
Hematological parameters in high altitude residents:Tibetan natives versus Han migrants
2014-01-22 10:41TianyiWUFengyunLIULingHUChunyinWEIZhigangWANGOuzhouLOUBUChaoyingCUBianbaXuebinQIBingSU
中國應用生理學雜志 2014年6期
Tian-yi WU, Feng-yun LIU, Ling HU, Chun-yin WEI,, Zhi-gang WANG, Ouzhou-LOUBU,Chao-ying CU, Bianba, Xue-bin QI, Bing SU
1. Department of Hypoxic Physiology and Mountain Sickness, High Altitude Medical Research Institute, Xining 810012; 2. High Altitude Medical Research Centre, University of Tibet, Lhasa 850000; 3. Department of Hematological Laboratory, Qinghai Cardiovascular Disease Hospital, Xining 810012; 4. State Key Laboratory of Genetic Resources and Evolution, Kunming Institute of Zoology, Academy of Science, Kunming 650023, China
Introduction
Tibetans are the oldest population living permanently on the Tibet plateau. Recently, we have reported a preliminary study on gender eあects the hemoglobin concentration in the Han and Tibetan population at various altitudes and found that hemoglobin levels were higher in Han than in Tibetan for both males and females [1]. However, there are multiple factors including altitude, age, gender, ethnic origin,menstruation, nutrition and illness which simultaneously affects the erythropoietic response to altitude hypoxia [2,3]. Understanding the causes of the variation is complex because each of these factors acting independently is likely to affect hemoglobin level and, in addition, they also can be act in concert.Furthermore, the magnitudes of the contribution of the various factors to the hemoglobin level could vary with altitude. Even simply considering altitude as the stimulus for the hemoglobin response, it is not known how variations in age, gender and ethnic origin, separately and together aあect hemoglobin concentration for a range of altitudes in any region of theworld. To describe the variation with altitude among health persons in relation to age, gender, and ethnic origin are necessary.
In addition, an attractive hypothesis is the age was a major contributing factor in chronic mountain sickness (CMS). In fact, Hb could be considered to show a continued increases with age for 20 to 70 years of age in Quechua Indians at Peruvian Andes [4,5]. However, an initially study by Wu et al [6] found no increase in Hb with age in Tibetan highlanders.More information is needed and it is a question that arises for discussion. Recently, an another biomedical problem is that the hypoxic hematological response related to menstruction. Peruvian altitude women who during premenopause presented a lower Hb values than men, whereas after the menopause, Hb increased dramatically and reach levels as the men[7,8]. CMS may appear later in women, who are protected during their reproductive years by the ovarian hormones [9], however, the relationship between Hb concentration and menstruation in Tibetan women is limited. Finally, studies have also been demonstrated the existence of genetic influence on hematological adaptation. そis is an area where data in humans have become available only recently [10,11]. In relation to this, the comparative population studies help to provide evidence of its great importance. そis report clarifies the situation by presenting data on Hb,Hct, and RBC values for a large samples of healthy Tibetan natives and Han migrants of known age, sex and occupation assessed at their different habitual altitudes (mean 2 664, 3 813, 4 525 m and 5 226 m) .
Materials and Methods
Areas
Due to the sparse and scattered population in the Qinghai-Tibetan Plateau, this survey was conducted over 23 years (1990-2012) in four geographic areas. All areas are located in the north-eastern and south-western part of the Plateau at 31-39°N and 89-103°E, and has a highland continental climate.(1) The Xining - Golmud area (Xining at 2 261m,Golmud at 2 801 m, and three neighboring agricultural villages at 2 560 m , 2 808 m, and 2 900 m) had a mean altitude of 2 664 ± 258 m. (2) Haibei area,six pastoral and agricultural villages in the area (3 719,3 750, 3 762, 3 790, 3 890, and 3 986 m) averaged 3 813± 96 m altitude. (3) Qingnan area: Seven villages in the mountainous pastures of the Qingnan area in the Kunlun and Bayankala Mountains (4 180, 4 200, 4 300,4 420, 4 650, 4 700, and 5 226 m) had a mean altitude of 4 525 ± 370 m. (4) In addition to the above, populations were sampled at 5 200 m in a Tibetan village known as Snow Mountain, near Mt. Animaqin.It is one of the highest inhabited communities in Tibet. Han Chinese, who had lived in the village for more than one year, were also studied.
Subjects
The investigation was carried out in 6 352 healthy adult high altitude residents of both sexes. Three thousands two hundreds of fifty-six subjects were Tibetan native highlanders. そe Tibetan lineage was by data of genealogy and the census register. A select Tibetans, only individuals who were born, raised and permanently reside at high altitude and had never traveled to lowlands were considered. All were lifelong altitude residents and had no known non-Tibetan ancestors. By occupation, Tibetans were mainly herders (84.0%), herders/farmers (12.6%) and laborers or officers (3.4%). Another 3 096 persons were Han Chinese migrants, who had been born and lived in the lowland below 1 000 m or near sea level, and had migrated to high altitude for at least more than one year, the length of time they had lived at high altitude ranging 1 to 48 years, the mean duration of altitude residence was 17.6 ±12.8 years. Han subjects were office workers or laborers (62.0%), or farmers(38.0%). Most of them descend to the lowlands for one month holidays every 1 to 3 years. To minimize influences from ambient pollution we favored agric-pastoral areas devoid of mining and without high population density. そe protocol was reviewed for the protection of human subjects by the Qinghai High Altitude Medical Research Institutional Committee on Human Research. Children and their parents were given detailed explanation of the purpose of the study and, for the younger children, permission was obtained from both parent and child. Older children gave their own permission.
We did not accept subjects who were the mixed ethnic stem (Han×Tib. or Tib.×Han). We chose only nonsmoking subjects, and who had not used drugs in recent weeks. If individual who reported or demonstrated evidence of any significant illness were excluded from the study.
Six hundreds and seven children (332 Tibetans,and 275 Han, the age range 5 to 15 years) were studied. Because it was strong reluctance and fear in the children to have blood drawn, so the sample sizes in both Tibetan and Han children were relatively small. We determined that age 16 as a delimitation between the adolescent and adult subjects, it is be-cause the young afer age 16 reach the age of puberty in boys and menarche in girls both in Tibetan and Han subjects at high altitude. Menstrual and obstetric histories were collected on all women those who had delivered within three months were excluded. In the present data, there was a comparison between the pre- and post-menopausal females, the non-menstruating girls being excluded from the premenopausal group.
Questionnaires
A questionnaire was used and distributed to all of the surveying persons, which covering age, sex, race,occupation, place of birth, length of time at lowland,length of migratory time at high altitude, current and past duration of altitude residence, history of smoking and drinking, past medical history, family history and chief complaints. Specifically, ancestry, health status, socioeconomic status and lifestyle of the participants were closed examined.
Physical examinations and laboratory tests
Physical examinations were performed. Blood pressure, resting electrocardiograph, pulmonary function test, chest roentgenography, blood gas (ABL 3 Automatic blood gas analyzer, Radiometers, Denmark),and oxygen saturation (by finger oximetry, Datex Ohmeda, Louiseville, CO, USA) were performed in each subject and will be reported elsewhere.
CMS criteria
Previously, we excluded patients with CMS the cutoff hemoglobin values> 23 g/dl was following the criteria of Carlos Monge C some 48 years ago [12].Using the recent international diagnostic criteria for CMS (Qinghai CMS score), a value of ≥ Hb 19 g/dl in females or ≥ 21 g/dl in males has been taken arbitrarily as the sole diagnostic criterion of CMS [13].そe study of 3 468 adult Tibetan and 3 382 adult Han subjects initially studied. According to the above criteria for acceptance of 3 256 adult Tibetan and 3 096 adult Han subjects were included in our final analysis.
Sea-level control standards
We utilized Tianjing (76 m) [14] and Shanghai (38 m)[15] as our sea-level adult and children standards,respectively. Taking the Tianjing means plus two standard deviations as the upper limit of sea level normal. Because there is no sea-level native Tibetan population in China, thus, the hematological values among Tibetans to be compared with Han sea-level standard for reference only.
Routine hematology
Blood samples were obtained by vein-puncture from resting, seated subjects collected in the morning, and immediately placed into two evaluated tubes. One (2 ml venous blood ) taken into a Wintrobe’s tube contain sodium heparin 0.2 mg was spun for hematocrit at 3 000 rpm for 30 min using a standard centrifuge(LXY-64 Model, Beijing Medical Machine Company)with a effective radius of 159 mm and speed of 50 rps. Use of longer centrifugation times for did not yield further lower Hct values. Hemoglobin concentrations were measured by the cyanometahemoglobin technique using a spectrophotometers (SM-571,Shanghai Medical Manufacture, Shanghai), which had been previously calibrated. Red cell count was carried out by classical microscopy techniques. All blood samples were analyzed immediately on site following collection. Mean corpuscular volume (MCV),mean corpuscular hemoglobin (MCH), and mean corpuscular hemoglobin concentration (MCHC) of both Tibetan and Han subjects were also calculated.Hematocrit and red blood cell values generally supported the trends in hemoglobin concentration(shown below in Table 2 and 3 in appendices). Because of the large volume of data, we have focused the analysis on the hemoglobin concentrations(shown below in appendices).
Statistical methods
Data were analyzed by using the statistical package(SAS version 9.0, SAS Institute, Cary, NC). For analysis, the entire data set was divided into four groups,Han males, Tibetan males, Han females and Tibetan females. Multivariate regression analysis for each group assumed the form: hemoglobin concentration(g/dl) = a + b× altitude (meters) + c× age (years),where b and c were β-coeきcients. そe gender comparisons were between Han and Tibetans. For males,we determined by Wald χ2tests whether the altitude and age coefficients from the multiple regression equations, with their standard errors, were diあerent between Han and Tibetans. We did a similar analysis for females. In addition, for illustration, we have presented descriptive statistics including mean and standard deviation, for altitude ranges and age classes for the entire cohort by ethnic group and gender. Linear regression analysis and correlation coeきcients were used to assess the relationship between variables.Data in Table 1 are reported as mean±SEM, and data in Table 2 and 3 are shown as mean±SD. Diあerences were accepted as significant when the probability (P)was P<0.05.
Results
As shown in Table 1, for each group, the number of subjects examined was greater than one thousand.The overall multiple regression in each of the four equations was statistically significant. Also noted in Table 1 is that the individual coeきcients for altitude and age were statistically significant, indicating that both of these variables aあected hemoglobin concentration for males and females in both Tibetan and Han. In fact, the variances shown (r2) indicated that 85 percent, or more, of the hemoglobin concentrations in the population groups studied could be accounted for by the combined variations in age and altitude. そe comparison of Tibetan and Han subjects,which was the primary aim of the study, showed that for both males and females, both the altitude and age coeきcients were larger in Han than in Tibetan subjects (Tab.1). そe multiple regression analysis, therefore, indicated that both age and altitude were factors aあecting hemoglobin concentration, and that in both males and females, these factors had a greater eあect on hemoglobin concentration in Han than in Tibetan subjects.
For presentation in Table 2 and Table 3 (hemoglobin concentration), the data obtained for each altitude range were divided into age classes analogous to age classes published previously by Leon-Velarde et al [8] for Peruvian subjects. In order to determine if the values shown in Table 2 and Table 3 reliably represented the hemoglobin concentrations for our populations, we calculated (from the regression equations in Table 1) hemoglobin at the mid point of the age classes for each altitude. そe regression equations predicted the hemoglobin values for the classes in Table 2 and Table 3 with an overall mean difference of +0.2 g/dl+0.01(SEM)hemoglobin concentration. そerefore, we considered that for purposes of demonstration, we could reliably use the data from Table 2 and 3 to illustrate factors aあecting hemoglobin concentration at altitude.
Hemoglobin diあerences: Han minus Tibetan (eあect of ethnic group)
Using the data from Table 2 and 3, the diあerences in hemoglobin concentration between Han and Tibetan subjects could be displayed by comparing the two ethnic groups for the same altitude range and age classes. In male subjects, panel A, the points representing the diあerences in hemoglobin concentration(Han minus Tibetan) were positive values (Fig.1).Furthermore for each of the three age groups, the differences progressively increased with increasing altitude. そat is, Han subjects tended to have higher hemoglobin values than the Tibetan subjects and this diあerence increased with increasing altitude. Above 2 664 m, hemoglobin diあerence increased about 1.0 g/dl for every 1 000 m increase in altitude.
In females, panel B, the points representing the Han minus Tibetan differences in hemoglobin concentration were also positive values, consistent with a trend for Han females to have higher hemoglobin values than Tibetan females (Fig.1B). Also for each of the three age groups, the diあerences at the highest altitude tended to be greater than at the lowest altitude,but the diあerences were relatively small compared to males. そus, while Han females tended to have higher hemoglobin values than Tibetan females, above 2 664 m, the hemoglobin difference increased only about 0.3 g/dl for every 1 000 m increase in altitude,which was less than in males.
Hemoglobin diあerences: male minus female (eあect of gender)
Because as noted in Figure 1, above, gender appeared to be an important association in the hemoglobin diあerences between Han and Tibetan, we examined the gender eあect for the two ethnic groups using the difference in hemoglobin (male minus female) for age class at each altitude (Fig. 2). In Tibetan children,panel A, boys had hemoglobin values similar to those of girls at any of the altitudes examined. For Tibetan adults, panel A, although the male-female diあerence values were all positive, there was no increase in the gender-related difference with increasing altitude.The data in Tibetans suggested, therefore, that in adults, but not in children, males tended to have higher hemoglobin levels than females, but in neither children nor adults did a gender-related difference increase with altitude.
For Han children, panel B, boys tended (P>0.05)to have higher hemoglobin values than girls, but these differences were not significant for altitudes up to 4 525 m. Above 4 525 m there were few children in the sample.For Han adults, panel B, the male-female difference values were all positive and in addition, there was an increase in this gender-related difference with increasing altitude. そe data in Han suggested,therefore, that in adults (and possibly in children),males tended to have higher hemoglobin levels than females. Furthermore, in adults (and possibly in children), this gender-related difference increased with altitude. The illustrated data in Tibetans and Han,taken together, suggested that increasing altitude exaggerated the male minus female hemoglobin difference in Han subjects, but not in Tibetan subjects.そe implications were that being a mature male was a more important factor increasing hemoglobin at high altitude in Han than in Tibetans.

Tab. 1 Multiple regression equation for hemoglobin concentration in terms of altitude and age for each of four groups of residents of Tibet, where b and c, respectively, represent coefficients for altitude and age.
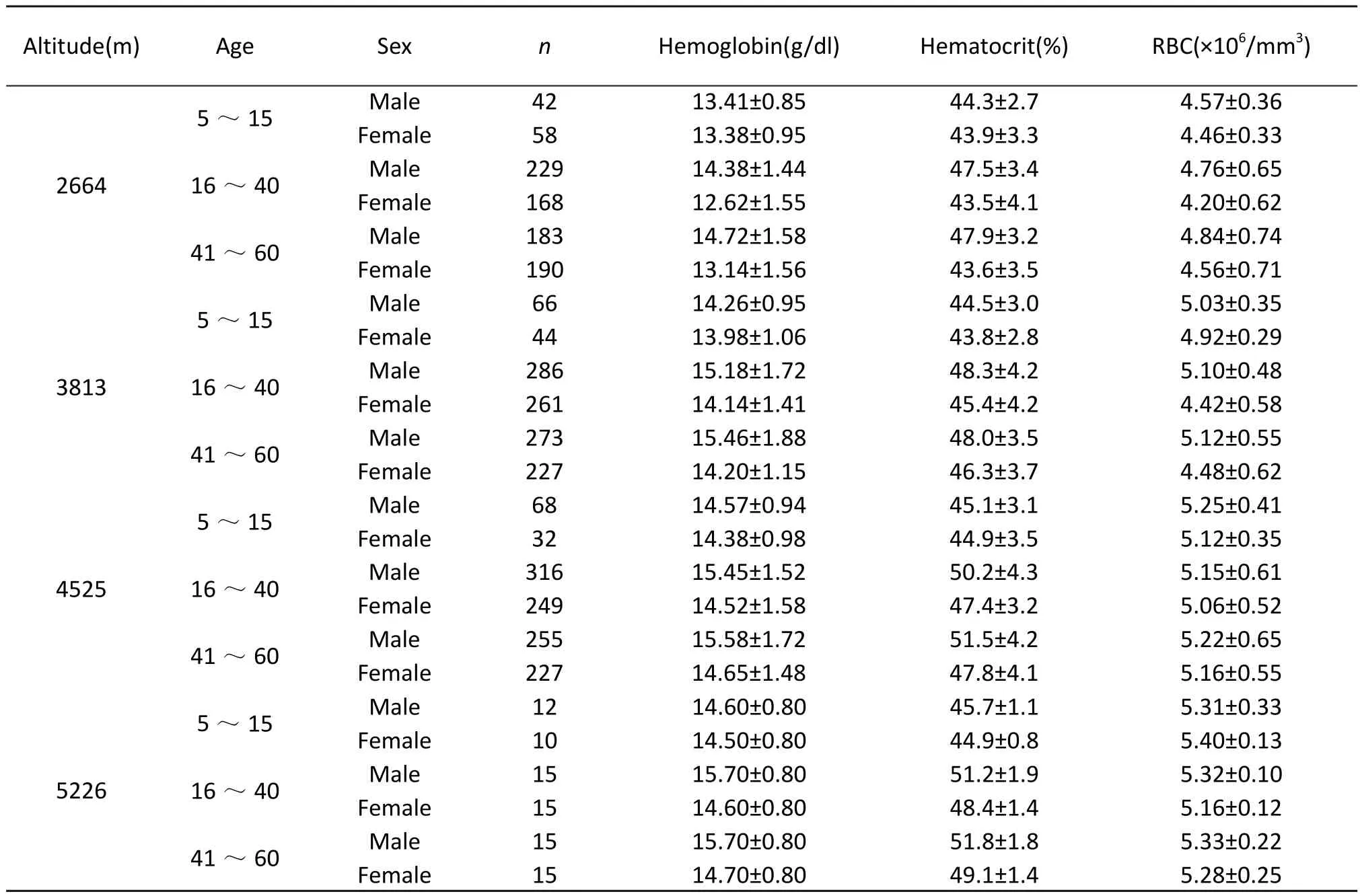
Tab. 2 Hematological parameters in Tibetan children and adults in Qinghai-Tibet at four different altitudes.
Hemoglobin diあerences: older minus younger (eあect of age)
In the present data, the most striking finding relative to age, was the hemoglobin difference between young men and boys (Fig.3). For Tibetans, panel A, the finding was that young men had about one gm/dl more of hemoglobin than did boys for all the altitudes examined, but older men had hemoglobin values little higher than those in young men. For females, while young women may have had more hemoglobin than girls, and older women may have had more hemoglobin than younger women, the age related difference was clearly less than the one gm/dL seen between young men and boys. For Tibetans,therefore and relative to the other age comparisons,the higher hemoglobin in young men than in boys stood out.
For Han males, panel B, the finding was that young men had about three g/dl of hemoglobin more than did boys for all the altitudes examined, but older men had hemoglobin values relatively similar to younger men. For females, while young women may have had more hemoglobin than girls, and older women may have had more hemoglobin than younger women,the age related difference was clearly less than the three gm/dl seen between young men and boys. For Han therefore, and relative to the other age comparisons, the higher hemoglobin in young men than in boys was striking.
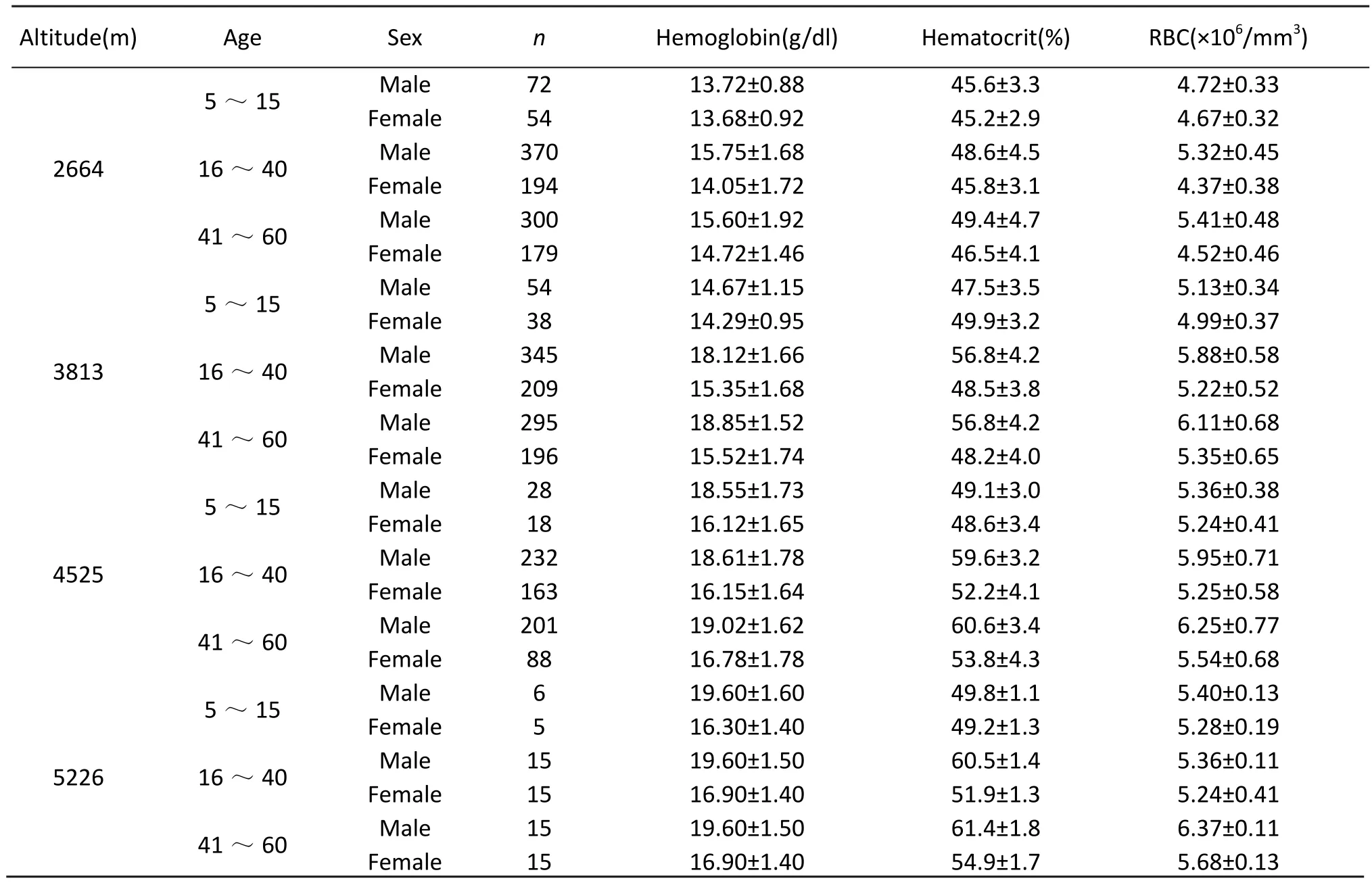
Tab. 3 Hematological parameters in Han children and adults in Qinghai-Tibet at four different altitudes.
On viewing panels A and B, we observed that the higher hemoglobin in young men than in boys was a more striking difference in Han than in Tibetans.Also apparent was that the hemoglobin comparisons for the other Han and Tibetan groups (older versus younger men, young women versus girls, older women versus younger women) did not show diあerences as large as those between young men and boys.
Menopause and hemoglobin levels
A total of 784 Tibetan premenopausal and 275 postmenopausal women living at three diあerent altitudes(2 664 m, 3 813 m, and 4 520 m), 576 Han pre-menopausal and 236 postmenopausal women residing at the same altitudes were studied. そe premenopausal women were selected randomly both in Tibetans and Han. Table 4 presents a comparison of the mean Hb concentration in native Tibetan with acclimatized Han females pre- and post-menopause. Among the Tibetan females, the change little following the menopause at an altitude of 2 664 m. そe menopausal females had slightly but no significantly higher Hb concentration at 3 813 m. However, a dramatic increased Hb concentration were observed in Han menopausal females at 4 525 m with a highly significant diあerence between females before and afer menopause (P<0.01). Even so, after menopause the Tibetan female’s Hb concentration still to be lower than that of males. Among the Han females, the Hb concentration increased significantly in menopausal women at all three altitudes, the diあerence was more pronounced in pre-and in post-menopause (P<0.01 at 2 664 m and 3 813 m,P<0.001 at 4 525 m ). In addition, the mean age for the menopause shift to an earlier date among Han females at high altitude when compared with that in Han female lowlanders,while the mean age for the menopause. そe values of arterial oxygen saturation (SaO2) in Tibetan pre- and afer menopausal women was higher than that of the Han pre- and afer menopausal women at three different altitudes (Tab. 5).
The MVC, MCH, and MCHC were completely consistent with the data from China at sea level [20,21]. Moreover, direct microscopic examination of the red cell morphology and evaluation of the red cell indices revealed the cells to be normocytic and normochromatic, with no evidence of a nutritional anemia. Although the values of Hb in Tibetans was significantly lower than Han migrants, the red cell indices were not diあerent.
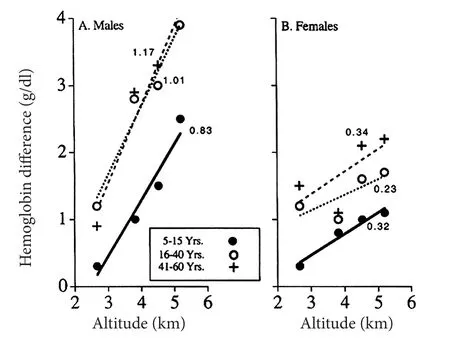
Fig. 1 Hemoglobin difference Han minus Tibetan (effect of ethnic group) versus altitude of residence for three different age groups. Shown are 5- 15 years (filled circles, unbroken line), 16 - 40 years (unfilled circles, dotted line) and 41 -60 years (pluses, dashed line). The slopes of the lines are indicated. Shown are males (panel A) and females (panel B).Here and in Figures 2 and 3, data are from Table1 and 2.
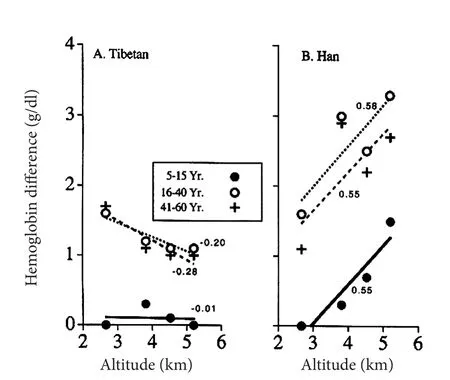
Fig. 2 Hemoglobin difference male minus female (effect of gender) versus altitude of residence for the three age groups.Symbols are the same as in Figure 1. The slopes of the lines are indicated. Shown are Tibetans (panel A) and Han (panel B).
Discussion
The main findings of the present investigation were that among persons living on the Qinghai-Tibetan Plateau, hemoglobin concentrations at various altitudes were different between Han and Tibetan residents depending on gender and age. The study aimed at a description of normal subjects by eliminating persons with disease, and those with histories of smoking, dust exposure, or substance abuse.However, even with a cohort of nearly seven thousand normal subjects, the present study had certain limitations. One was the lack of sea level measurements, which resulted from our inability to evaluate concurrently a substantial cohort of Tibetan subjects born and raised at sea level. Another limitation of the present study was that it could not distinguish ethnic from developmental differences, because Tibetans were born and remained at altitude, while Han were born near sea level and migrated to high altitude.そus for Han, and in contrast to Tibetans, the duration of altitude residence was less than the reported age. However, despite these problems, the present study represented the largest, most systematic and complete, collection and analysis of altitude-related hematological data performed to date on the Tibetan Plateau.
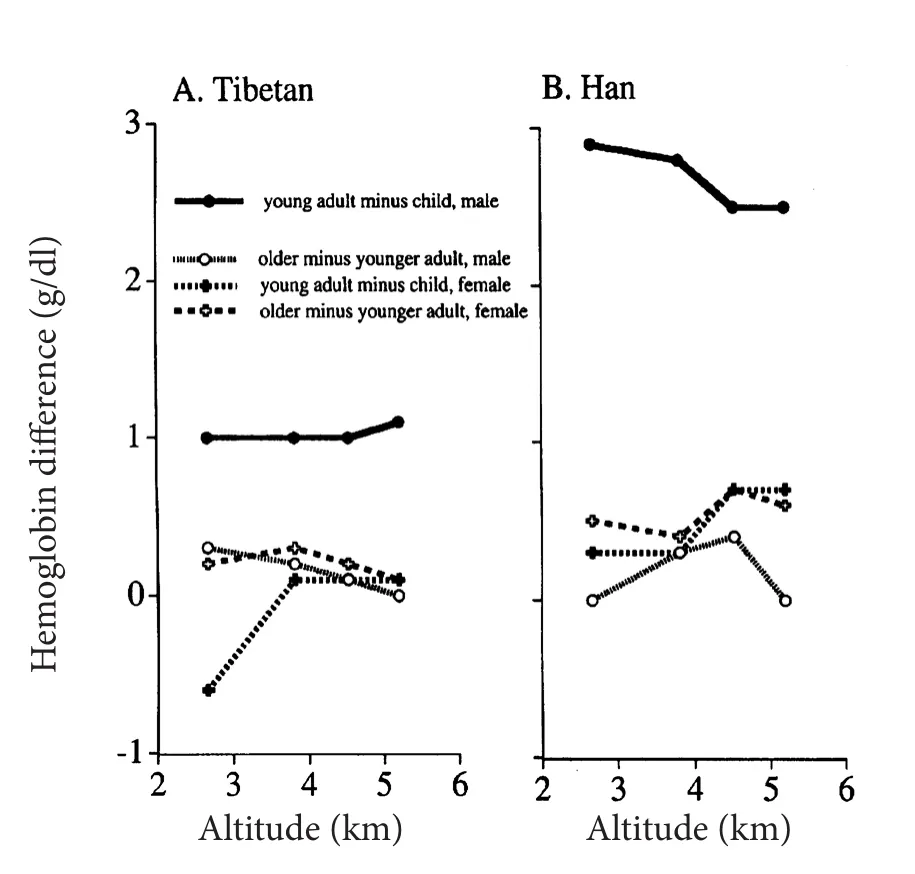
Fig. 3 Hemoglobin difference older minus younger subjects(effect of age) versus altitude for a comparison of young men and boys (filled circles and unbroken line), older and younger men (unfilled circles and dotted lines), young women and girls (filled pluses and dashed lines), and older women and younger women (unfilled pluses and dashed lines). Shown are Tibetans (panel A) and Han (panel B).
A comparison of our data with previously published data from the Tibetan plateau (Fig.4) previously published data in adult Tibetan men show a wide range of hemoglobin concentrations for a given altitude. While we do not know the cause of the variability, or why our data are at the lower end ofthe published range, we have wondered if our exclusion of smokers may have contributed to the findings in our study. If so, comparison of hemoglobin levels in smoking and non-smoking Tibetan men is important in future studies in high altitude residents. In any event, our findings do emphasize diあerences between Tibetan and Han subjects living in the same location and who, by our criteria and by interviews, were consuming their usual diets and in good health.

Tab. 4 The values of Hb concentration (g/dl) difference between the pre-menopausal and post-menopausal women in Tibetan natives and Han sojourners.

Tab. 5 The values of arterial oxygen saturation (SaO2, %) difference between the pre-menopausal and post-menopausal women in Tibetan natives and Han sojourners.
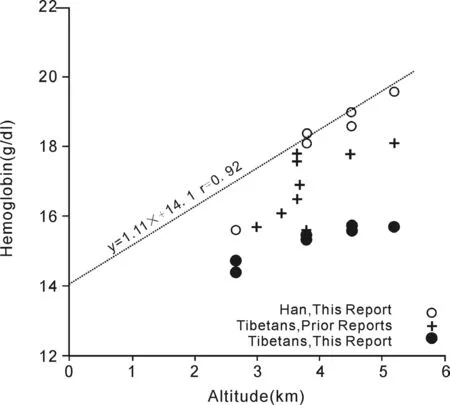
Fig. 4 Hemoglobin values at varying altitudes in normal adult, male populations residing at high altitude. The dotted line with its equation represents the line of best fit through mean values reported in the literature from North and South America and for Han subjects in Tibet (references from our recent review[10]). Unfilled circles indicate measurements in Han men from this report. Filed circles indicate Tibetan men from this report.
In the present study, the higher hemoglobin levels occurred in Han than Tibetan subjects at altitude was supported by a) the larger altitude coeきcients in the Han subjects as calculated by multiple regression, b)the displacement in Han of the mode toward higher hemoglobin values in the histograms of male and female populations at 4 525 m, c) the positive Han-Tibetan hemoglobin difference for given classes of altitude and age, especially in males, d) the increase in the Han - Tibetan hemoglobin diあerence with increasing altitude, especially in males, and e) the previous findings reported in the literature, as recently reviewed [10,16]. The greater increase in the hemoglobin with increasing altitude in Han than in Tibetan suggests that the two ethnic groups responded diあerently to progressively severe chronic hypoxia.
In the present study, the Hb, Hct, and RBC are higher in men than women for both Tibetan and Han residents. However, the diあerence between men and women is less for Tibetan than for Han. Also, the difference is particularly striking among the males,Han males appeared to have much higher Hb values than the male Tibetans. An interesting phenomenon is the line relating Hb to altitude for Han men presented a much higher prevalence of CMS than Tibetan men in Tibet (1.78%vs5.59%,P<0.001)[6].
Aging and high altitude polycythemia is an intriguing question that arise for discussion. Peruvian scientists suggested that CMS is an accentuated tendency to polycythemia that occurs normally with age [17]. そe age-dependent polycythemia is caused by an age-dependent loss of ventilation and arterial hypoxemia [18, 19]. Does there is also a similar relation between Hb/Hct and the age of Tibetan populations at diあerent altitudes? Unfortunately, too little research has been done in this area in the Himalayas.These tantalizing data have noted the fact that Han Chinese at sea level their hematological parameters,Hb, Hct, and RBC increased progressively from 1-18 years of age and remains unchanged through old age[14,15]. Nevertheless, while they had been migrated to and lived permanently at high altitude, there was a positive correlation between Hb/Hct and age in the Han immigrants at three altitudes. Among the Tibetans, however, there was little or no tendency of these hematological parameters to increase with age. Inversely, Tibetans show the similar pattern of change in hematological parameters with age as seen at lowlands. そis is an evidence that Tibetan and Andean high-altitude natives have adapted differently [20],and these reveal generally more genetic variance in the Tibetan population and more potential for natural selection [21].
Relatively, studies in the Andes suggest that women who protected from CMS during their pre-menopausal span, but after menopause the increase in hemoglobin with a high incidence of CMS, and has been attributed to the post-menopausal decrease in levels of ovarian hormones [7-9]. How is the situation among Tibetan females? Present study showed that among the Han females, the postmenopausal women have a higher Hb concentrations than those of the pre-menopausal women with a high significant difference (P<0.01) for the all three altitudes. The diあerence was more pronounced even at altitude of 2 664 m. そis finding was confirmed by Santolaya et al (1982) [22] who found that in 162 Andean older females (aged 40-50 yr) living at 2 800 m, PaCO2was also increased above male in this age range. Suggest even at lower altitude, females after menopause the decreased progesterone levels induced hypoventilation which accentuate hypoxemia and lead to an increased erythropoiesis. Surprisingly, in Tibetans an age-related increase in Hb concentration occurred in older postmenopausal women was seen only in higher residents than 4 000 m above sea level, and had statistical significant, indicates that the threshold altitude for erythrocytosis is much higher for Tibetan women than for Han women. そis diあerence is due in part to the Tibetan older women seem to ventilate more than Han, although the mechanism is unclear. Our own data from Maqin area (4 520 m ) suggest that menopausal Tibetan women have higher resting minute ventilation per unit of body surface area (VE 8.2±0.4 vs 7.4±0.6 L·minˉ1·m2 SE,P<0.001 ) and higher saturation (88.30% ±0.05%vs 84.20%±0.06% SE, P<0.01) when compared to menopausal Han women [23]. Leon-Velarde et al reported that in 152 women, 30-54 years old, living at 4 300 m, oxygen saturation fell 3% and hematocrit rose 3% afer menopause. A threshold CMS score of 21 was exceeded by 45% after menopause but only 22% before [7]. Our study showed that menopausal Tibetan women have a higher SaO2values than Han women after menopause at three different altitudes of 2 264 m, 3 814 m, and 4 524 m. Possibly Tibetan women have greater hypoxic ventilatiory responsiveness, larger lungs, better lung function, and greater lung diffusing capacity than lowland Han migrants,thus had less hypoxemia or a smaller hematopoietic response to a given level of hypoxemia than Han women [24]. Results from this study could further validate the hypothesis that Tibetans are genetically adapted to high altitude [10,11].
Finally, what is the significance of an increased Hb in terms of high altitude adaptation? It is still a controversial issue. Some authors suggested that polycythemia is a compensatory mechanism for hypoxemia at high altitude and therefore that high levels of Hb represent a physiologic response and may be beneficial [25], at least people who living at moderate altitude that’s how it is [8]. However, others believe that such a polycythemic response is pathological rather than adaptational [26], and on the basis of hemodilution studies, that even mild erythrocytosis may serve no useful physiological purpose [27]. In this regard, a very brilliant exposition was oあered by Winslow [28]that polycythemia is a two-edged sword: increase hemoglobin concentration is potentially important in augmenting oxygen-carrying capacity, but Hct values over 50%-55% dramatically increased blood viscosity and may impose a circulatory burden. Clearly, altitude polycythemia is a liability but not an asset.
Acknowledgements
そis work was supported by the “973” National Basic Research Program (2012 CB 518202, and “Pre-973”National Basic Research Program (2012 CB 722506),PRC We thanks to Prof. Ye Cheng-Fu of the Department of mathematics of the Qinghai General University for multivariate regression analysis of this study.
1. Wu TY, Wang XQ, Wei CY, et al. Hemoglobin levels in Qinghai-Tibet: different effects for Tibetans versus Han[J]. J Appl Physiol, 2005, 98(2): 598-604.
2. Winslow RM, Chapman KW, Gibson CC, et al. Different hematologic responses to hypoxia in Sherpas and Quechua Indians [J]. J Appl Physol, 1989, 66(4): 1561-1569.
3. Winslow RM, Chapman KW, and Monge CC. Ventilation and the control of erythropoiesis in high altitude natives of Chile and Nepal[J]. Am J Human Biol, 1990, 2(6): 653-662.
4. Monge CC, Arregui A, Leon-Velarde F. Pathophysiology and epidemiology of chronic mountain sickness [J]. Int J Sports Med, 1992, 13(Suppl 1): S79-S81.
5. Leon-Velarde F, Arregui A, Monge C, et al. Ageing at high altitude and the risk of chronic mountain sickness [J]. J Wild Med, 1993, 4(2): 183-188.
6. Wu TY, Li Y, Ge RL, et al. Epidemiology of chronic mountain sickness: Ten years’ study in Qinghai-Tibet [M]//Ohno H, Kobayashi T, Masuyama S, et al. Progress in mountain medicine and high altitude physiology. Matsumoto: Press Committee of the そird World Congress, 1998: 120-125.
7. Leon-Velarde F, Ramos MA, Hernandez J-A, et al. そe role of menopause in the development of chronic mountain sickness [J]. Am J Physiol Regul Integr Comp Physiol, 1997,272 (1Pt 2): R 90-R94.
8. Leon-Velarde F, Gamboa A, Chuquiza JA, et al. Hematological parameters in high altitude residents living at 4 355, 4 660, and 5 500 meters above sea level [J]. High Alt Med Biol, 2000, 1(2): 97-104.
9. Leon-Velarde F, Rivera-Chira M, Tapia R, et al. Relationship of ovarian hormones to hypoxemia in women residing at 4 300 m [J]. Am J Physiol Regul Interg Comp Physiol, 2001, 280(2): R 488-R493.
10. Wu TY, Liu FY, Ouzhou-Loubu, et al. A genetic adaptive pattern-low hemoglobin concentration in the Himalayan highlanders[J]. Chin J Appl Physiol, 2013, 29(6): 481-493.
11. Wu TY. High-altitude medical research in China: importance and relevance [J]. Science, 2012 (Suppl): 3.
12. Monge CC. Natural acclimatization to high altitude: clinical conditions [M]// Life at High Altitude. Washington, PAO,Scientific Publication. No 140. 1966: 46.
13. Leon-Velarde F, Maggiorini M, Reeves JT, et al. Consensus statement on chronic and subacute high altitude Disease [J].High Alt Med Biol, 2005, 6(2): 147-157.
14. Tianjing hematological investigative group (THIG). A survey of the hematological parameters in 1677 healthy persons living in the Tianjing region [J]. J Tianjing Med, 1980,8(Suppl. Transfusion and blood ): 158-162.
15. Deng JD. Clinical hematology[M]. Shanghai: Shanghai Science and Technology Press, 1985: 1018-1050.
16. Moore L.G. Human genetic adaptation to high altitude[J].High Alt Med Biol, 2001, 2(2): 257-282.
17. Whittembury J, Monge CC. High altitude, hematocrit, and age [J]. Nature (London), 1972, 238(5362): 278-279.
18. Sime F, Monge CC, Whittembury J. Age as a cause of chronic mountain sickness (Monge’s disease)[J]. Int J Biometeorology, 1975, 19 (2): 93-98.
19. Monge CC, Whittembury J. Chronic mountain sickness and the physiopathology of hypoxemic polycythemia [M]//Sutton JR, Jones NL, Houston CS. Hypoxia: man at altitude.New York: そieme and Stratton, 1982: 51-56.
20. Beall CM. Two routes to functional adaptation: Tibetan and Andean high-altitude natives [J]. Proc Natl Acad Sci USA,2007, 104(Suppl 1): 8655-8660.
21. Beall CM. Tibetan and Andean pattern of adaptation to high altitude Hypoxia [J[. Human Biol, 2000, 72(2): 201-228.
22. Santolaya BR, Araya CJ, Vecchiola DA., et al. Hematocrito,hemoglobina y pression de oxigeno arterial en 270 hombres y 266 mujeres sanas residentes de altura (2 800 ms) [J]. Rev Hosp Roy H Glover, 1981, 1(1): 17-29.
23. Wu TY, Li WS, Wei CY, et al. Chronic mountain sickness:Gender differences and the influence of menopause [J].Chin J Appl Physiol, 2000, 16(Suppl 1): 5-6.
24. Wu TY, Kayser B. High altitude adaptation in Tibetans[J].High Alt Med Biol, 2006, 7(3): 193-206.
25. Zubieta-Castillo G, Zubieta-calleja G, Arano E, et al. Respiratory disease, chronic mountain sickness and gender differences at high altitude [M]// Ohno H, Kobayashi T,Masuyama S, et al. Progress in mountain medicine and high altitude physiology. Matsumoto: Press Committee of theそird World Congress, 1998: 132-137.
26. Garruto RM, Dutt JS. Lack of prominent compensatory polycythemia in traditional native Andeans living at 4 200 meters [J]. Am J Phys Anthropol, 1983, 61(3): 355-366.
27. Winslow RM Monge CC, Brown RG, et al. Eあects of hemodilution on O2transport in high-altitude polycythemia [J]. J Appl Physiol, 1985, 59(5): 1495-1502.
28. Winslow RM. High-altitude polycythemia [M]// West JB,Lahiri S. High altitude and man. Bethesda: Amer Physiol Society Press, 1984: 163-172.
- 中國應用生理學雜志的其它文章
- Children’s exercise capacity at high altitude in Tibet
- Hypoxic preconditioning: effect, mechanism and clinical implication (Part I)
- Role of HCN channels in the nervous system: membrane excitability and various modulations
- How to deal with cerebral palsy in 21st century
--A new epoch in clinic treatment - A rat model of high altitude polycythemia rapidly established by hypobaric hypoxia exposure
- Plasma endothelin-1 and nitric oxide correlate withligustrazine alleviation of pulmonary artery hypertension in patients of chronic cor pulmonale from high altitude plateau during acute exacerbation