
Atypical Chronic Myeloid Leukaemia with Trisomy 13:a Case Report
2011-11-22 02:36:10GuoyuHuChaohuiYuanKuiTanandZhenzhenChen
Chinese Medical Sciences Journal 2011年4期
Guo-yu Hu*,Chao-hui Yuan,Kui Tan,and Zhen-zhen Chen
Department of Hematology,First Hospital of Zhuzhou,Zhuzhou 412000,China
ATYPICAL chronic myeloid leukaemia (aCML),which shows both myeloproliferative and myelodysplastic features,is a type of myeloproliferative/myelodysplastic disease as defined by the World Health Organisation (WHO) classification of the myeloid neoplasms.1Because of the presence of neutrophilic leukocytosis,aCML may resemble chronic myelogenous leukemia (CML).However,in contrast with CML,aCML does not have the Philadelphia chromosome or the bcr/abl fusion gene.
With the continuous karyotype analysis of aCML,several changes in the karyotype of aCML have been detected.However,few are recurring and no specific cytogenetic changes have been associated with aCML.Nonspecific cytogenetic abnormalities can be observed in 56%~82% of aCML cases.Although the most frequent abnormalities include trisomy 8 and del (20q),abnormalities involving other chromosomes such as 12,13,14,17,and 19 have also been described.1In this report we describe a case of aCML with trisomy 13.
CASE DESCRIPTION
A 36-year-old female was admitted into the hospital in August,2010 for lymphadenectasis in the left neck accompanied with low-grade fever for one month.In physical examination,the main finding was two palpable enlarged lymph nodes in the left neck with the size of 2 cm×1.5 cm,medium degree of hardness,and gentle tenderness.Liver and spleen were not touched in subcostal region.Blood routine examination revealed white blood cell (WBC) count at 16.8×109/L,neutrophils 0.81,hemoglobin 118 g/L,and platelets 422×109/L.Biopsy report of one of the swollen lymph nodes revealed lymphoid tuberculosis.X-ray test of the chest showed no abnormalities.Tuberculosis antibody test showed positive IgG,and negative result in purified protein derivative test.
The patient was given anti-tuberculosis treatment combined with rimifon 0.3 g once per day,rifampicin 0.45 g once per day,pyrazinamide 0.75 g once per day,and ethambutol 0.5 g thrice per day.Changes in blood routine examination were detected during the course of treatment,showing a progressive increase of WBC to 38×109/L after two months.After treated with interferon α2b (5×106units by intramascular injection every other day),WBC was progressively increased,anaemia as well as thrombocytopenia occurred.
In order to determine the reason of leukocytosis,the patient was admitted into hospital again.Physical examination revealed lymphadenectasis all over the surface of her body.In addition,spleen was palpated 4.5 cm apart from the left ribs,and liver about 3 cm below the right ribs.Biopsy of lymph node of the neck was performed once again to rule out the spread of scrofula,the result of which showed massive inflammatory cell infiltration in the lymph node,suggesting reactive hyperplasia.The value of alkaline phosphatase was 71.Full blood count revealed neutrophilic leukocytosis (WBC,82.43×109/L;neutrophils,48.53×109/L).Hemoglobin was 62 g/L,and platelet count was 49×109/L.In addition,the blood film showed a left shift,with the presence of 4% myeloblast,2% myelocytes,4% stab cells but none nucleated red cells.Bone marrow aspirate smear showed hypercellularity with prominent granulocyte proliferation and marked dysgranulopoiesis.Two hundred karyocytes were classified,in which granulocyte series accounted for 64.5% and erythron accounted for 31%.In the granulocyte series,myeloblasts took up of 4%,progranulocytes 1%,myelocytes 19.5%,metagranulocytes 12%,stab cells 12.5%,and segmented neutrocyte 15%.Bone marrow biopsy revealed hypercellularity dominated by granulocyte series,and no abnormal localization of immature precursors was found.Bcr/abl fusion gene and JAK2V617F mutation detection using specific allele PCR test produced negative results.No -5/5q-,-7/7q-,21-or other chromosome disorders common in myelodysplastic syndrome was detected with fluorescence in situ hybridization (FISH).Cytogenetic analysis of bone marrow with routine G-band coloration detected trisomy 13.Bacterial artificial chromosome clone RP11-115I22 (chr 13:47 901 161~ 48 065 782) (Invitrogen,Carlsbad,CA,USA) located in the RB gene region of chromosome 13 was chosen as the probe for chromosome 13 counting,and trisomy 13 was confirmed using FISH (Fig.1).
A diagnosis of aCML was made based on the above findings.In addition to concentrated RBC transfusion,the patient was treated with hydroxyurea (3 g once per day for 5 days,1.5 g once per day for 7 days,1.0 g once per day for 4 days) and thalidomide (150 mg once per day for 16 days).Re-examination of full blood count after treatment revealed that WBC count was 12.43×109/L,neutrophils 75.5%,haemoglobin 117 g/L,platelet count 27 ×109/L.After being discharged from the hospital,the patient still took thalidomide 150 mg once per day and hydroxyurea 0.5 g once per day for 3 months up to the present with regular follow-up.
DISCUSSION
aCML is a rare myeloid neoplasm (approximately 1-2 cases per 100 cases of typical bcr/abl+CML) that primarily affects the elderly (median age,62-68 years),shows no distinct gender difference,and often presents with extramedullary disease,mostly involving the spleen and the liver.2Cytogenetic abnormalities occur commonly in aCML;however,no specific cytogenetic changes have been associated with aCML.3To the best of our knowledge,there has been no report about aCML with karyotype of sole trisomy 13.In the present case,the patient demonstrates the following clinical features:firstly,young age of onset;secondly,fast changing peripheral blood cell count;thirdly,lymphadenectasis over the surface of the body and splenohepatomegalia;fourthly,as shown in bone marrow cytomorphologic examination,normal value of neutrohpil alkaline phosphatase,eosinophilic granulocyte and basophilic leukocyte were not increased;and last,no response to interferon treatment.
Trisomy 13,as a sole karyotypic abnormality in acute leukemia,has been reported in several cases.4-6In addition,few CML cases with trisomy 13 as the sole cytogenetic abnormality have been reported so far.7Trisomy 13 was reported to be one of the factors of unfavorable prognosis and poor therapeutic reaction in AML.8The role of the additional copy of chromosome 13 in the molecular pathogenesis of aCML is not clear and the gene(s) of importance in chromosome 13 are yet to be determined.Recently,Fehniger et al4have reported that the symptoms of 3 casesof AML caused by trisomy 13 were relieved by lenalidomide treatment,so we adopted the combination of hydroxyurea and thalidomide to treat this patient,with satisfactory therapeutic effect.Nonetheless,more clinical cases are needed to identify the clinical features and effective treatment of aCML with trisomy 13.
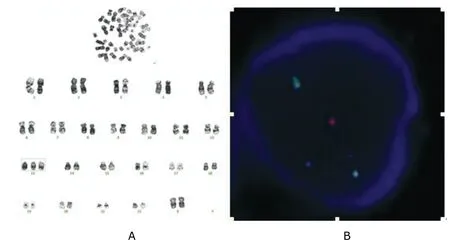
Figure 1.Trisomy 13 in a 36-year-old female patient.
1.Hall J,Foucar K.Diagnosing myelodysplastic/myeloproliferative neoplasms:laboratory testing strategies to exclude other disorders.Int J Lab Hematol 2010;32:559-71.
2.Xubo G,Xingguo L,Xianguo W,et al.The role of peripheral blood,bone marrow aspirate and especially bone marrow trephine biopsy in distinguishing atypical chronic myeloid leukemia from chronic granulocytic leukemia and chronic myelomonocytic leukemia.Eur J Haematol 2009;83:292-301.
3.Hernández JM,del Ca?izo MC,Cuneo A,et al.Clinical,hematological and cytogenetic characteristics of atypical chronic myeloid leukemia.Ann Oncol 2000;11:441-4.
4.Fehniger TA,Byrd JC,Marcucci G,et al.Single-agent lenalidomide induces complete remission of acute myeloid leukemia in patients with isolated trisomy 13.Blood 2009;113:1002-5.
5.Baer MR,Bloomfield CD.Trisomy 13 in acute leukemia.Leuk Lymphoma 1992;7:1-6.
6.Trivedi PJ,Patel PS,Brahmbhatt MM,et al.A new recurring chromosome 13 abnormality in two older patients with de novo acute myeloid leukemia:an Indian experience.Indian J Hum Genet 2009;15:137-9.
7.Saigo K,Nakagawa T,Ryo R,et al.Philadelphia chromosome-negative chronic myelogenous leukemia with trisomy 13.Rinsho Ketsueki 1995;36:1295-9.
8.Ito Y,Hakoda Y,Iwase O,et al.First Japanese case of sole trisomy 13 anomaly in acute myeloid leukemia.Cancer Genet Cytogenet 2000;120:85-6.
 Chinese Medical Sciences Journal2011年4期
Chinese Medical Sciences Journal2011年4期
- Chinese Medical Sciences Journal的其它文章
- Efficacy of Surgical Therapy for Carotid Body Tumors
- Neurological Manifestations of Takayasu Arteritis
- Efficacy and Safety of Low Molecular Weight Heparin Prophylaxis for Venous Thromboembolism Following Lumbar Decompression Surgery
- Contrary Regulation of TIMP-1 and MMP-9 by Hepatocyte Growth Factor Antibody after Lung Injury
- Surgical Removal of a Giant Vegetation on Permanent Endocavitary Pacemaker Wire and Lead
- Open Partial Nephrectomy in Solitary Kidney with Multiple Renal Cell Carcinoma:a Case Report