
Intensive follow-up vs conventional follow-up for patients with nonmetastatic colorectal cancer treated with curative intent: A metaanalysis
2023-12-29 03:18:50LiLiCuiShiQiCuiZhongQuZhenQingRen
Li-Li Cui,Shi-Qi Cui,Zhong Qu,Zhen-Qing Ren
Abstract BACKGROUND The frequency and content of follow-up strategies remain controversial for colorectal cancer (CRC),and scheduled follow-ups have limited value.AIM To compare intensive and conventional follow-up strategies for the prognosis of non-metastatic CRC treated with curative intent using a meta-analysis.METHODS PubMed,Embase,and the Cochrane Library databases were systematically searched for potentially eligible randomized controlled trials (RCTs) from inception until April 2023.The Cochrane risk of bias was used to assess the methodological quality of the included studies.The hazard ratio,relative risk,and 95% confidence interval were used to calculate survival and categorical data,and pooled analyses were performed using the random-effects model.Additional exploratory analyses were performed for sensitivity,subgroups,and publication bias.RESULTS Eighteen RCTs involving 8533 patients with CRC were selected for the final analysis.Intensive follow-up may be superior to conventional follow-up in improving overall survival,but this difference was not statistically significant.Moreover,intensive follow-up was associated with an increased incidence of salvage surgery compared to conventional follow-up.In addition,there was no significant difference in the risk of recurrence between intensive and conventional follow-up strategies,whereas intensive follow-up was associated with a reduced risk of interval recurrence compared to conventional follow-up.Finally,the effects of intensive and conventional follow-up strategies differed when stratified by tumor location and follow-up duration.CONCLUSION Intensive follow-up may have a beneficial effect on the overall survival of patients with non-metastatic CRC treated with curative intent.
Key Words: Intensive follow-up;Conventional follow-up;Colorectal cancer;Curative intent;Meta-analysis
INTRODUCTION
Colorectal cancer (CRC) is the third most frequently diagnosed cancer,which accounted for more than 1.9 million cases and 900000 cancer-related deaths worldwide in 2000,thereby causing a great public health burden[1,2].The incidence and prognosis of CRC have improved because of the use of population-based screening programs and understanding the necessity of a healthy lifestyle.Early diagnosis and treatment are significantly related to CRC prognosis[3].The 5-year survival rate is 90% for stage I-II CRC and is reduces to 14% for stage IV CRC[4].The standard treatment for early-stage CRC is curative surgery,and tumor node metastasis is an important predictor of early-stage CRC prognosis and other prognostic factors,including tumor location and clinicopathological results[5-7].Nevertheless,10%-20% of patients develop recurrent disease,and an additional follow-up strategy should be applied to improve CRC prognosis.
Curative surgery aims for the early detection of treatable recurrence and improving CRC prognosis.Generally,there is a long follow-up duration for patients with CRC treated through curative surgery.However,the frequency and content of follow-ups remain controversial for CRC,and scheduled follow-ups have limited value[8-10].A prior meta-analysis found that the use of intensive follow-up strategies could improve overall survival compared to conventional follow-up strategies.However,the pooled analyses did not yield a conclusive solution[11].Moreover,stratified analyses based on studies and patient characteristics were not performed.Therefore,this systematic review and meta-analysis was conducted to determine the effects of intensivevsconventional follow-up strategies on the prognosis of patients with CRC treated with curative intent.The study chose randomized controlled trials (RCTs) for its data.
MATERIALS AND METHODS
Search strategy and selection criteria
This study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines[12].RCTs comparing the effects of intensive and conventional follow-up strategies for non-metastatic CRC treated with curative intent were eligible for our study,and the publication language was restricted to English.We systematically searched PubMed,Embase,and the Cochrane library for eligible trials throughout April 2023,and we used the following search terms: (“colorectal neoplasms”) AND (“recurrence” OR “metastasis” OR “survival analysis” OR “mortality“ OR ”prognosis“) AND (“follow up“ OR “episode of care” OR “surveillance”) AND (“randomized controlled trials”).Trials that had already been completed but had not yet been published were also searched on the ClinicalTrials.gov website (NIH,United States).Manual searches were also performed on the reference lists of the relevant reviews to identify any new trials that met the inclusion criteria.
Two reviewers independently conducted the literature search and trial screening,and conflicts between the reviewers were resolvedviadiscussions.Studies were included if they met the following criteria: (1) Patients: All patients with nonmetastatic CRC who were treated with curative intent surgery;(2) Intervention: Intensive follow-up strategy;(3) Control: Conventional follow-up strategy;(4) Outcome: The study should report at least one outcome of overall survival,cancerspecific survival,relapse-free survival,salvage surgery,recurrence,and interval recurrences;and (5) Study design: All included studies had to have an RCT design.
Data collection and quality assessment
The following data were independently collected from the included trials: First author’s name,publication year,region,sample size,mean age,proportion of males,tumor stage (Dukes’ stage A/B/C),tumor location (colon cancer/rectal cancer),treatments (curative intent surgery and subsequent adjuvant treatments),intervention,control,follow-up,and reported outcomes (overall survival,cancer-specific survival,relapse-free survival,salvage surgery,recurrence,and interval recurrences).The Cochrane risk of bias was used to assess methodological quality,including random sequence generation,allocation concealment,blinding of participants and personnel,blinding of outcome assessment,incomplete outcome data,selective reporting,and other biases[13].Each item was defined as having a low,high,or an unclear risk of bias.Two reviewers independently performed the abstracted data and methodological quality assessments,and a third reviewer who referred to the original article settled inconsistent results.
Statistical analysis
The effects of intensivevsconventional follow-up strategies on survival and categorical data were assigned as hazard ratios (HR),relative risks (RR),and 95% confidence intervals (CI),and pooled analyses were performed using the random-effects model because it considers the underlying variations across the included trials[14,15].Heterogeneity among the included trials was evaluated usingI2andQstatistics,and significant heterogeneity was defined asI2>50% orP<0.10[16,17].The stability of the pooled analyses were determined using sensitivity analysis through the sequential removal of a single trial[18].Subgroup analyses of the investigated outcomes were performed based on sample size,mean age,proportion of males,tumor location,and follow-up duration,and the differences between subgroups were assessed using the interactiont-test,which assumes that the data distribution was normal[19].Moreover,the ratio of HR (RHR) to RR (RRR) between the subgroups was assessed among patients without specific characteristics[20].Funnel plots,Egger’s test,and Begg’s test were used to assess potential publication bias[21,22].All reportedPvalues for the pooled analyses were 2-sided,and the inspection level was 0.05.Statistical analyses were performed using the STATA software (version 10.0;Stata Corporation,College Station,TX,United States).
RESULTS
Literature search and study selection
A total of 2671 articles were identified from the initial electronic search,and 1743 studies were retained after duplicate articles were removed.Subsequently,1698 studies were excluded because they reported irrelevant topics,and the remaining 45 studies were retrieved for full-text evaluation.Reviewing the reference lists yielded two potentially eligible studies,and 46 articles were subjected to detailed evaluation.After this,28 studies were excluded because they reported the same population (n=15),did not have an RCT design (n=9),or included cancers at other stages (n=4).The remaining 18 RCTs were included in the final meta-analysis[23-40].Details of the study selection process are shown in Figure 1.
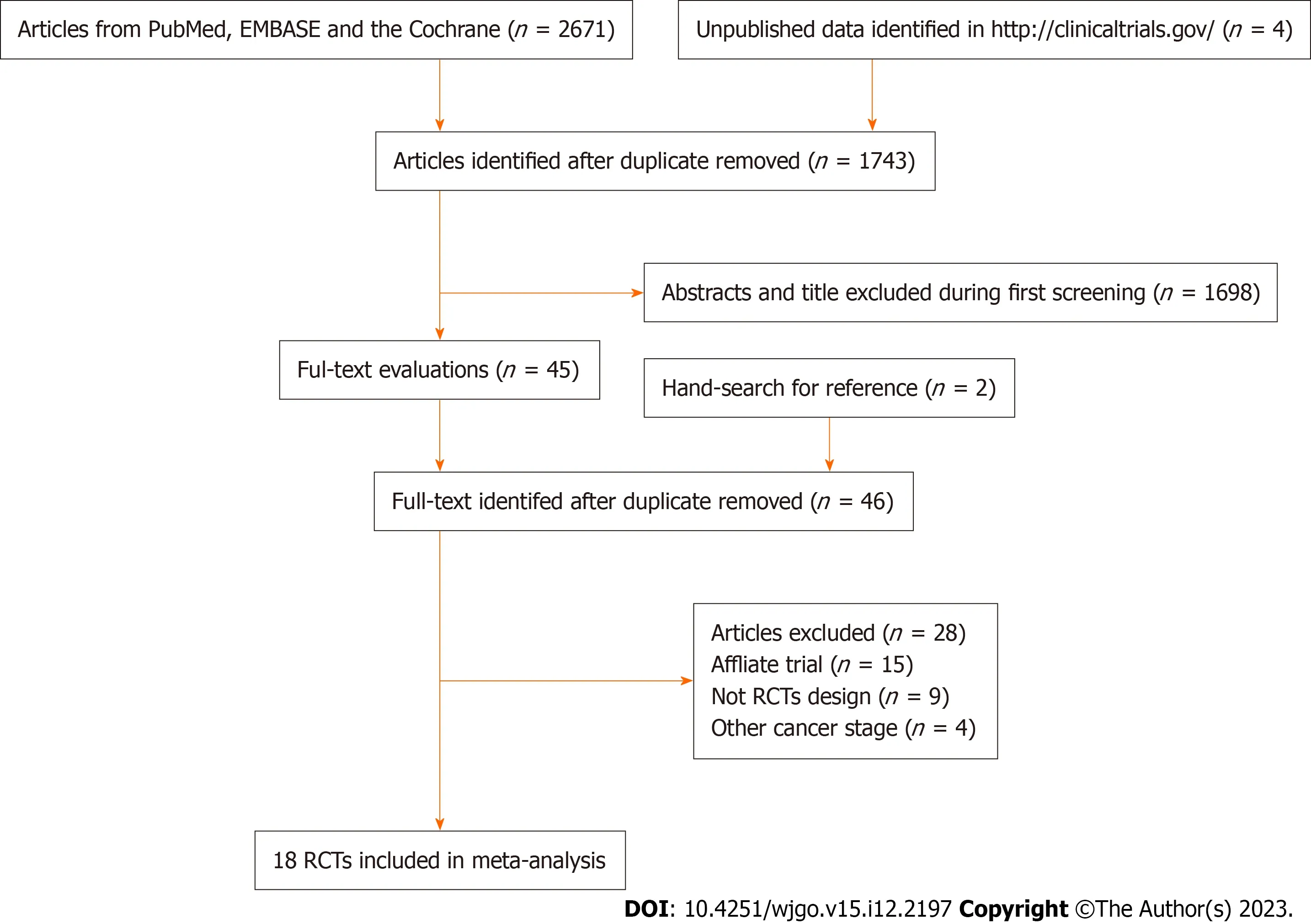
Figure 1 The PRISMA flowchart for the literature search and study selection process. RCT: Randomized controlled trial.
Trials’ characteristics
Table 1 summarizes the baseline characteristics of the identified trials and patients involved.A total of 8533 patients with CRC were included from 18 RCTs,and the sample sizes ranged from 106 to 2509.Seventeen of the included trials were performed in Western countries,including Australia and European countries,whereas the remaining one trial was conducted in China.The follow-up duration ranged from 1.0-10.0 years.Details of the methodological quality of the included trials are listed in Table 2.Most of the included trials were of moderate to high quality,and three were of low quality.
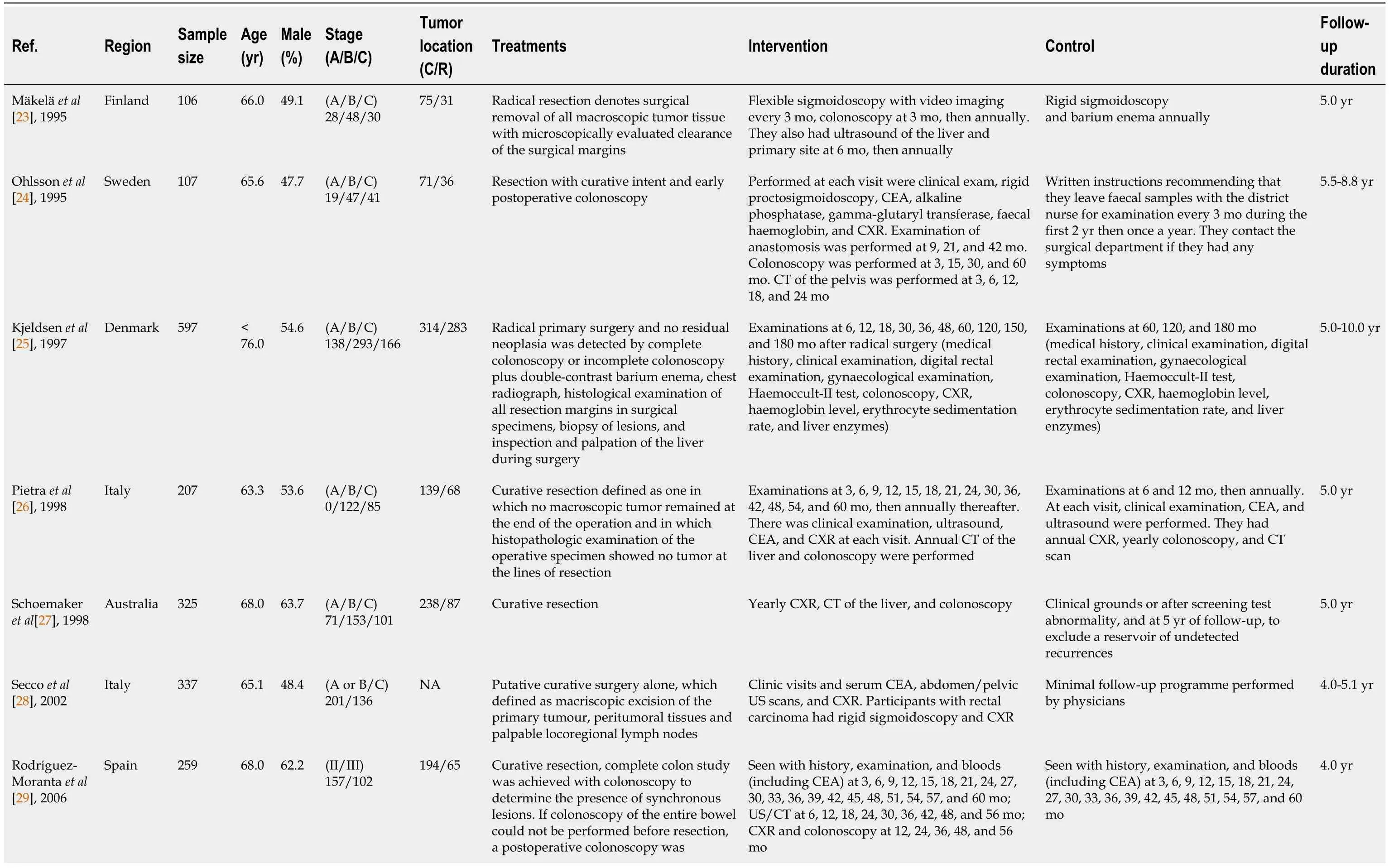
Table 1 The baseline characteristics of included trials and recruited patients
Overall survival
Sixteen trials reported the effects of intensivevsconventional follow-up strategies on overall survival.There was no significant difference between intensive and conventional follow-up strategies for the improvement of overall survival (HR=0.90;95%CI: 0.81-1.01;P=0.062;Figure 2A),and no evidence of heterogeneity was observed across the included trials (I2=0.0%;P=0.643).Sensitivity analysis indicated that an intensive follow-up strategy might be associated with an improvement in overall survival compared to a conventional follow-up strategy (Supplementary material).Subgroup analyses found that intensive follow-up was superior to conventional follow-up in overall survival if the sample size was <500,proportion of males was <60.0%,and follow-up duration was ≥ 5.0 years (Table 3).There were no significant differences between subgroups when stratified by sample size (RHR=1.19;95%CI: 0.95-1.48;P=0.135),mean age (RHR=1.07;95%CI: 0.84-1.35;P=0.584),proportion of males (RHR=1.11;95%CI: 0.89-1.39;P=0.339),tumor location (RHR=1.07;95%CI: 0.84-1.36;P=0.584),and follow-up (RHR=0.86;95%CI: 0.69-1.06;P=0.163).No significant publication bias for overall survival was observed (Pvalue for Egger’s test: 0.753;Pvalue for Begg’s test: 0.558;Supplementary material).
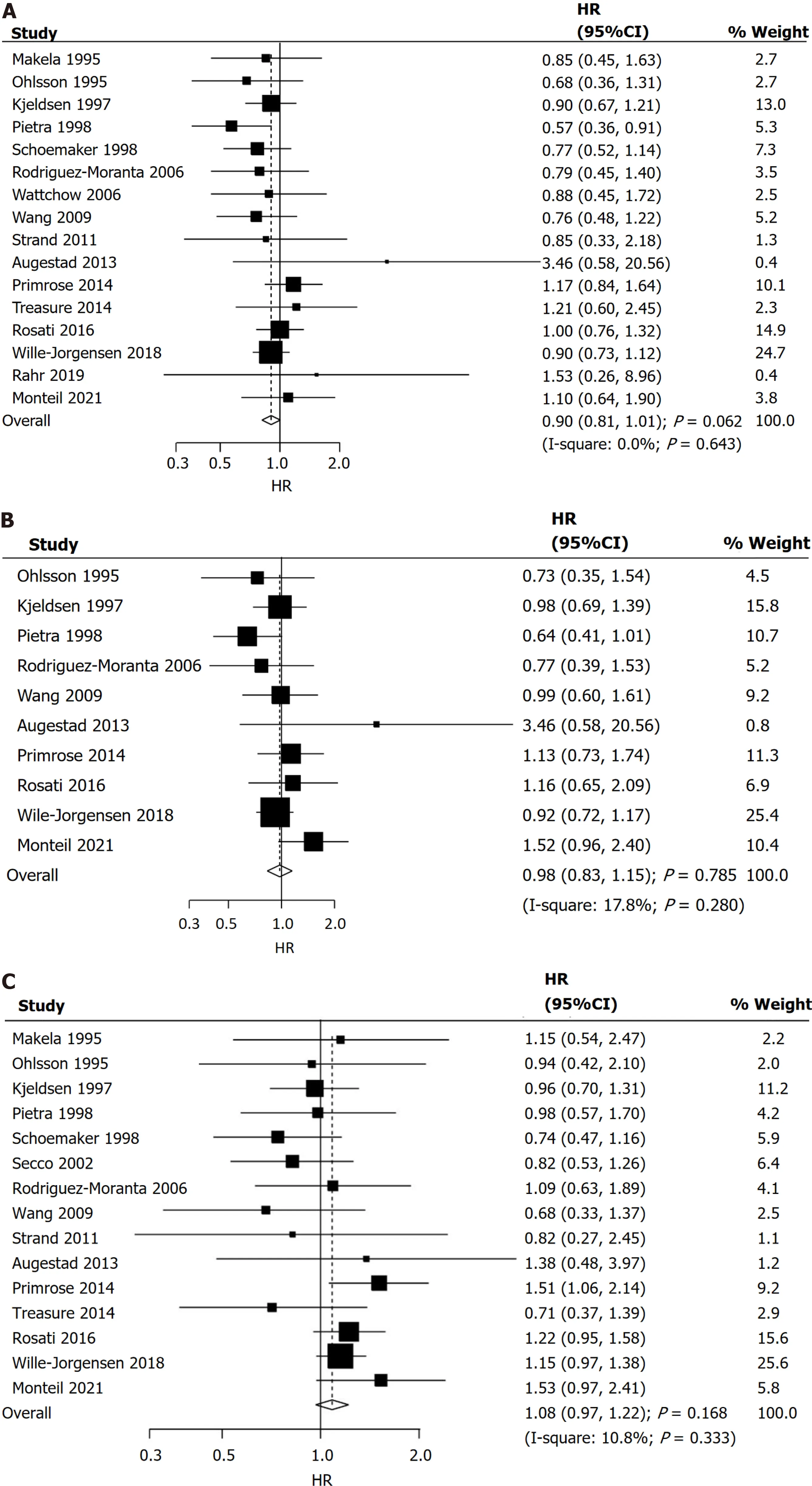
Figure 2 Intensive vs conventional follow-up strategies.A: On overall survival;B: On cancer-specific survival;C: On relapse-free survival;D: On salvage surgery;E: On recurrence;F: On interval recurrences.HR: Hazard ratio;CI: Confidence interval;RR: Risk ratio.
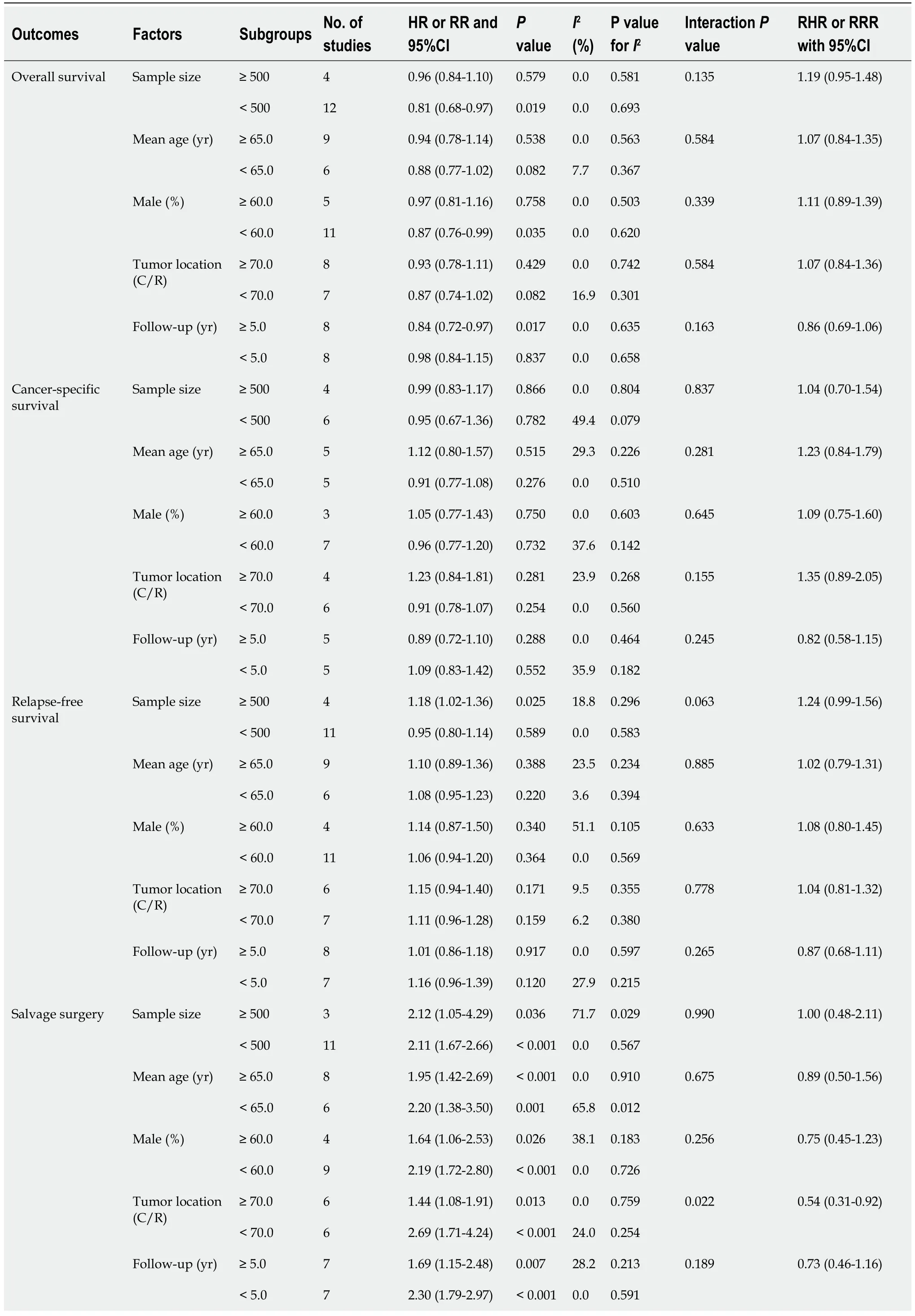
Table 3 Subgroup analyses for investigated outcomes

PET-CT: Positron emission tomography/computed tomography;CXR: Chest radiography;CEA: Carcinoembryonic antigen;CA: Carbohydrate antigen;US: Ultrasound.
Cancer-specific survival
Ten trials reported the effects of intensivevsconventional follow-up strategies on cancer-specific survival.No significant difference between intensive and conventional follow-up strategies was observed for improvement in cancer-specific survival (HR=0.98;95%CI: 0.83-1.15;P=0.785;Figure 2B),and unimportant heterogeneity was detected across the included trials (I2=17.8%;P=0.280).Sensitivity analysis indicated that the pooled analyses were stable and not altered by the sequential removal of a single trial (Supplementary material).The results of the subgroup analyses were consistent with those of the overall analysis in all subgroups (Table 3).Moreover,the differences between subgroups were not statistically significant when stratified by sample size (RHR=1.04;95%CI: 0.70-1.54;P=0.837),mean age (RHR=1.23;95%CI: 0.84-1.79;P=0.281),proportion of males (RHR=1.09;95%CI: 0.75-1.60;P=0.645),tumor location (RHR=1.35;95%CI: 0.89-2.05;P=0.155),and follow-up (RHR=0.82;95%CI: 0.58-1.15;P=0.245).There was no significant publication bias for cancer-specific survival (Pvalue for Egger’s test: 0.492;Pvalue for Begg’s test: 0.858;Supplementary material).
Relapse-free survival
Fifteen trials reported the effects of intensivevsconventional follow-up strategies on relapse-free survival.There was no significant difference between intensive and conventional follow-up strategies for improvement in relapse-free survival (HR=1.08;95%CI: 0.97-1.22;P=0.168;Figure 2C),and non-significant heterogeneity was observed among the included trials (I2=10.8%;P=0.333).Sensitivity analysis revealed that intensive follow-up may be associated with poor relapsefree survival after excluding the trial performed by Schoemakeret al[27] (Supplementary material).Subgroup analyses indicated that an intensive follow-up strategy was associated with poor relapse-free survival when the sample size was ≥ 500 (Table 3).Furthermore,there were no significant differences between subgroups when stratified by sample size (RHR=1.24;95%CI: 0.99-1.56;P=0.063),mean age (RHR=1.02;95%CI: 0.79-1.31;P=0.885),proportion of males (RHR=1.08;95%CI: 0.80-1.45;P=0.633),tumor location (RHR=1.04;95%CI: 0.81-1.32;P=0.778),and follow-up (RHR=0.87;95%CI: 0.68-1.11;P=0.265).No significant publication bias was observed for relapse-free survival (Pvalue for Egger’s test: 0.189;Pvalue for Begg’s test: 0.621;Supplementary material).
Salvage surgery
Fourteen trials reported the effects of intensivevsconventional follow-up strategies on the incidence of salvage surgery.We noted that intensive follow-up significantly increased the risk of salvage surgery compared to a conventional follow-up strategy (RR=1.99;95%CI: 1.57-2.53;P<0.001;Figure 2D),and unimportant heterogeneity was detected among the included trials (I2=25.0%;P=0.184).The pooled analyses for the incidence of salvage surgery were robust and not altered by any specific trial (Supplementary material).The results of the subgroup analyses were consistent with those of the overall analysis,and significant differences between the intensive and conventional follow-up strategies were observed in all subgroups (Table 3).We noted that intensivevsconventional follow-up strategies on salvage surgery in tumor location [colon/rectal ratio (C/R)] ≥ 70.0% was lower than tumor location (C/R) <70.0% (RRR=0.54;95%CI: 0.31-0.92;P=0.022).There was no significant publication bias for salvage surgery (Pvalue for Egger’s test: 0.419;Pvalue for Begg’s test: 1.000;Supplementary material).
Recurrence
Fifteen trials reported the effects of intensivevsconventional follow-up strategies on the risk of recurrence.We noted that the intensive follow-up strategy had no significant effect on the risk of recurrence (RR=1.13;95%CI: 0.98-1.31;P=0.094;Figure 2E),and significant heterogeneity was observed across the included trials (I2=51.6%;P=0.011).Sensitivity analysis indicated that the intensive follow-up strategy was associated with an elevated risk of recurrence when the trial conducted by Seccoet al[28] was excluded (Supplementary material).Subgroup analyses suggested that the intensive follow-up strategy was associated with an increased risk of recurrence when the sample size was ≥ 500 and the mean age was <65.0 years (Table 3).Moreover,the differences between subgroups were not statistically significant when stratifiedby sample size (RRR=1.37;95%CI: 0.970-1.93;P=0.075),mean age (RRR=1.09;95%CI: 0.76-1.56;P=0.645),proportion of males (RRR=1.44;95%CI: 0.66-3.12;P=0.357),tumor location (RRR=0.92;95%CI: 0.68-1.24;P=0.583),and follow-up (RRR=0.85;95%CI: 0.62-1.17;P=0.317).No significant publication bias was observed for recurrence (Pvalue for Egger’s test: 0.492;Pvalue for Begg’s test: 0.843;Supplementary material).
Interval recurrence
Seven trials reported the effects of intensivevsconventional follow-up strategies on the risk of interval recurrence.We noted that intensive follow-up significantly reduced the risk of interval recurrence compared to conventional follow-up (RR=0.59;95%CI: 0.41-0.86;P=0.006;Figure 2F),and significant heterogeneity was observed among the included trials (I2=66.1%;P=0.007).The sensitivity analysis indicated that the pooled analyses were not altered when a particular trial was excluded (Supplementary material).Subgroup analyses found that intensivevsconventional follow-up strategies were associated with a lower risk of interval recurrence if the sample size was <500,mean age was ≥ 65.0,proportion of males was <60.0,tumor location (C/R) was <70.0%,and follow-up duration was <5.0 years (Table 3).Moreover,the effects of intensivevsconventional follow-up strategies on the risk of interval recurrence in the subgroups of tumor location (C/R) ≥ 70.0% (RRR=1.96;95%CI: 1.21-3.20;P=0.007) and follow-up ≥ 5.0 years (RRR=1.77;95%CI: 1.02-3.07;P=0.044) were greater than the corresponding subgroups.There was no significant publication bias for interval recurrence (Pvalue for Egger’s test: 0.790;Pvalue for Begg’s test: 1.000;Supplementary material).
DISCUSSION
Numerous studies have addressed the effects of intensivevsconventional follow-up strategies on the prognosis of patients with non-metastatic CRC treated with curative intent.However,the study results are controversial.This comprehensive quantitative meta-analysis identified 8533 patients with CRC from 18 RCTs,and the patients had a broad range of characteristics.We noted that the intensive follow-up strategy was not associated with overall survival,cancer-specific survival,relapse-free survival,or recurrence compared to the conventional follow-up strategy.Moreover,intensive follow-up significantly increased the incidence of salvage surgery and reduced the risk of interval recurrence compared to conventional follow-up.Finally,the effects of intensive and conventional follow-up strategies differed when stratified by tumor location and follow-up duration.
Several systematic reviews and meta-analyses have compared the effects of intensive treatment with those of conventional follow-up strategies on the prognosis of patients with non-metastatic CRC treated with curative intent[11,41].The results of a meta-analysis conducted by Zhaoet al[11] were consistent with those of a Cochrane review,and the investigated outcomes were similar.A Cochrane review found that using an intensive follow-up strategy did not affect survival outcomes but could increase the incidence of salvage surgeries[41].Although the analysis in this study was comprehensive,stratified analyses were performed only through the intervention protocol and according to the study or patient characteristics.Therefore,this study was conducted to compare the effects of intensivevsconventional follow-up strategies on the prognosis of non-metastatic CRC treated with curative intent by examining published RCTs.
The summary result did not reveal significant differences between intensive and conventional follow-up strategies for improving overall survival.However,this pooled analysis was not stable,and the sensitivity analysis revealed a potentially beneficial role of intensive follow-up on overall survival.A potential reason for this could be that recurrent cases can be detected early and further curative procedures can be applied among patients who receive an intensive follow-up strategy,which could improve the prognosis of CRC after curative surgery.Moreover,patients in the intensive follow-up group showed an increased frequency of clinic visits,tests,and examinations,which could improve CRC prognosis[41].Furthermore,subgroup analyses found that the beneficial effects of intensive follow-up strategies were mainly relevant when the sample size was <500,proportion of males was <60.0%,and follow-up duration was ≥ 5.0,which could be explained by the fact that patients with rectal cancer need longer follow-up durations owing to the delayed liver and lung recurrences[42].Finally,intensive follow-up might be superior to conventional follow-up among women because the difference in lifestyle and compliance among women was better than that among men.
There were no significant differences between the intensive and conventional follow-up strategies in improving cancerspecific survival and relapse-free survival.These results were consistent with those of prior meta-analyses[11,41].However,subgroup analyses found that intensive follow-up was associated with poor relapse-free survival when the sample size was ≥ 500 patients.The potential reason for this could be the large sample size with sufficient power to detect potential differences,and that residual cancer could be detected through a more thorough follow-up[43].Similar to a previous meta-analysis,we noted that intensive follow-up significantly increased the incidence of salvage surgery,which could be explained by the early detection of recurrent cases,and salvage surgery was performed for patients with recurring issues.
Although there was no significant difference in the risk of recurrence between groups,intensive follow-up significantly reduced the risk of interval recurrence.Moreover,intensive follow-up was associated with an increased risk of recurrence when the sample size was ≥ 500 and the mean age was <65.0 years.A potential reason for the risk of recurrence could be that the recurrent cases were consistent and could be affected by the colon/rectal cancer ratio[42].Moreover,most recurrent cases occurred within 36 mo,and the mean age of the patients was significantly related to the tumor stage[44].Interval recurrence was defined as symptomatic recurrence,and recurrent presentation in asymptomatic cases was observed when using an intensive follow-up strategy.
This study has several limitations.First,the disease status and treatments across the included trials were different,which could affect the prognosis of CRC after curative surgery.Second,the follow-up protocol differed among the included trials,and the frequency and content of examination could affect the prognosis of CRC.Third,there was substantial heterogeneity for recurrence and interval recurrence,which was not fully explained using sensitivity and subgroup analyses.Finally,there are inherent limitations of meta-analyses on published articles,including inevitable publication bias and restricted detailed analyses.
CONCLUSION
This study found that an intensive follow-up strategy might have beneficial effects on the overall survival of patients with CRC.Moreover,an intensive follow-up strategy was associated with an increased incidence of salvage surgery and a reduced risk of interval survival.Further large-scale studies should be performed to explore suitable follow-up plans after CRC surgery.
ARTICLE HIGHLIGHTS
Research background
Colorectal cancer (CRC) is the third most frequently diagnosed cancer,and the prognosis of CRC at early stage was relative better.The frequency and content of follow-up strategies play an important role on the prognosis of CRC,and intensive follow-up may improve the prognosis of CRC.
Research motivation
Assess the effects of intensive with conventional follow-up strategies for CRC patients after curative intention using a meta-analysis.
Research objectives
This study aimed to compare the overall survival,cancer-specific survival,relapse-free survival,salvage surgery,recurrence,and interval recurrences between intensive and conventional follow-up strategies for non-metastatic CRC treated with curative intent.
Research methods
The eligible trials were identified from PubMed,Embase,and the Cochrane Library databases from inception until April 2023.All of pooled analyses were calculated using the random-effects model,which considering the underlying varies across included trials.
Research results
We noted intensive follow-up play a beneficial effects in improving overall survival,and interval recurrence as compared with conventional follow-up.Moreover,the incidence of salvage surgery was significantly increased for patients received intensive follow-up.
Research conclusions
This study found intensive follow-up was superior than conventional follow-up for CRC patients after curative intention,which should introduce in clinical practice.
Research perspectives
The results of this study based on randomized controlled trials,and the evidence level for pooled conclusions was high.
FOOTNOTES
Author contributions:Cui LL and Ren ZQ conceived the study concept and participated in its design,data extraction,statistical analysis;Cui LL,Cui SQ,Qu Z,and Ren ZQ contributed to the manuscript drafting,and editing;Cui SQ and Qu Z participated in the literature research;and all authors read and approved the final manuscript.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
PRISMA 2009 Checklist statement:The authors have read the PRISMA 2009 Checklist,and the manuscript was prepared and revised according to the PRISMA 2009 Checklist.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORCID number:Li-Li Cui 0009-0002-6404-5884;Shi-Qi Cui 0009-0006-4950-6063;Zhong Qu 0009-0002-5608-9633;Zhen-Qing Ren 0000-0003-2816-5395.
S-Editor:Wang JJ
L-Editor:A
P-Editor:Xu ZH
 World Journal of Gastrointestinal Oncology2023年12期
World Journal of Gastrointestinal Oncology2023年12期
- World Journal of Gastrointestinal Oncology的其它文章
- Dual primary gastric and colorectal cancer: A complex challenge in surgical oncology
- Conversion immunotherapy for deficient mismatch repair locally unresectable colon cancer: A case report
- Association of MBOAT7 rs641738 polymorphism with hepatocellular carcinoma susceptibility: A systematic review and meta-analysis
- Prognostic value of T cell immunoglobulin and mucin-domain containing-3 expression in upper gastrointestinal tract tumors: A meta-analysis
- Paired-related homeobox 1 induces epithelial-mesenchymal transition in oesophageal squamous cancer
- Evaluating the causal relationship between human blood metabolites and gastroesophageal reflux disease