protective factors,including physical activity,dietary fiber-rich meals,whole grains,and dairy products,have also been found (6).It was reported that 58.2% of CRC death and 57.6% of CRC-related disability-adjusted life years (DALYs) globally were estimated to be attributable to known risk factors (7).
China has an immense CRC burden,accounting for about 30% of all new cases and all CRC-related deaths worldwide (8).The sharp increase in CRC burden was strongly affected by the acquisition of smoking,alcohol abuse,sedentary lifestyles,overnutrition,and metabolic risk factors paralleled by the undergoing rapid socioeconomic transition that developed countries like the U.S.have experienced decades ago.An array of comprehensive CRC prevention strategies must be established and refined to deal with the rising CRC burden in China.The successful cancer control interventions implemented in the U.S.are valuable references for China and the comparison of cancer incidence,mortality,and DALYs between China and the U.S.can provide useful information for cancer prevention and control.Therefore,this study employed the latest data from the Global Burden of Disease (GBD) 2019 database to report CRC burden in CRC incidence,mortality,and DALY,and the contributions of risk factors to CRC deaths in China and the U.S.
Materials and methods
Data collection on disease burden of CRC
Data in this analysis was extracted from the GBD 2019 database using the Global Health Data Exchange (GHDx)query tool (http://ghdx.healthdata.org/) (9).The GBD study provides updated estimates of incidence,mortality,DALYs,and corresponding risk factors by age group and sex annually (10).To assess the temporal trends,we collected overall,age-and gender-specific CRC new cases,deaths,DALYs,and age-standardized rates (ASRs) [with 95% uncertainty intervals (95% UIs)] from 1990 to 2019 in China and the U.S.annually.All the rates were reported per 100,000.
Data collection on risk factor exposure of CRC
The GBD 2019 calculated the attributable disease burden of CRC based on a comparative risk assessment (CRA)framework.GBD organized risk factors into four levels,from the broadest (Level 1) to the most specific (Level 4)(7).In this study,we obtained data on the Level 4 groups of risks for CRC and the corresponding summary exposure values (SEVs),including ten death-related risk factors,which were diet low in milk,diet high in red meat,diet high in processed meat,diet low in fiber,diet low in calcium,low physical activity,smoking,alcohol use,high fasting plasma glucose (FPG),and high body-mass index(BMI),respectively (11).The SEV,with a range of 0-100%,was applied to evaluate the exposure distribution of risk factors.A value 0 of SEV refers to the population at no additional risk and a value 1 of SEV refers to the population at the maximum risk level (12).
Statistical analysis
The number of new cases,deaths,age-standardized incidence rate (ASIR),and age-standardized mortality rate(ASMR) of CRC were summarized and plotted by gender and age group for China and the U.S.,respectively.We calculated the change rates of ASIR and ASMR between 1990 and 2019.The change rates of ASMR and SEV attributable to each risk factor were also calculated.
To analyze the temporal patterns of CRC burden over the past three decades,log-linear regression models were constructed to examine trends over time (13).The number of Joinpoints and the relevant P value were calculated by the permutation test,and the best model was chosen based on the Bayesian information criterion (BIC) (14).To indicate the direction and magnitude of the trends,we calculated the annual percent change (APC),average annual percent change (AAPC),and their corresponding 95% confidence interval (95% CI) of incidence,mortality,and DALY for each segment.The terms “increasing” or“decreasing” were used when the AAPC was statistically significant (P<0.05);otherwise,the term “stable” was used.The Joinpoint regression analyses were conducted using the Joinpoint Regression Program software (Version 4.9.0.1,National Cancer Institute,Bethesda,America).All P<0.05 was considered statistically significant.To assess the effect of demographic factors on the secular trends in incidence,mortality,and DALY from 1990 to 2019,the RiskDiff tool was adopted (http://www.regstattools.org/riskdiff/riskdiff.htm),which was further split into two drivers,changing demographics and cancer risk (15).Further detailed data sources and key parameters used are provided inSupplementary Table S1.
Results
Incidence and mortality of CRC in China and the U.S.
In 2019,it was estimated that there were 607,900 CRC new cases (male: 390,204;female: 217,696) in China with an ASIR of 30.55 per 100,000.Males showed higher ASIR than females (41.43 per 100,000vs.21.10 per 100,000)(Table 1).By age group,people in the age group of 65-69 years accounted for the largest proportion of new cases(15.38%) (Figure 1A).The ASIR was the highest for males in 85-89 age group (463.02 per 100,000) and for females in 95+age group (192.92 per 100,000),respectively(Figure 2A).
There were 261,777 deaths in China in 2019 (males:164,730;females: 97,047).The ASMR in China was 13.86 per 100,000,with 19.32 per 100,000 for males and 9.68 per 100,000 for females (Table 1).For both sexes,the predicted deaths increased with age and peaked in 70-74 age group(Figure 1B).The mortality rate increased with age as well,which was the highest for males in 90-94 age group(484.45 per 100,000) and for females in 95+group (242.57 per 100,000).Both the death cases and the mortality rate were higher in males than in females in each age group(Figure 1B,Figure 2B).
The ASIR in China was comparable to ASIR globally(26.71 per 100,000) but lower than that in the U.S.(41.86 per 100,000).The ASMR did not show significant differences among China,the U.S.(14.77 per 100,000),and the world (13.69 per 100,000) (Table 1).The incidence and mortality rates in both countries increased sharply for people aged over 50 years (Figure 2).Additionally,in both males and females,the risk of incidence and death for CRC increased with age.Lager differences favoring males appear starting at the age of about 30 years,and the gender differential was somewhat smaller in the U.S.than in China(Figure 2C,D).
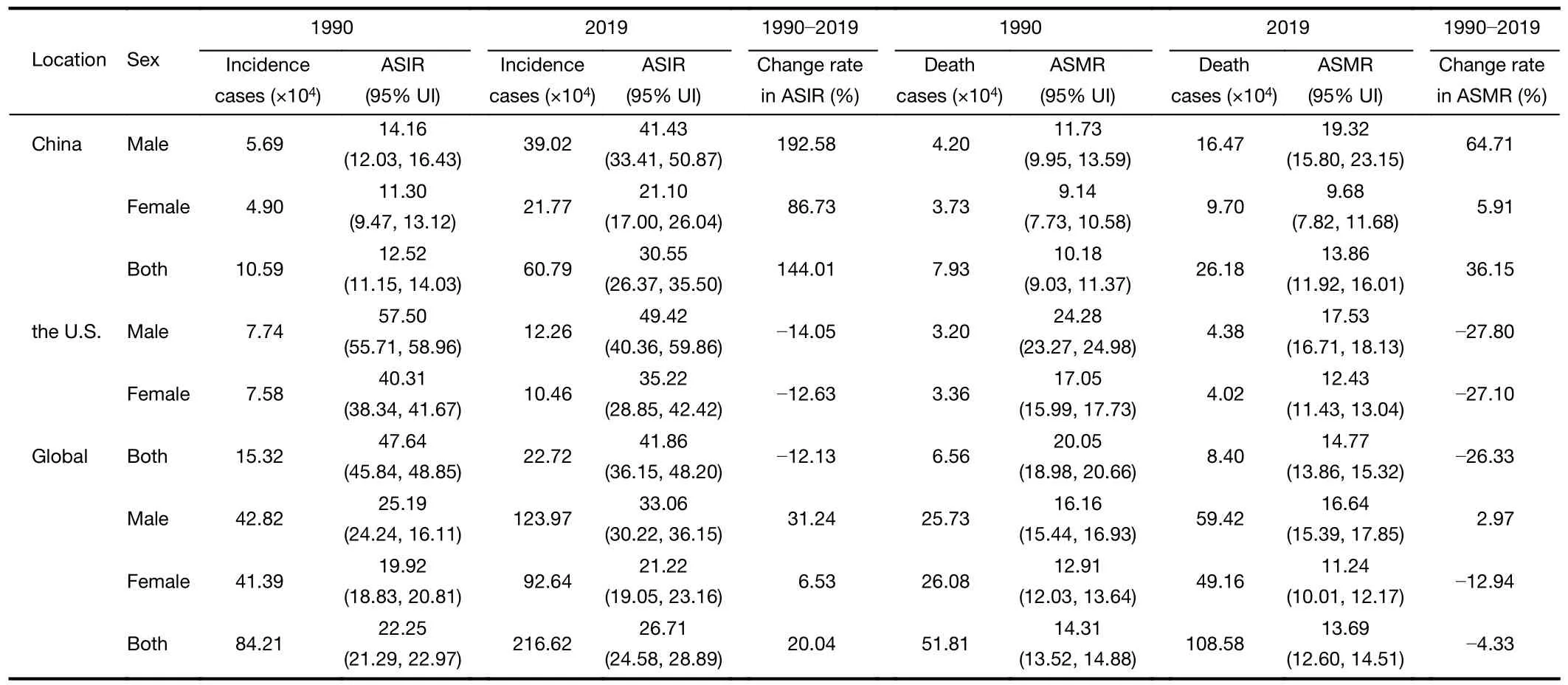
Table 1 Incidence,deaths,corresponding age-standardized rates and change rates of colorectal cancer by sex in China,the U.S.and Global between 1990 and 2019
Trends in CRC incidence,mortality and DALYs in China and the U.S.
For all CRC burden measures included,increasing trends were observed for both sexes in China,while the U.S.exhibited decreasing trends.The incidence and mortality rates of CRC in China presented increased trends with an AAPC of 3.11 (95% CI: 2.89-3.33,P<0.001),and an AAPC of 1.05 (95% CI: 0.83-1.27,P<0.001),respectively.The DALY rate of CRC also showed an upward trend with an AAPC of 0.91 (95% CI: 0.72-1.09,P<0.001) from 1990 to 2019 (Table 2).
In males,the ASIR for CRC in China increased from 14.16 per 100,000 in 1990 to 41.43 per 100,000 in 2019,with an AAPC of 3.75 (95% CI: 3.48-4.03,P<0.001).Whereas ASIR in the U.S.showed a rapidly decreasing trend (AAPC=-0.48,95% CI: -0.76--0.21,P<0.001)(Table 2,Figure 3A).Similar to the ASIR,from 1990 to 2019,the ASMR and the ASR of DALY rate showed increasing trends for China with an AAPC of 1.71 (95%CI: 1.45-1.98,P<0.001) and an AAPC of 1.60 (95% CI:1.36-1.84,P<0.001),respectively (Table 2,Figure 3B),but decreasing trends for the U.S.with AAPCs of -1.10 (95%CI: -1.33--0.87,P<0.001) and -0.90 (95% CI:-1.14--0.66,P<0.001) respectively (Table 2,Figure 3C).
In females,the ASIR for CRC in China increased from 11.30 per 100,000 in 1990 to 21.10 per 100,000 in 2019,with an AAPC of 2.16 (95% CI: 1.94-2.38,P<0.001).Whereas ASIR in the U.S.exhibited a rapidly decreasing trend (AAPC=-0.49,95% CI: -0.71--0.27,P<0.001)(Table 2,Figure 3A).From 1990 to 2019,ASMR showed an increasing trend for China (AAPC=0.16,95% CI:0.03-0.29,P=0.020) and a decreasing trend for the U.S.(AAPC=-1.09,95% CI: -1.24--0.94,P<0.001) (Table 2,Figure 3B).However,the ASR of DALY rate showed decreasing trends for both countries with an AAPC of-0.12 (95% CI: -0.27-0.03,P=0.114) and an AAPC of-0.97 (95% CI: -1.13--0.81,P<0.001),respectively(Table 2,Figure 3C).
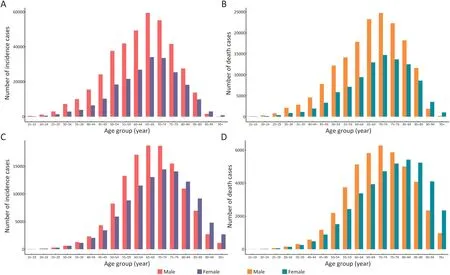
Figure 1 Colorectal cancer incidence,death numbers by gender,age group,and country in 2019.(A) China cases;(B) China deaths;(C) the U.S.cases;(D) the U.S.deaths.
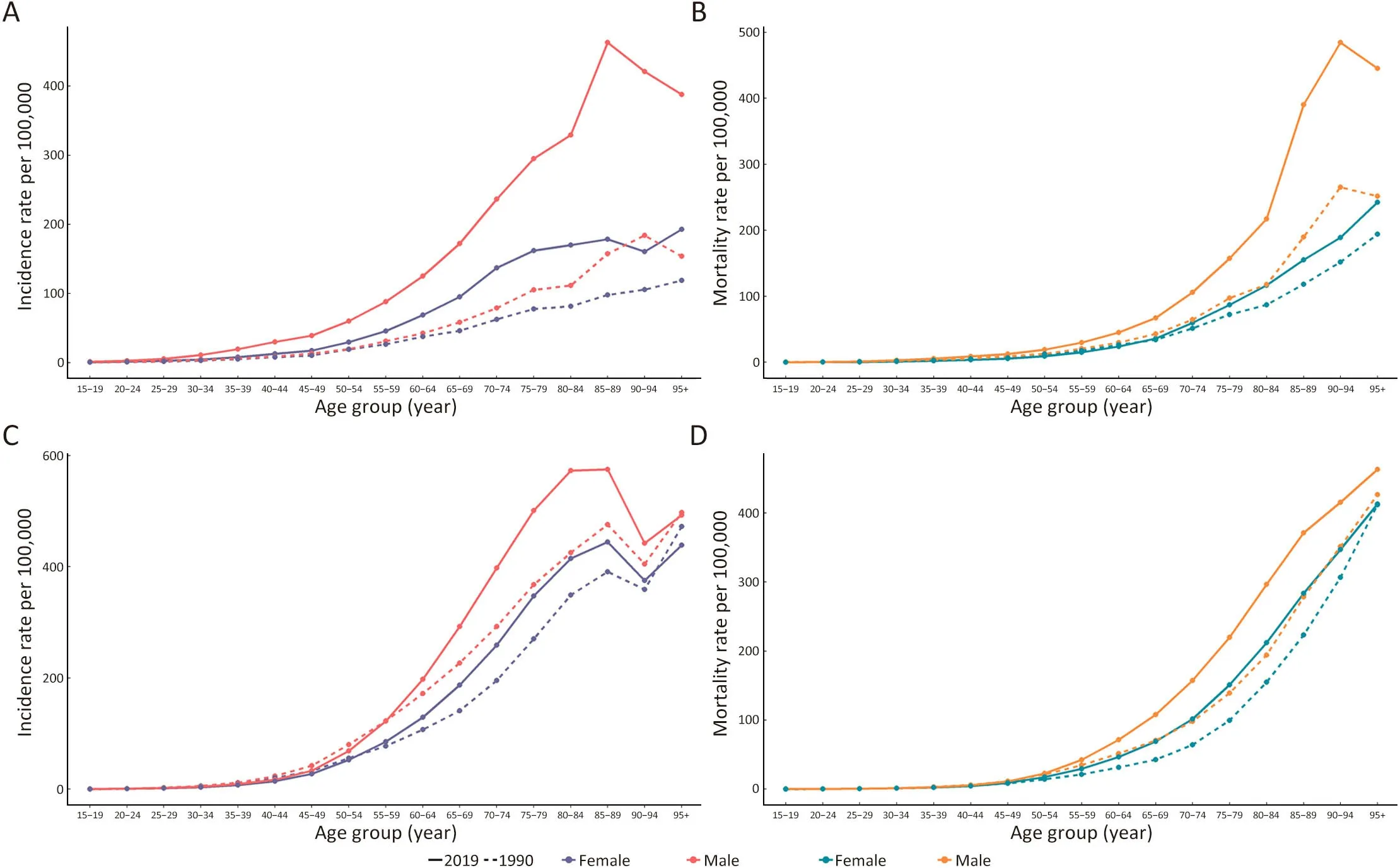
Figure 2 Colorectal cancer incidence,mortality rates (per 100,000) by gender,age group,and country in 1990 and 2019.(A) China incidence rate;(B) China mortality rate;(C) the U.S.incidence rate;(D) the U.S.mortality rate.
Risk factors of CRC deaths
The death to the studied associated risk factors for CRC in 2019 increased gradually with age in both countries between 15 and 89 years old,peaking at 85-89 age group and decreasing at 90 years and older (Figure 4A).Risk factors associated with CRC deaths varied by sex in different age groups.In females,diet low in milk accounted for the largest proportion of CRC ASMR in China,whereas in the U.S.the main risk factor was smoking.In males,smoking contributed the most to ASMR in China,whereas in the U.S.high BMI was the leading deathrelated risk factor (Figure 4B,C).
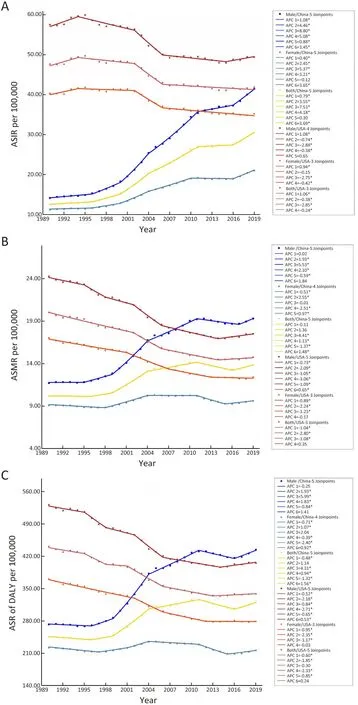
Figure 3 Trend in ASIR (A),ASMR (B) and ASR of DALY rate (C) of colorectal cancer overall and by gender in China and the U.S.ASIR,age-standardized incidence rate;ASMR,age-standardized mortality rate;DALY,disability-adjusted life-year;ASR,age-standardized rate;APC,annual percentage change.
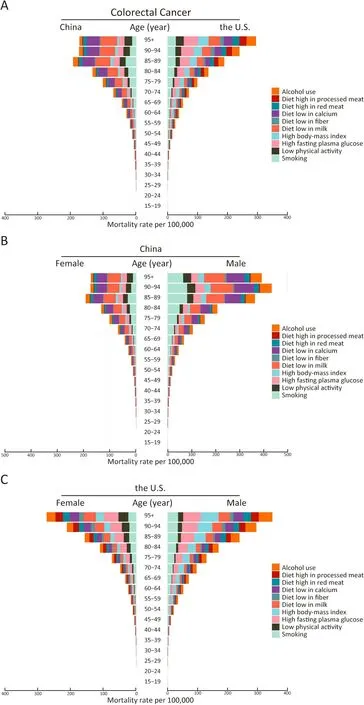
Figure 4 Mortality rate attributed to risk factors for colorectal cancer by age group between China and the U.S.in 2019 (A);by age group and gender in China (B) and by age group and gender in the U.S.(C) in 2019.
In China,the ASMR for CRC due to major potential risk factors increased from 1990 to 2019 (excluding diet low in fiber and calcium).Notably,diet low in milk contributed the most to the CRC death burden,with an ASMR of 2.66(95% UI: 1.75-3.56) per 100,000.Mortality risks increased the fastest in high BMI with an ASIR percentage change of 227.27%.There were also greater increases in high red meat and high processed meat products,with increases of 138.24% and 128.57%,respectively.Besides,the fastest decrease was in low fiber,with a decrease of 44.00%.In the U.S.,the ASMR for CRC due to major risk factors showed a decreasing trend between 1990 and 2019 (excluding high FPG and BMI).Diet low in fiber showed the largest decrease of 50.82% in ASMR.In addition,low physical activity and smoking also had rapid decreases of 46.85%and 40.78%,respectively.And high BMI increased the fastest at 7.82% (Table 3).Diet low in milk,diet low in calcium,and smoking contribute the most part of ASMR for CRC in China in 2019.In the U.S.,smoking,high BMI,and high FPG contribute the most part of ASMR for CRC in 2019.Particularly,smoking played a major role in CRC death,accounting for 2.12 per 100,000 in ASMR for both countries in 2019 (Table 3).
The ASR of SEV in China decreased from 25.60 per 100,000 in 1990 to 21.91 per 100,000 in 2019.Compared to China,the ASR of SEV in the U.S.increased over the past 30 years,from 21.34 per 100,000 in 1990 to 22.51 per 100,000 in 2019.Exposure to high BMI increased the most with the largest change rate of 180.85% in China,and exposure to smoking decreased the most with a change rate of 37.50% in the U.S.(Table 3).
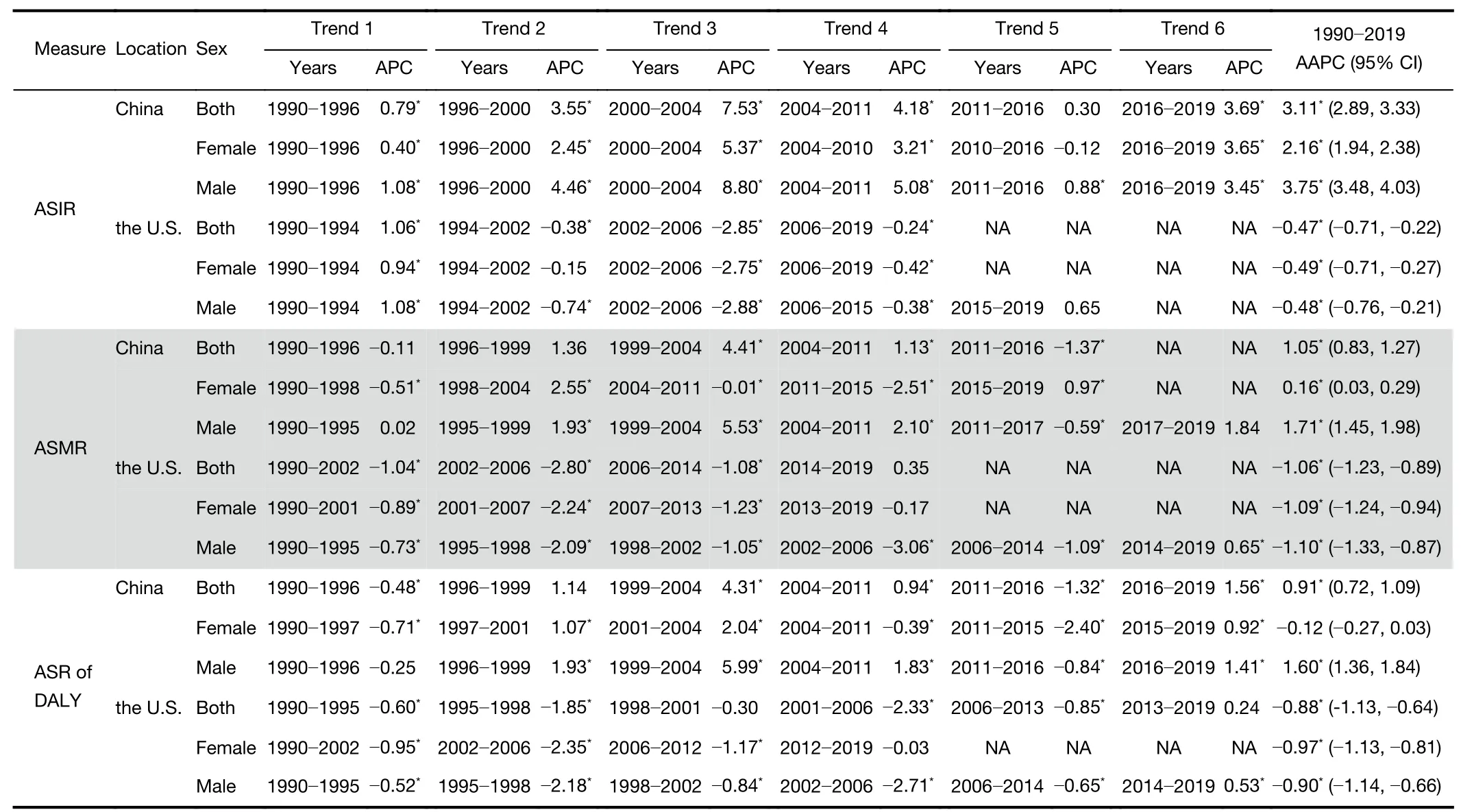
Table 2 Joinpoint analysis for ASIR,ASMR and ASR of DALY rate of colorectal cancer by sex in China and the U.S.between 1990 and 2019
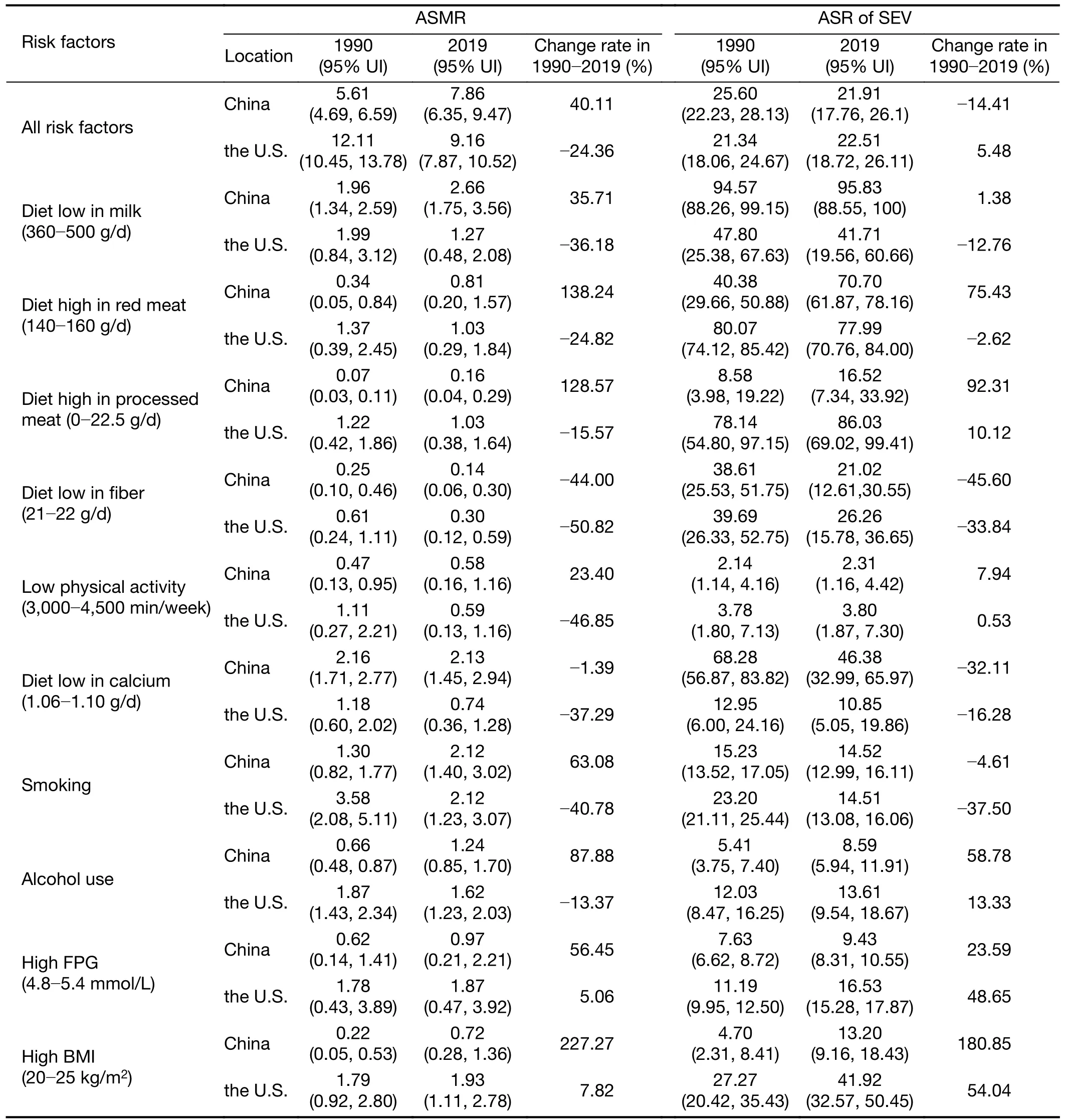
Table 3 ASMR and age-standardized summary exposure value rates attribute to risk factors for colorectal cancer and rate of changes in China and the U.S.between 1990 and 2019
Discussion
Based on the GBD 2019 database,we comprehensively compared CRC burden and changes in major risk factors between China and the U.S.We found that the CRC burden has kept increasing over the past 30 years in China,with ASIR,ASMR,and ASR of DALY increased largely;while those in the U.S. showed decreasing trends.Compared with the U.S.,lower ASIR and ASMR rates were observed in China (16-18).The leading risk factor contributing to CRC death in China was low milk,and it was smoking in the U.S.
The CRC burden in China continued to increase compared with the decreasing trends in the U.S.Previous studies have reported the difference between the two countries (18-22).The decreasing trend was partly attributable to the implementation of national CRC screening in the U.S.The “adenoma-carcinoma” sequence is the basis for the development of CRC.The progression generally takes 5-10 years,so there is ample opportunity for early detection and therapeutic action (23).CRC screening,with colonoscopy as the main tool,is more advantageous in terms of early diagnosis and intervention(24).In the U.S.,the CRC screening program began in the 1980s and has gradually been promoted.Because the coverage of colonoscopy screening increased from 21% to 60% between 2000 and 2015,the CRC incidence in the U.S.declined rapidly after 2000 (25).Moreover,it could be found that a greater decreasing trend of CRC incidence was partly offset when including the demographic effect(Supplementary Table S1).We found that the actual CRC burden in the U.S.was decreasing,and the main reasons for the net increment were the aging of society and population size.In contrast,there was an increment in the CRC burden in China.China started large-scale CRC population screening in Haining County,Zhejiang province in the 1970s.Since then,CRC screening has been carried out in both urban and rural locations in the north and south of China (26),even though there is currently no nationwide organized CRC screening program (27).The effectiveness of cancer screening mainly depends on the population coverage and adherence of the target population.Nevertheless,so far the scope of CRC screening remains the modest in China.Results from a high-risk urban population CRC screening with 182,927 participants have revealed that the total screening colonoscopy participation rate was 14%,and the rate of advanced colorectal neoplasia detection among the highrisk group undergoing colonoscopy was 3.32% (28).
From 1990 to 2019,the burden of CRC in China has increased dramatically and has become a more serious problem in China,which was consistent with the conclusions of previous Chinese epidemiological studies(16-18).This increase could be interpreted by the association of the rising socioeconomic status (29),changes in dietary habits (12),and westernized lifestyle (30) with the CRC burden.In addition,the burden increased more prominently in males as well as the overall burden was lower in females than in males,which was in line with the previous studies (20,31,32).This gender disparity may be caused by the fact that males often face greater health risks,such as overweight or obesity,smoking,alcohol use,high red meat intake,and insufficient physical activity (33).In addition,some studies have shown a protective effect of estrogen and oral contraceptive use on the occurrence of CRC in females (5,11).
The age distribution showed that age played an important role in risk factors associated with CRC,with lower incidence and mortality in younger people under 50 years old and a rapid increase with age after 50 years,indicating that the prevention and control of CRC should focus on the middle-aged and elderly population.This observation has been supported by previous studies (5,16),and in the U.S.,the recommendation to begin regular screening in people aged 50 years is a strong recommendation (34).The increment in sigmoidoscopy coverage in people over 50 years old is credited to the successful promotion of the screening programs (25).
The number of CRC patients diagnosed was much higher than that reported by National Cancer Center Registry (NCCR) (60.79 per 100,000 in 2019vs.40.8 per 100,000 in 2016).Notably,females in China also showed a higher increment in incidence compared with data from NCCR (AAPC: 2.16vs.1.20) (35).This could be explained by the different data sources used and the fact that the GBD estimates were reconstructed using sources of varying quality (1).In the GBD study,the main source of data for China is surveillance data from the China Disease Surveillance Points (DSP) system.The DSP estimates are based on the number of cases reported by the disease surveillance points (Supplementary Table S2),representing about 24% of the country’s population (36).In the NCCR of China,data are reported across 682 disease surveillance points (487 were included),representing 27.6% of the national population in 2016 (35).Established in 2002,the NCCR normative reporting started relatively late compared with the GBD estimation,which covers national data for 30 years as well as becomes the only official way to access national data for such a long period (1,37).On the other hand,the study periods were disparate and our analysis showed that females in China had a rapid increase in incidence from 2016 to 2019 (APC=3.65).
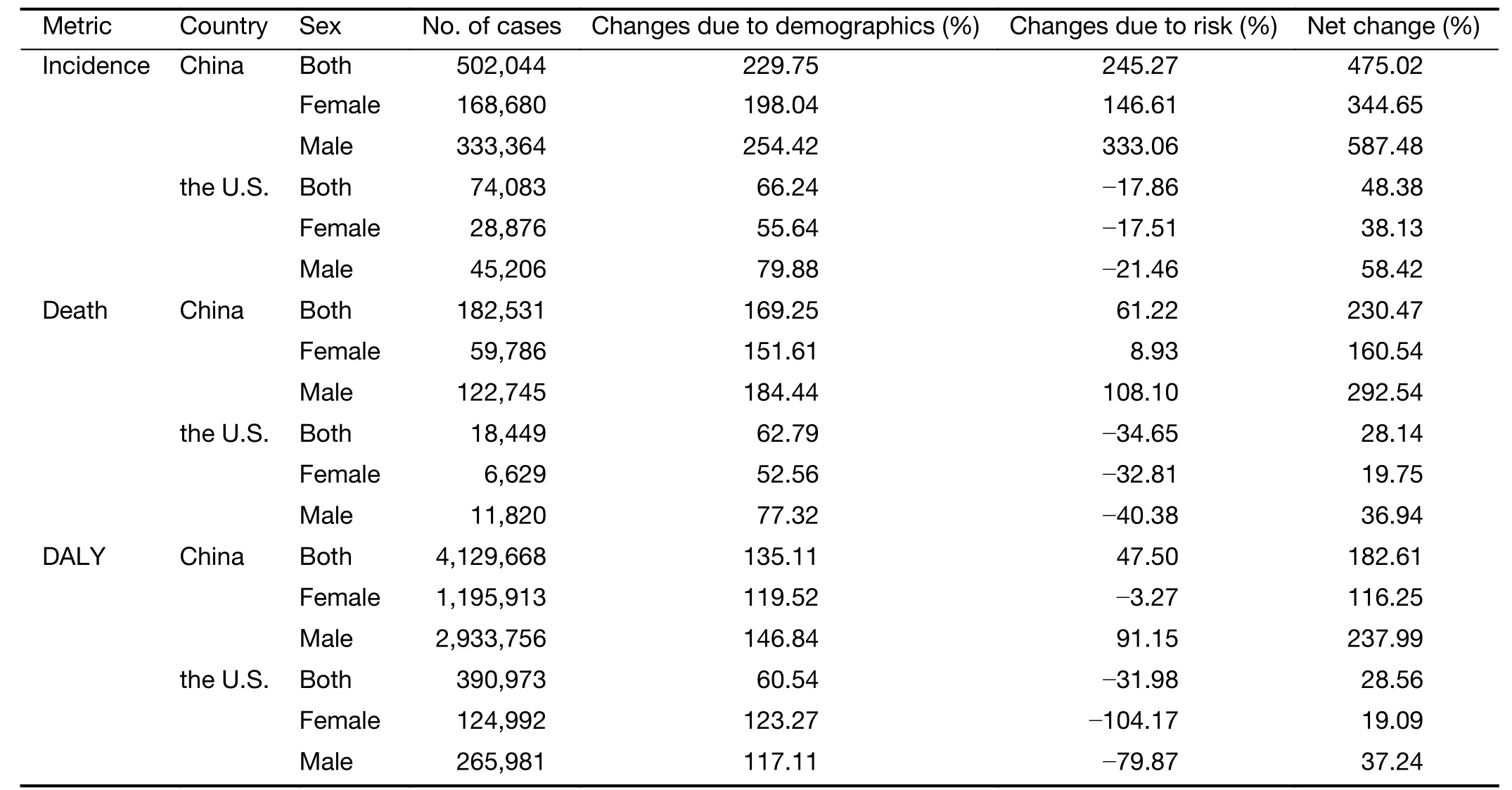
Table S1 Changes in No.of cases of colorectal cancer from 1990 to 2019 apportioned into changes due to demographics and risk
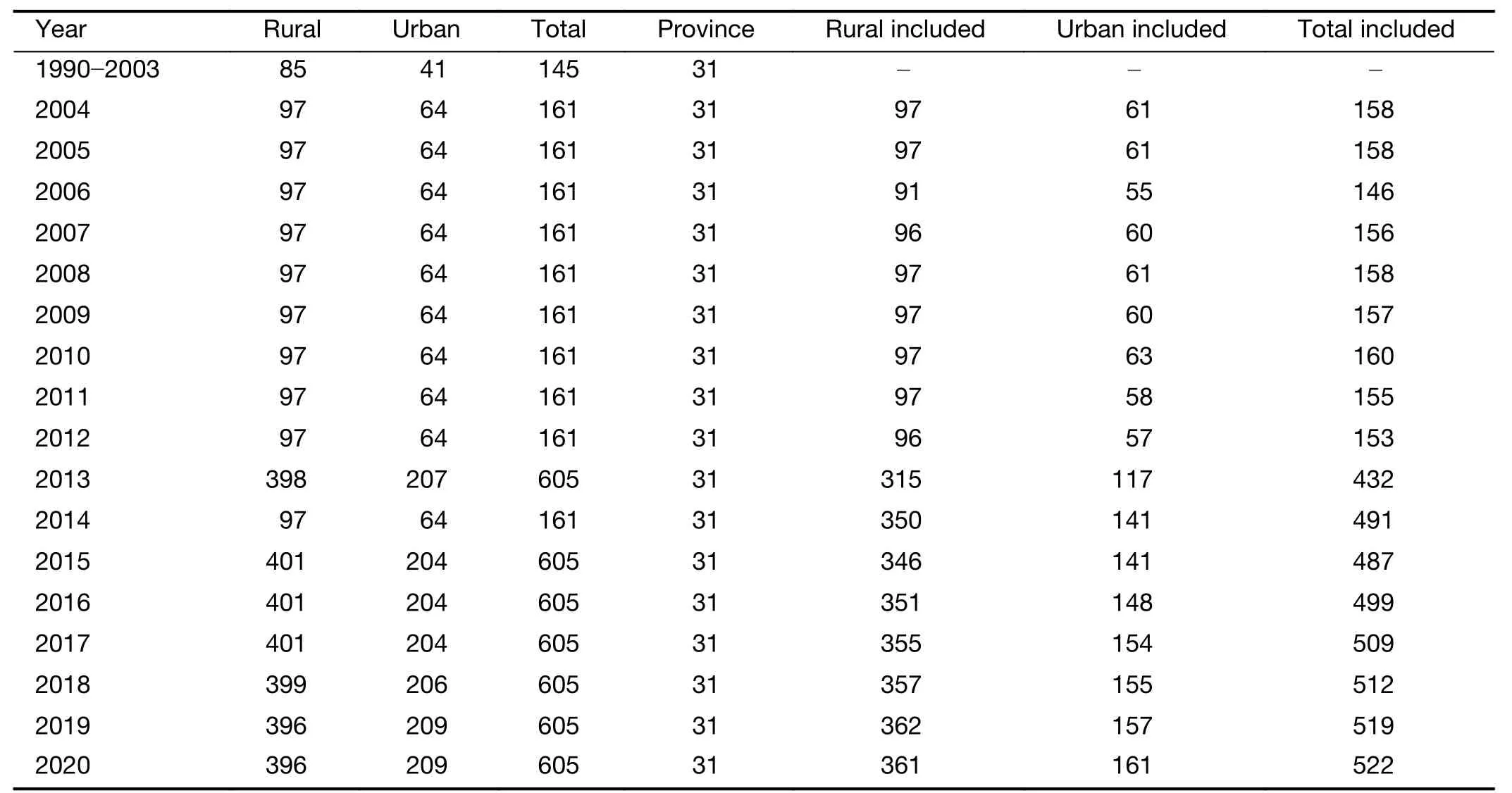
Table S2 No.of China Disease Surveillance Point system registries from 1990 to 2020
This study reported that smoking played a prominent role in CRC death in both countries.The number of smokers in the U.S.has steadily decreased from 37.4% in 1971 to 14% in 2019 (38),whereas the smoking rate of Chinese males was still more than 50% from a recent report (39).Compared with the U.S.,measures could be taken to reduce the smoking rate,which might be an effective and feasible way to prevent CRC in China.Additionally,we found that diet low in milk contributed the most to CRC death in China in 2019,which is the main risk factor for CRC around the world as well (40).In the previous study,high consumption of dairy products and the protective effects attributed to calcium and vitamin D levels might be inversely connected with the risk of CRC (41).Moreover,overweight,obesity,and excessive intake of red and processed meat contribute to important factors in the occurrence and death of CRC (42).In recent data,the proportion of obese people was increasing in China over years,but the average daily intake of alcohol and moderate or higher intensity physical activity improved little (43).Therefore increasing physical activity could be the most direct preventive method.Mortality due to excessive intake of red and processed meat products also increased rapidly in China,which was in line with previous studies (44,45).These findings indicate that the carcinogenic compounds from the red and processed meat will form when meats are cooked at high temperatures.Results have also shown that dietary patterns have shifted with socioeconomic development.In low-and middle-income countries,consumption of fat,sugar,and foods like red meat and processed meat has increased,whereas it has stabilized in high-income countries (22,45).
The study has several limitations.First,GBD data are derived from estimation and mathematical modeling(1,10,46).Second,colon cancer and rectal cancer were not analyzed separately in this study,and their trends could not be shown respectively.The dataset used in the study was from public databases and lacked pathological types,which would be a more valuable reference for health policy formulation if trend analysis of pathological types could be performed.Finally,GBD 2019 had only national-level data,which could not analyze the differences in CRC in the regional,provincial,and urban-rural areas of China.
Conclusions
ASRs of incidence,death,and DALY of CRC increased in China but decreased in the U.S.during the past three decades. Males and middle-aged and elderly people suffered a heavier disease burden of CRC.The high burden of CRC attributed to relevant risk factors suggested the
need for enhanced prevention and management of CRC risk factors.
Acknowledgements
This study was supported by the Sanming Project of Medicine in Shenzhen (No.SZSM201911015).
Footnote
Conflicts of Interest: The authors have no conflicts of interest to declare.
 Chinese Journal of Cancer Research2022年5期
Chinese Journal of Cancer Research2022年5期
- Chinese Journal of Cancer Research的其它文章
- Characteristics of lymph node stations/basins metastasis and construction and validation of a preoperative combination prediction model that accurately excludes lymph node metastasis in early gastric cancer
- Correlation between imaging features on computed tomography and combined positive score of PD-L1 expression in patients with gastric cancer
- Evaluation of triage strategies for high-risk human papillomavirus-positive women in cervical cancer screening: A multicenter randomized controlled trial in different resource settings in China
- Myeloid checkpoints for cancer immunotherapy
- National guidelines for diagnosis and treatment of malignant lymphoma 2022 in China (English version)
- Beyond images: Emerging role of Raman spectroscopy-based artificial intelligence in diagnosis of gastric neoplasia