
Frostbite in Southwest China: A Single-Center Retrospective Analysis
2022-07-06 08:53YueXiaoDingKeWenDanHaoYanMeiLiXianJiang
國(guó)際皮膚性病學(xué)雜志 2022年2期
Yue Xiao, Ding-Ke Wen, Dan Hao, Yan-Mei Li, Xian Jiang,*
1Department of Dermatology, West China Hospital, Sichuan University, Chengdu, Sichuan 610041, China; 2Laboratory of Dermatology, Clinical Institute of Inflammation and Immunology, Frontiers Science Center for Disease-related Molecular network,West China Hospital, Sichuan University, Chengdu, Sichuan 610041, China; 3Department of Neurosurgery, West China Hospital,Sichuan University, Chengdu, Sichuan 610041, China.
Abstract
Keywords: frostbite, amputation, prognosis, Southwest China
Introduction
Frostbite is caused by the skin and underlying tissue freezing, with ice crystals forming in and between cells.1Severe frostbite is considered one of the most devastating injuries among all types of cold-induced abnormalities.2The morbidity and mortality rates of severe frostbite are increasing in the northern regions of China.3The present retrospective observational study aimed to describe the demographic features of patients treated for frostbite at a single center in Southwest China as the data of frostbite was scarce in this region. However, there is little documentation of frostbite in the southwestern regions of China. Southwest China differs drastically from the northern regions regarding its mountainous terrain and diverse ethnicity.In this retrospective observational study,we evaluated the demographic and clinical differences between two patient populations with frostbite: Tibetan and Han,and discussed the factors affecting the outcome of severe frostbite in Southwest China.
Patients and methods
Patient selection
Patients with frostbite admitted to West China Hospital fromJanuary1st,2009,toJanuary1st,2019,werescreened for inclusion.Patients’medical records were retrieved from the Research System by searching with term “frostbite.”Patients without a complete description of the physical examination findings or laboratory test results were excluded (Supplementary Fig. 1, http://links.lww.com/JD9/A16).This study was approved by the department of clinical trial management,West China Hospital of Sichuan University,to obtain clinical data retrospectively.
Clinical data
Patient information was collected from the hospital information systems.Demographic and clinical data were summarized, including age, sex, ethnicity, time from frostbite onset to admission, frostbite location, frostbite severity, operative intervention, and length of stay.Admission blood test results were also documented,including the red blood cell (RBC) count, hemoglobin(Hb), hematocrit (Hct), mean corpuscular volume, mean corpuscular Hb, mean corpuscular Hb concentration,white blood cell count,neutrophil granulocyte percentage,platelet count, alanine aminotransferase level, aspartate aminotransferase level, albumin level, prothrombin time,activated partial thromboplastin time,and fibrinogen level.The severity of frostbite was classified into four grades,which can be simply classified as superficial (1stand 2nddegree) and deep (3rdand 4thdegree) frostbite.1Deep frostbite often required surgery to remove the devitalized tissue.Two researchers independently and blindly evaluated the frostbite grade based on a description of the physical examination findings(Supplementary Table 1,http://links.lww.com/JD9/A17).We modified Glasgow Outcome Scale and built a functional independence scoring algorithm of amputees to retrospectively define patients with a poor outcome as those who were partially able to perform selfcare but lacked the competence to return to work or study(Supplementary Table 2,http://links.lww.com/JD9/A18).4
Statistical analyses
Categoricalvariableswereshownasfrequency(percentage)and analyzed using the Chi-squared test or Fisherexact test.Continuous data were presented as mean ± standard deviation and analyzed using the Student t-test.All analyses were performed using SPSS 23.0 (SPSS inc., Chicago, IL,USA),and the significance level was set as P <0.05.
Results
Demographic and clinical characteristics of patients with frostbite
In this study,data of 27 patients were collected,with age ranged from 14 to 81 years, and most patients were younger than 20 years(41%,11/27).Most patients were male,while only 15%were female.The ratio of Tibetans versus Hans was 13:14. The most common frostbite site was the lower extremities (74%, 20/27) followed by the upper extremities (63%, 17/27), whereas the ears and perineum were least commonly affected. The mean prehospital delay was 10 days (range 1-48 days),suggesting that none of these patients met the criteria for thrombolytic therapy;this was mainly due to the delay in admission,frequent freeze-thaw cycles,and the variable length of stay ranging from 2 to 104 days (Table 1).
We classified the patients based on the classification scheme for severity of frostbite. Most patients were categorized as having severe frostbite(85%,23/27),while only 15% were considered to have minor frostbite. As tissue loss is generally regarded as a major indicator of an unfavorable outcome for frostbite, we investigated the amputation rate of the patients with severe frostbite.Amputation surgery was performed for nearly half of the patients with severe frostbite(43%,10/23)versus none of the patients with mild frostbite (Table 1). To clarify the potential factors contributing to amputation among patients with severe frostbite, we compared the bloodtest results of patients with and without amputation.However,the blood test results did not significantly differ between these two groups (Table 2).
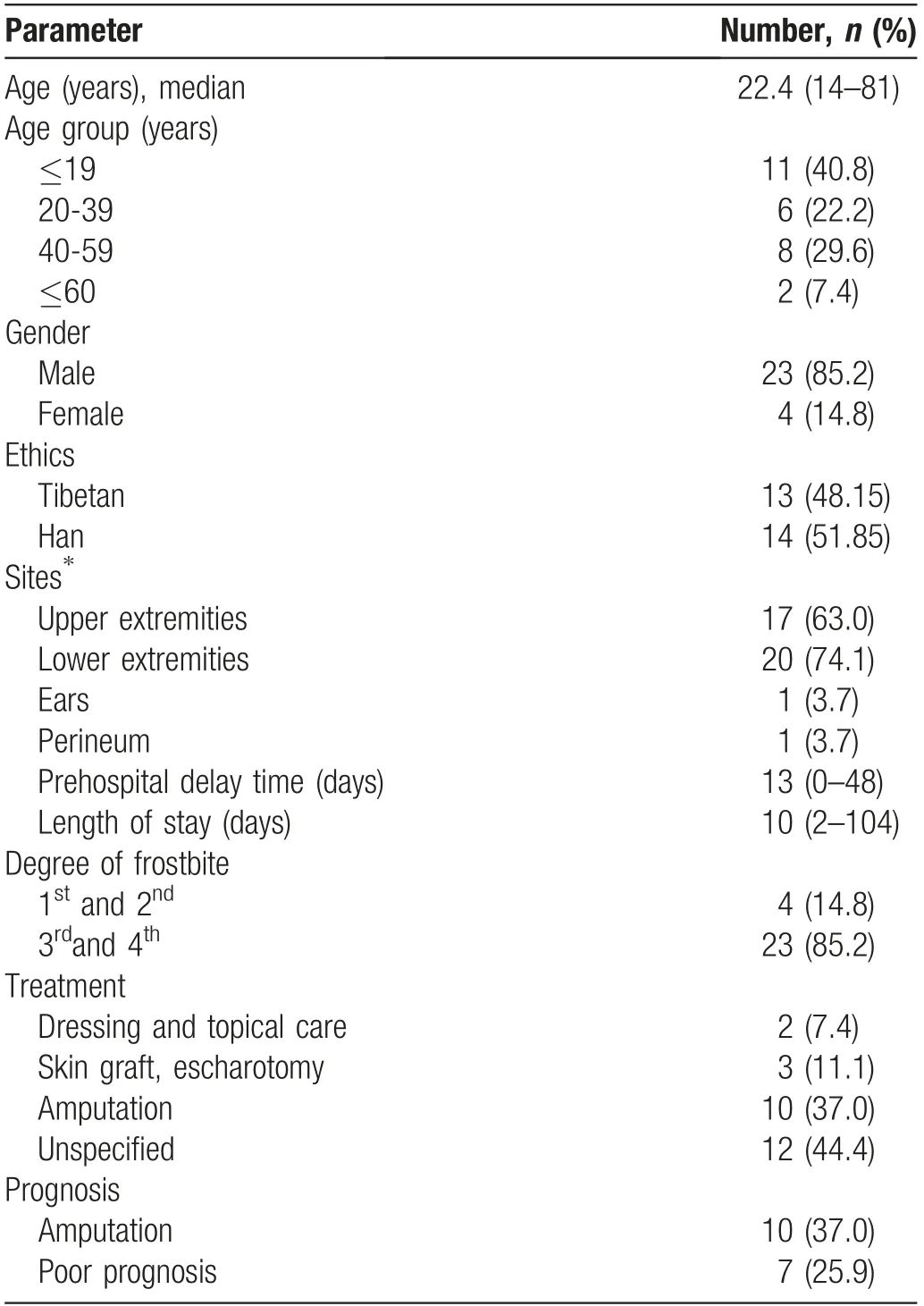
Table 1 Demographic characteristics of frostbite in a single center.
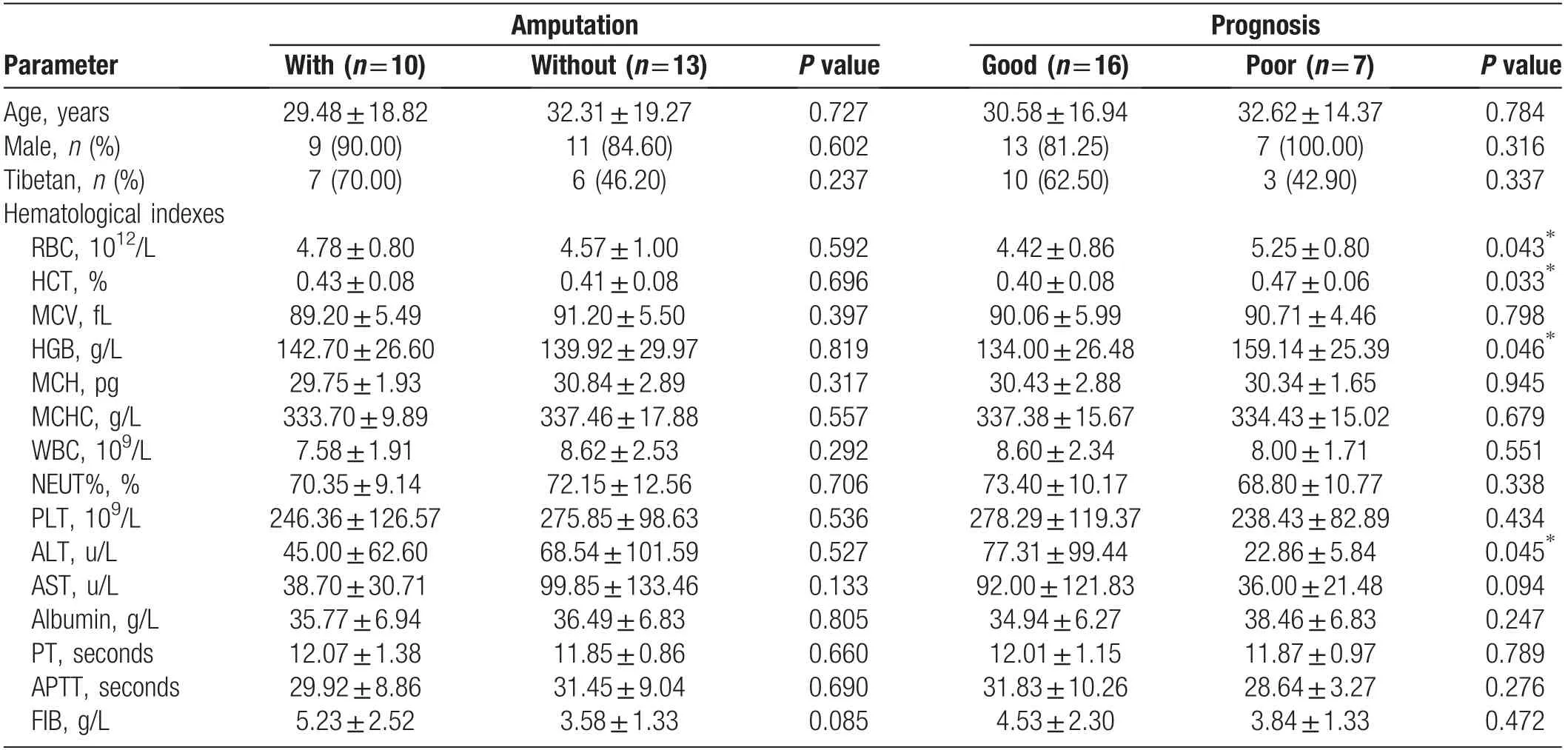
Table 2 Differences of clinical characteristics among patients with severe frostbite (mean±standard).
Considering that amputation and tissue loss may not equal the eventual functional outcome, we used a functional independence scoring algorithm to further study the differences between patients with a poor functional outcome and those with a good functional outcome (Supplementary Table 2, http://links.lww.com/JD9/A18). Based on this scale, seven patients were categorized as the poor outcome group, while 20 were categorized as the good outcome group.A comparison of the blood parameters in patients with good versus poor functional outcomes revealed a significant intergroup difference in the RBC count,Hct,and Hb level(P <0.05)(Table 2).
Time and reason distribution of frostbite
All frostbite injuries were incurred from September to April, with the incident rate peaking in December,January, and February (Fig. 1A). For Tibetans, cold injuries were mainly caused by winter outdoor activities like intentional long exposure to extreme weather during pilgrimage (70%, 9/13). For Hans, the most common reason for frostbite was accidental long-time cold exposure during work,like liquid nitrogen leakage repair,followed by psychological disorders such as dementia,schizophrenia, and drunkenness (Fig. 1B).
Discussion
This research revealed the distinctive demographic and clinical profile of patients with frostbite in a single medical center in the southwestern Chinese region inhabited by Tibetan and Han people.5-9Despite similarities in residence and living habits, the two populations developed frostbite owing to specific reasons.In the current study,pilgrimage accounted for 70%of all frostbite cases in Tibetan patients,whereas the Han patients with frostbite shared more epidemiologic similarities with patients in other regions especially cities.8-10
Most Tibetans live in the high-altitude mountainous regions in the Sichuan province and Qinghai-Tibet region and follow Tibetan Buddhism. For Tibetan Buddhists,pilgrimage is an essential and common sacred ritual comprising a nonstop pedestrian march from their homes to the Potala Palace. This nonstop travel exposes the Tibetan Buddhists to extreme weather patterns such as blizzards, often without proper shelter for an extended period.Moreover,hospital admission may be delayed due to the intentional endurance of cold-induced symptoms,which contributes to patients missing a valuable time window for thrombolytic therapy. As our center is often not the primary care-providing institute for these patients,caution should be taken in these primary triage centers to rapidly identify these patients and perform timely intervention, including faster assessment, rewarming,prehospital thrombolysis, or telemedicine to improve the functional outcome.1,11

Figure 1. The time distribution and reason analysis of frostbite in southwest China.(A)Time distribution of frostbite.(B)Reasons for frostbite in Tibetans and Hans.
Under the standardized protocol, patients with severe frostbite who are rewarmed rapidly and transferred to a hospital within 6-24 hours without repeated freeze-thaw damage can receive tissue plasminogen activator, which dissolves microvascular thrombi and restores blood flow before the occurrence of irreversible tissue necrosis.1,12However, patients with frostbite often do not meet the strict criteria for thrombolytic therapy.13Most patients admitted to our center were in the final stage, with bad body conditions.For example,a 19-year-old Tibetan man who accidentally soaked his feet in a creek while on pilgrimage was transferred to our center 4 days after the onset of symptoms. In the current study, none of the patients received thrombolytic therapy due to inadequate basic medical protocols for frostbite in the local hospitals,exposure to freeze-thaw cycles, and delayed transfer to our center. This lack of thrombolytic therapy markedly affects the chances of salvaging the affected limb/digit and the outcome, especially for severe cases. The current findings strongly indicate that the frostbite management protocols used in regional hospitals in West China are inadequate, as these hospitals generally do not see many patients with frostbite.
We summarized the precautions and therapeutical measures used to treat severe frostbite.14-16
Precautions to prevent frostbite: (1) Wear appropriate clothing,including warm clothing that is not tight,gloves,a mask, and a hat. (2) Keep dry. (3) Intake sufficient energy and oxygen. (4) Monitor for early symptoms of frostbite such as numbness, a stabbing sensation, and white skin appearance.
Prehospital therapeutic measures for frostbite: (1) Get out of the cold environment and into a shelter as soon as possible.(2)Remove wet clothes.(3)Soak limbs in warm water at 37-39°C. (4) Avoid freeze-thaw cycles.
Frostbite treatment: (1) Debridement. (2) Elevate extremities to decrease edema. (3) Administration of analgesia and antibiotics.(4)Tetanus toxoid prophylaxis.(5) Administer tissue plasminogen activator within 24 hours of rewarming. (6) Perform amputation surgery if necessary (watch and wait for tissue demarcation before amputation).
Although it is well-accepted that the hallmark of a poor outcome in patients with frostbite is amputation and tissue loss, the occurrence of systemic inflammatory response syndrome might lead to multiple organ failure.Most previous studies have used different parameters to assess the frostbite severity because this assessment largely relies on caregivers’ subjective assessments in each institute.6,17Considering that amputation is also an appropriate management with which to prevent systemic infection when the affected extremities present with gangrene or irreversible tissue necrosis, the poor outcome does not necessarily indicate the incidence of amputation. The outcome of severe frostbite may be affected by multiple factors, including the duration of prehospital delay, length of stay, and level of amputation. Therefore, when trying to clarify the factors associated with poor outcome, rather than using the conventional amputation categorization, we adopted a functional independence assessment algorithm performed by two blinded investigators. We predominantly evaluated the self-care ability and capacity to return to society; thus, patients with partially amputated toes and fingers were considered to have a better functional outcome than those with amputation of the lower extremities. This scoring system revealed that the RBC count, Hct, and Hb level were significantly associated with the outcome of patients with frostbite. However,the limited sample size might have biased the present results.Therefore,we suggest that it is insufficient to use amputation as the sole endpoint to determine the outcome of patients with frostbite. A more universal and detailed functional evaluation should be performed to optimize the post-treatment outcome.
The present study had some limitations. The small number of patients and retrospective single-center design may have biased the results. The results showed that the incidence of frostbite is affected by factors such as temperature, occupation, and activities. However, we could only analyze the data and observe trends rather than make statistically significant conclusions. In addition,potential confounding factors like the lack of access to transportation in remote areas and factors affecting hospital attendance should also be considered.However,this study was an initial attempt to study frostbite demographics in a non-typical cold region in China. A large-scale, clinical study in these populations might be helpful for providing a better clinical reference for frostbite treatment in such regions.
In conclusion,to avoid severe frostbite damage,routine mandatory activities like pilgrimage should be conducted under proper protection in extreme weather. Hematologi-cal indexes such as the RBC count,Hct,and Hb level should be monitored closely by first-line medical personnel during hospitalization, as these indexes might indicate the outcome of frostbite. Further research is advocated for the better management of frostbite in similar regions.
Acknowledgements
The authors would like to express their gratitude to the patients and their relatives for understanding and participating in our study.
Source of funding
The study was supported by the 1.3.5 project for disciplines of excellence, West China Hospital, Sichuan University (No. ZYJC21036), and National Natural Science Foundation of China (No. 82003373).

- 國(guó)際皮膚性病學(xué)雜志的其它文章
- Clinical Features and Corrected Factors with Neurosyphilis in HIV/Syphilis Co-Infected Patients Based on Stage of Syphilis
- Dermoscopic Features of Basal Cell Carcinoma and Their Association with Histological Types in A Chinese Population: A Perspective Study
- p62/SQSTM1 Participates in the Innate Immune Response of Macrophages Against Candida albicans Infection
- Role of Epigenetics in the Pathogenesis of Systemic Sclerosis
- Skin Organoid Research Progress and Potential Applications
- Dermatoscopy in the Diagnosis of Vulvar Basal Cell Carcinoma: A Case Report