
Conversion immunotherapy for deficient mismatch repair locally unresectable colon cancer: A case report
2023-12-29 03:18:54ZhenSunHeLiuGuanNanZhangYiXiao
Zhen Sun,He Liu,Guan-Nan Zhang,Yi Xiao
Abstract BACKGROUND Owing to the special features of biologics,deficient mismatch repair (dMMR) in patients with colon cancer has achieved little treatment efficacy from chemoradiotherapy.Immunotherapy has shown promising results for the treatment of colon cancer.The high response rate observed suggests a great option for patients presenting with unresectable tumors,as it allows for better oncological resection.Here,we aimed to highlight the significant effects of immunotherapy on dMMR in colon cancer.CASE SUMMARY A 54-year-old man diagnosed with locally unresectable dMMR colon cancer received preoperative immunotherapy (three cycles of pembrolizumab) and achieved a pathological complete response after surgery.CONCLUSION Immunotherapy can be used as a conversion treatment for locally unresectable colon cancer with dMMR.
Key Words: Colon cancer;Immunotherapy;Pathological complete response;Case report
INTRODUCTION
Surgery remains the primary radical therapy for colon cancer[1,2],and resection radicality is an important predictor of local recurrence and overall survival[3].Owing to the delayed administration of adjuvant chemotherapy,postoperative complications can cause poor oncological outcomes in patients with colorectal cancer (CRC)[4].Hence,resection radicality should be improved,and the incidence of surgical complications should be reduced.Preoperative chemotherapy improves resection radicality and survival[5-8].However,owing to the special features of biologics,patients with deficient mismatch repair (dMMR) colon cancer have achieved little treatment efficacy with chemoradiotherapy[9].Immunotherapy has previously shown promising results for colon cancer[10-13].Hence,we aimed to draw attention to its significant effect on dMMR in colon cancer.This study was written in compliance with the SCARE Guideline[14].
CASE PRESENTATION
Chief complaints
A 54-year-old man presented to the hospital with difficulty in defecating.
History of present illness
Symptoms started 2 mo before the patient was diagnosed with colon cancer in May 2023.
History of past illness
The patient had undergone colectomy twice owing to a poorly-differentiated adenocarcinoma of the splenic flexure colon (unknown pTNM stage) in 2007 and a moderate-to poorly-differentiated adenocarcinoma of the cecum (pT4aN2a) in 2008.Postoperative adjuvant chemotherapy was administered after both surgeries.
Personal and family history
The patient denied any family history of malignant tumors.
Physical examination
Physical examination revealed normal vital signs.The digital anal examination result was also normal.
Laboratory examinations
Laboratory results showed normal carcinoembryonic antigen and carbohydrate antigen 19-9.No abnormality was found in routine blood analyses.
Imaging examinations
Colonoscopy revealed a large,cauliflower-like mass in the transverse colon.Histopathological examination of the biopsy specimen revealed a poorly-differentiated adenocarcinoma with dMMR.Contrast-enhanced abdominal computed tomography (CT) demonstrated a bulky tumor measuring >10 cm in the transverse colon (Figure 1A),and several enlarged lymph nodes in the mesentery.CT did not reveal metastases to distant sites.
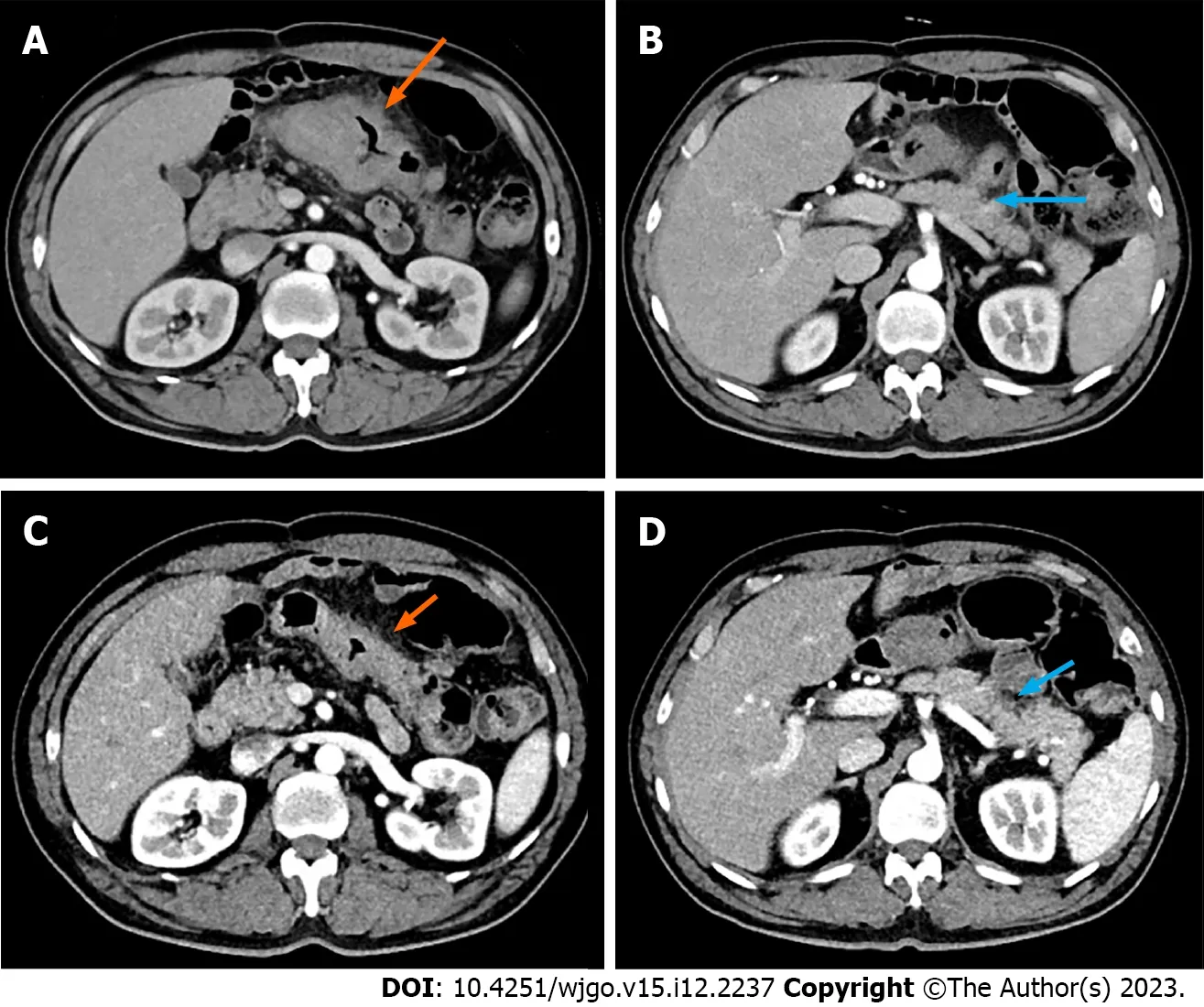
Figure 1 Computed tomography scans taken before and after immunotherapy. A and B: Before immunotherapy (arrows);C and D: After immunotherapy.The orange arrows showed the location and range of the tumor,while the blue arrows showed invasion of the pancreatic capsule.
FINAL DIAGNOSIS
Considering the invasion of the pancreatic capsule (Figure 1B),negative margins were not ascertained intraoperatively.
TREATMENT
Preoperative immunotherapy is recommended for conversion to resection.The patient received three cycles of pembrolizumab immunotherapy without complaints.Post-treatment CT showed significant regression of the tumor (Figure 1C and D),as assessed by our team.
Thus,the patient underwent open transverse colectomy with D2 lymph node dissection two weeks after the end of immunotherapy.The previous ileocolonic anastomosis was resected during surgery.
As shown in Figure 2A,gross examination revealed invasion of the serosal surface by the tumor.Interestingly,pathological examination showed that the tumor regression grade was 0,indicating complete regression with no residual tumor cells,including the lymph nodes (Figure 2B).The final stage in this patient was a pathologic complete response (pCR).
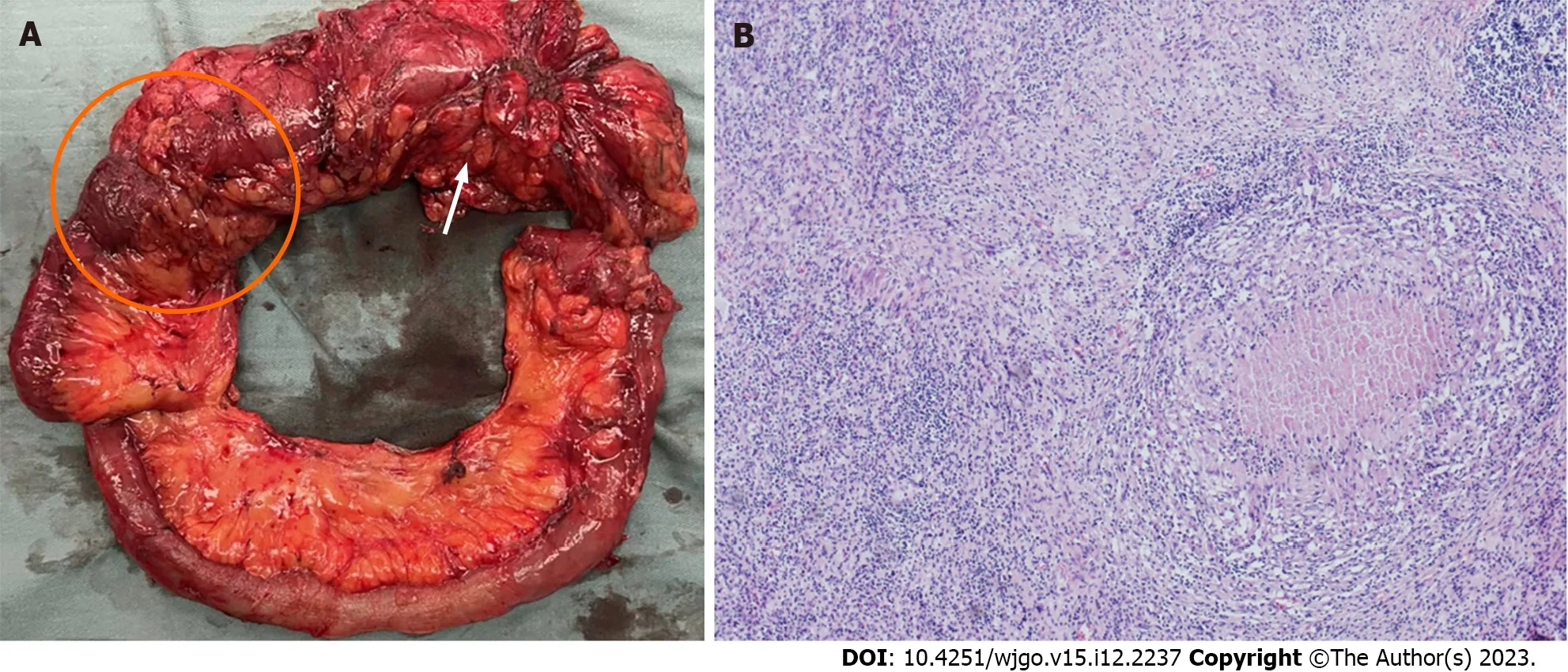
Figure 2 Gross pathological examination and hematoxylin and eosin staining. A: Gross pathological examination showed the tumor (orange arrow)and previous ileocolonic anastomosis (orange circle);B: Hematoxylin and eosin staining slide (magnification: × 40) showed that the lesion was tumor-free.
OUTCOME AND FOLLOW-UP
Delayed gastric emptying (DGE) occurred,and a transnasal feeding tube was placed for nutritional support.The patient was discharged from the hospital on the 39th day after surgery,when the DGE was alleviated.
DISCUSSION
To the best of our knowledge,this case is the first to provide evidence of the efficacy of immunotherapy as a conversion regimen for locally unresectable colon cancer with dMMR.
The hallmark of dMMR is the inability to repair spontaneous mutations during DNA replication,leading to hypermutation and increased tumor mutation burden[15].Currently,dMMR is one of the major predictive biomarkers of the benefits of immune checkpoint inhibitor (ICI) benefit[16].Thus,MMR status should be regularly tested for colon cancer to guide personalized treatment.ICI therapy aims to overcome tumor immune escape by targeting immune inhibitory molecules expressed on the surfaces of the tumor and immune cells.
Since numerous questions remain regarding dMMR and its impact on the efficacy of immunotherapy,several clinical trials have been launched to determine the optimal treatment for patients with colon cancer.NICHE-1 was the first neoadjuvant immunotherapy study to show pathological responses in 100% of dMMR tumors[10].The PICC trial[12] reported a pCR rate of 65% in patients with locally advanced dMMR CRC who received immunotherapy.Peiet al[17] reported that 90.9% of patients with locally advanced dMMR CRC achieved pCR after neoadjuvant immunotherapy.The NICHE-2 study subsequently reported that the rates of major pathological response and pCR for locally advanced dMMR colon cancer were 95% and 67%,respectively[11].It also reported the first survival data in which none of the patients had recurrence at a median follow-up of 13 mo,suggesting the advantage of neoadjuvant immunotherapy.More than the potential survival benefit of immunotherapy,Hanet al[18] reported that neoadjuvant immunotherapy significantly reduced open surgery (83.3%vs72.2%,P<0.001) and multi-visceral resection rate (P=0.025) for CRC patients.Hence,this therapy could minimize the extent of surgery and improve postoperative recovery.
The high response rate observed in patients suggests that surgery combined with neoadjuvant immunotherapy is a promising option for CRC surgeons to use in dMMR colon cancers which appear unresectable.This method is also likely to achieve better oncologic resection and organ-sparing strategies.However,the optimal duration of immunotherapy and the timing of surgery remain to be determined.Moreover,a long-term follow-up is required to assess the effects of immunotherapy on the survival of a selected subset of patients with dMMR colon cancer.
CONCLUSION
Immunotherapy can be used as a conversion treatment for locally unresectable dMMR colon cancer.However,further evidence from clinical trials is required to confirm these findings.
FOOTNOTES
Author contributions:Sun Z and Liu H collected data and drafted the manuscript;Zhang GN participated in data acquisition and interpretation;Xiao Y revised and finalized the manuscript;all authors have read and approved the final manuscript.
Supported byNational High Level Hospital Clinical Research Funding,No.2022-PUMCH-C-027.
Informed consent statement:Written informed consent was obtained from the patient for publication of this report and any accompanying images.
Conflict-of-interest statement:Written informed consent was obtained from the patient for publication of this report and any accompanying images.
CARE Checklist (2016) statement:The authors read the CARE Checklist (2016) and the manuscript was prepared and revised according to this checklist.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORCID number:Zhen Sun 0000-0001-7430-8081;Guan-Nan Zhang 0000-0001-8685-5015;Yi Xiao 0000-0002-4309-1227.
S-Editor:Yan JP
L-Editor:A
P-Editor:Yu HG
 World Journal of Gastrointestinal Oncology2023年12期
World Journal of Gastrointestinal Oncology2023年12期
- World Journal of Gastrointestinal Oncology的其它文章
- Dual primary gastric and colorectal cancer: A complex challenge in surgical oncology
- Association of MBOAT7 rs641738 polymorphism with hepatocellular carcinoma susceptibility: A systematic review and meta-analysis
- Prognostic value of T cell immunoglobulin and mucin-domain containing-3 expression in upper gastrointestinal tract tumors: A meta-analysis
- Intensive follow-up vs conventional follow-up for patients with nonmetastatic colorectal cancer treated with curative intent: A metaanalysis
- Paired-related homeobox 1 induces epithelial-mesenchymal transition in oesophageal squamous cancer
- Evaluating the causal relationship between human blood metabolites and gastroesophageal reflux disease