
Dermatoscopy in the Diagnosis of Vulvar Basal Cell Carcinoma: A Case Report
2022-07-06 08:53DiegoAdolfodelosCobosDavaiosRodrigoCepedaValdesLuisFernandoFavelaFernandezClaudiaVillarrealCarrillo3JulioCesarSalasAlanis
國際皮膚性病學(xué)雜志 2022年2期
Diego Adolfo de los Cobos Davaios*, Rodrigo Cepeda-ValdesLuis Fernando Favela-Fernandez Claudia Villarreal-Carrillo3, Julio Cesar Salas-Alanis
1Debra Mexico, Guadalupe, Nuevo León 67150, Mexico; 2Julio Salas Dermatology, Guadalupe, Nuevo León 67150, Mexico;3Facultad de Medicina, Universidad Autónoma de Nuevo León, Monterrey, Nuevo León 67150, México.
Abstract
Keywords: basal cell carcinoma, cancer, case report, latino, tumors, woman
Introduction
Basal cell carcinoma (BCC) is the most common human malignancy, representing 75% of nonmelanoma skin cancers.1BCC is most frequently located on the sunexposed skin areas of the head and neck, but appears in unexposed areas such as the perineal and anal regions in less than 1% of cases.2-3Vulvar BCC is rare, accounting for approximately 3%of vulvar cancers;2such lesions are often diagnosed late because they grow slowly and tend to be asymptomatic, with no specific physical findings.4
Case report
A 65-year-old Latino woman presented with a nodule on her left labium majus(Fig.1).She had first noted the lesion 10years ago,and it had grown slowly but constantly since then. She also reported a 20-year history of pruritus and occasionalpainoftheleftlabiummajus.Thepatienthadnot received any previous diagnoses or treatments for the condition. There was no relevant medical history (the patient reported no history of cancer,sexually transmitted disease,humanpapillomavirus,irradiation,ortobaccouse)orfamilyhistory.Physicalexaminationrevealeda3.5×3.0 cm oval,erythematous lesion with a central rough,fissured surface. All other physical examination findings were normal,with no inguinal lymphadenopathy noted.

Figure 1. Clinical features of a Latin patient with vulvar basal cell carcinoma. An oval, erythematous lesion with a central rough,fissured surface measuring 3.5cm×3.0cm was observed on the left labium majus without inguinal lymphadenopathy noted.
Contact dermatoscopy (Dermalite DL3 Gen) showed one blurred cluster of arborising vessels on a pinkish background with white homogeneous areas and converging radial lines (Fig. 2). Based on histopathological examination of an incisional biopsy, the lesion was diagnosed as a BCC.
Discussion
Vulvar BCC is a rare malignancy that mainly affects Caucasian women older than 70years but can occur in younger patients of all races,with the youngest registered patient being a 20-year-old nulligravid African American woman.1,4Vulvar BCC presents most frequently in the labia majora as an eroded pigmented plaque in 3%of the Caucasian population and up to 81% of Chinese patients;2,5however, vulvar BCC may also present as multiple, bilateral, or disseminated lesions,3or as ulcerated lesions in 28% of Caucasian patients.6
The most common etiology for BCC is ultraviolet radiation exposure; however, as the vulva is unexposed,the cause of vulvar BCC is unclear. Mutations in tumor suppressor and regulatory genes such as p53 are present in 50%of patients with BCC.4The reported risk factors for BCC include Gorlin syndrome,chronic radiation,chronic arsenic exposure,xeroderma pigmentosum,and immunosuppression.7BCC has also been associated with lichen sclerosis,5Pagetdisease,8localtrauma,scars,andadvanced age.6,8
BCC has no specific features and can present as an asymptomatic lesion,pruritus,irritation,pain,discomfort,bleeding, or a palpable mass.3Vulvar BCC is most frequently misdiagnosed as inflammatory diseases, such as eczema,psoriasis,and chronic infection(especially when accompanied by pruritus),but must also be differentiated from Bowen disease,Paget disease,squamous cell carcinoma, melanoma, melanocytic nevus, seborrheic keratosis,pemphigus vegetans, and other vulvar tumors.7,9This makes the diagnosis of vulvar BCC complex, with an average diagnostic delay of 5 to 6years,7and an average lesion size of 2.1cm.6Furthermore,the width of the BCC may not be directly related to the depth of invasion.5The diagnosis of BCC is enhanced by dermatoscopy, as the dermatoscopiccharacteristicsofvulvarBCCarethesameas those of other cutaneous forms,featuring blue ovoid nests and arborizing telangiectasia.3,9
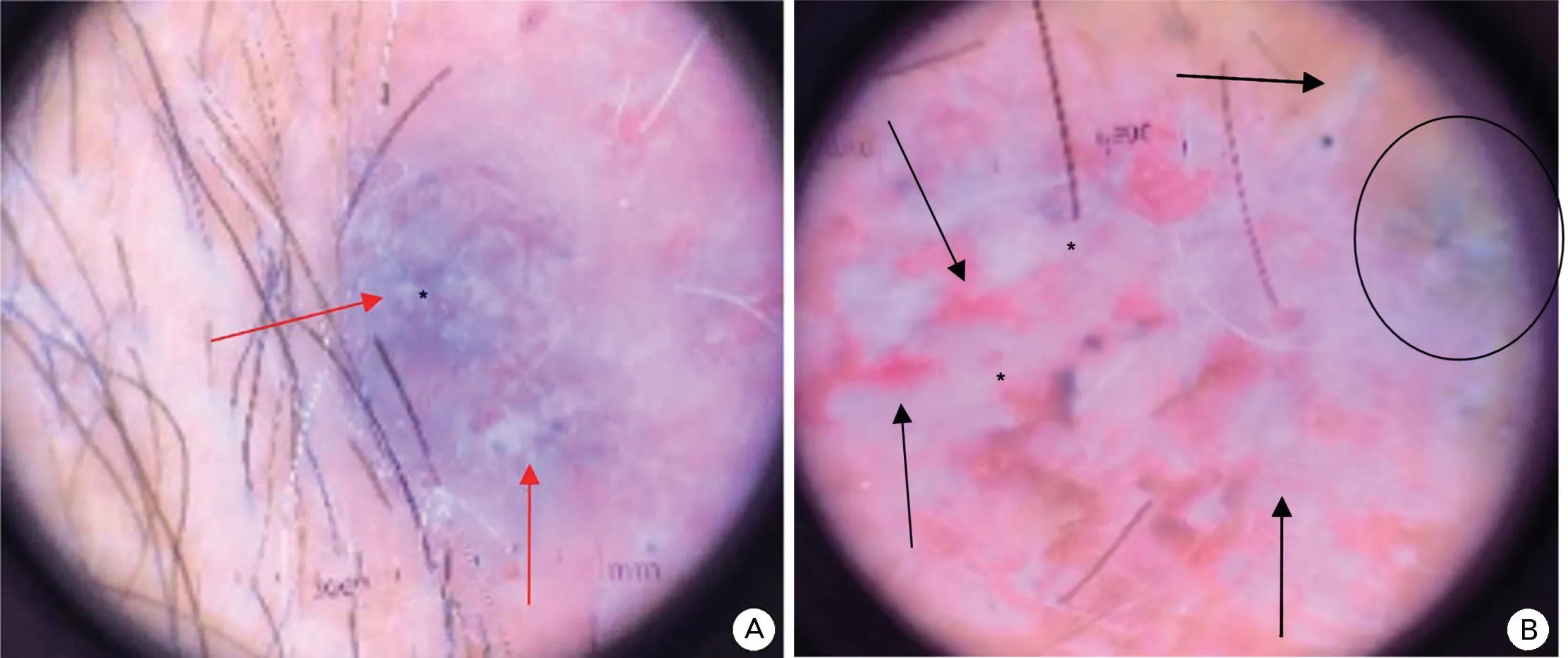
Figure 2. Dermatoscopy features of a Latin patient with vulvar basal cell carcinoma(×4).(A and B):Dermatoscopy shows a blurred cluster of arborizing vessels(black arrows in B)on a pinkish background with white homogeneous areas(red arrows in A)and converging radial lines(black circle in B).
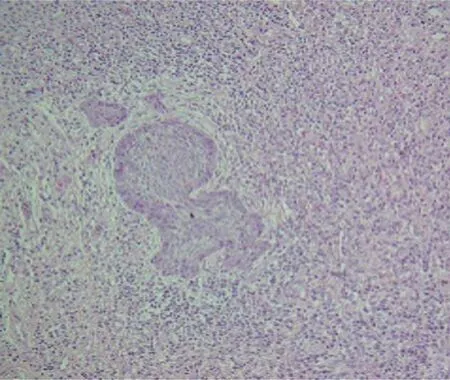
Figure 3. Histopathological features of a Latin patient with vulvar basal cell carcinoma(H&E,×10).A pigmented epidermis from which confluent nodules formed of basaloid tumor cells with peripheral palisading extend towards the middle and deep dermis,surrounded by a fibrovascular stroma with abundant mucin.
The preferred treatment in most cases of BCC is wide surgical excision, although local recurrence is possible if the margins are positive.4The margins cannot be easily observed with the naked eye, leading to positive margins after excision, with 25% of cases requiring a second intervention.10Dermatoscopy may aid in determining tumor margins, but is not exact. Patients with more advanced or aggressive tumors may benefit from Mohs micrographic surgery, which enables the intraoperative examination of margins and provides relative certainty that the margins are negative with minimal sacrifice of normal tissue.4

- 國際皮膚性病學(xué)雜志的其它文章
- Clinical Features and Corrected Factors with Neurosyphilis in HIV/Syphilis Co-Infected Patients Based on Stage of Syphilis
- Dermoscopic Features of Basal Cell Carcinoma and Their Association with Histological Types in A Chinese Population: A Perspective Study
- p62/SQSTM1 Participates in the Innate Immune Response of Macrophages Against Candida albicans Infection
- Frostbite in Southwest China: A Single-Center Retrospective Analysis
- Role of Epigenetics in the Pathogenesis of Systemic Sclerosis
- Skin Organoid Research Progress and Potential Applications