
Short-term efficacy assessment of transarterial chemoembolization combined with radioactive iodine therapy in primary hepatocellular carcinoma
2023-03-17 07:45:56LeiWangKunHuangYuZhangYiFanWuZhenDongYueZhenHuaFanFuQuanLiuYongWuLiJianDong
Lei Wang,Kun Huang,Yu Zhang,Yi-Fan Wu,Zhen-Dong Yue,Zhen-Hua Fan,Fu-Quan Liu,Yong-Wu Li,Jian Dong
Lei Wang,Yu Zhang,Yi-Fan Wu,Zhen-Dong Yue,Zhen-Hua Fan,Fu-Quan Liu,Department of Interventional Radiology,Beijing Shijitan Hospital,Capital Medical University,Beijing 100038,China
Kun Huang,Department of Radiology,Chinese Medical University Affiliated First Hospital,Shenyang 110001,Liaoning Province,China
Yong-Wu Li,Department of Nuclear Medicine,The Fifth Center of People's Liberation Army General Hospital,Beijing 100071,China
Jian Dong,Department of Radiology,Beijing Shijitan Hospital,Capital Medical University,Beijing 100038,China
Abstract BACKGROUNDTransarterial chemoembolization(TACE)is an effective treatment for primary hepatocellular carcinoma(PHC).Radioactive iodine therapy has been used in the treatment of advanced PHC,especially in patients with portal vein tumor thrombosis.However,data on the therapeutic effect of TACE combined with radioactive iodine therapy in PHC are scarce.AIM To investigate the clinical efficacy of TACE combined with radioactive iodine implantation therapy in advanced PHC via perfusion computed tomography(CT).METHODS For this study,98 advanced PHC patients were recruited and divided randomly into the study and control groups.Patients in the study group were treated with TACE combined radioactive iodine implantation therapy.Patients in the control group were treated with only TACE.The tumor lesion length,clinical effect,serum alpha-fetoprotein(AFP)and CT perfusion parameters were compared before and after therapy,and statistical analysis was performed.RESULTS There was no significant difference in tumor length and serum AFP between the study and control groups(P > 0.05)before treatment.However,the tumor length and serum AFP in the study group were lower than those in the control group 1 mo and 3 mo after therapy.After 3 mo of treatment,the complete and partial remission rate of the study group was 93.88%,which was significantly higher than the control group(77.55%)(P < 0.05).Before treatment,there were no significant differences between the two groups on the perfusion CT variables,including the lesion blood volume,permeability surface,blood flow,hepatic artery flow and mean transit time(P > 0.05).After 3 mo of treatment,all perfusion CT variables were lower in the study group compared to the control group(P < 0.05).The survival time of patients in the study group was 22 mo compared to 18 mo in the control group,which was significantly different[log rank(Mantel-Cox)= 4.318,P = 0.038].CONCLUSIONTACE combined with radioactive iodine implantation in the treatment of advanced PHC can inhibit the formation of blood vessels in tumor tissue and reduce the perfusion level of tumor lesions,thereby improving the clinical efficacy and prolonging the survival time of patients.
Key Words:Transarterial chemoembolization;Radioactive iodine;Primary hepatocellular carcinoma;Perfusion;Computed tomography
lNTRODUCTlON
Primary hepatocellular carcinoma(PHC)is a malignant tumor with a high incidence in the Chinese population.It can develop in hepatocytes and intrahepatic bile duct cells and cause clinical symptoms[1-3].Surgical resection is the primary treatment for early-stage hepatocellular carcinoma.However,due to an insidious onset and atypical early symptoms,more than 80% of hepatocellular carcinoma patients are diagnosed with metastasis and are ineligible for surgical treatment[1,4-6].
Transarterial chemoembolization(TACE)is the main treatment for patients with inoperable hepatocellular carcinoma.It can release chemotherapeutic drugs rapidly and maintain a high blood concentration in the organ to inhibit rapid local tumor growth.However,its long-term efficacy is inadequate[5-8].Radioactive iodine(125I)implantation is a new means of radiotherapy with a high radiation dose and precise localization.It is also a potential treatment option for patients with PHC[8-11].As such,this study investigated the short-term clinical efficacy of TACE combined with125I implantation in the treatment of patients with PHC.
MATERlALS AND METHODS
Patient data
From January 2016 to June 2018,98 patients with PHC,who were scheduled for treatment with interventional embolization chemotherapy,were selected as study subjects.They were randomly divided into the study group(n= 49)and the control group(n= 49).The inclusion criteria included:(1)Diagnosis of PHC according to the criteria in the Guidelines for Diagnosis and Treatment of Primary Hepatocellular Carcinoma[10,12-15];(2)PHC confirmed by computed tomography(CT),magnetic resonance imaging and liver puncture biopsy;(3)Patients aged 19-79 years;(3)PHC patients with preoperative liver function grade A or B according to the Child-Pugh classification;(4)Stage C and D lesions according to the Barcelona Clinic Liver Cancer(BCLC)staging system[10,12-15];(5)Preoperative assessment of survival time > 3 mo;and(6)PHC patients with survival status score 0-2 based on the Eastern Cooperative Oncology Group Performance Status[13].The exclusion criteria included:(1)Metastatic hepatocellular carcinoma;(2)Biliary obstruction due to tumor infiltration of the bile duct;(3)Hepatic artery-portal vein fistula formation;(4)Mental illness and intellectual disability;(5)Severe renal dysfunction;and(6)Other contraindications to treatment.Study protocols were reviewed by ethics experts and implemented with presurgical informed consent from patients and families.
Methods
Treatment method:The control group was treated with TACE,which included the following chemotherapy drugs:0.75-1.25 g of 5-fluorouracil;80-120 mg of cisplatin;20 mg of oxaliplatin;80-140 mg of epirubicin;and super-liquidated iodine oil as an embolic agent.The doses of chemotherapy drugs and iodine oil were adjusted according to the tumor size and blood supply.
The study group was treated with TACE combined with125I implantation.After 1 wk of TACE,a CT scan was performed to confirm the location,structure and specific size of the tumor and its surrounding tissues,and CT navigation and localization were performed.125I particles were placed in the patients after CT determined that the needle tip reached the target area,and the distribution was recorded.The puncture needle was withdrawn after successful placement was confirmed by CT scan,and the site was sterilized and bandaged.
Evaluation indices:After being admitted and treated,3 mL of venous blood was drawn to measure serum alpha-fetoprotein(AFP)by enzyme-linked immunoassay using an enzyme-labeled instrument(BD Biosciences,Franklin Lakes,NJ,United States).The CT perfusion parameters measured were blood volume(BV),permeability surface(PS),blood flow(BF),hepatic artery flow(HAF),and mean transit time(MTT).
Lesions were classified as complete remission(CR),partial remission(PR),stable disease and progressive disease according to the changes in the lesions before and after treatment.CR was defined as solid tumors,other than nodal disease,where the target lesion completely disappeared or all target nodes had shrunk to normal size for 4 wk or more.PR was defined as the sum of long diameters selected for target lesions and short diameters selected for target nodes reduced by ≥ 30% when compared to baseline for 4 wk or more.Progressive disease was defined by the sum of the target lesion diameters exceeding the reference value(smallest sum of the measured target lesion diameters)by 20% or more and the absolute value increased by ≥ 5 mm or ≥ 1 new lesions having appeared and not completely/partially in remission before the lesions grew in size or increased in number.Stable disease was defined when the volume and number of lesions were between PR and progressive disease.
Statistical processing
SPSS 21.0 software(IBM Corp.,Armonk,NY,United States)was used for statistical comparative analysis of the data.The measurement data,such as tumor length and AFP level,were expressed by mean ± SD,and thettest was adopted for comparison between groups.χ2test was adopted for comparative analysis between groups(clinical efficacy and other count data).The Kaplan-Meier method was used to model the survival analysis.P< 0.05 was considered a statistically significant difference.
RESULTS
Comparison of baseline characteristics between the two groups
In the study group,the patients ranged from 43-years-old to 76-years-old(56.3 ± 7.2 years)and included 28 males and 21 females.Thirty patients were BCLC stage C and 19 patients were BCLC stage D.The maximum diameter of the tumor lesion was 6.31 ± 2.00 cm.There were 32 cases of Child-Pugh grade A and 17 cases of Child-Pugh grade B PHC.In the control group,the patients ranged from 40-years-old to 75-years-old(55.5 ± 6.8 years)and included 31 males and 18 females.There were 34 cases of BCLC stage C and 15 cases of BCLC stage D.The maximum diameter of tumor lesion was 6.14 ± 1.89 cm.There were 30 cases of Child-Pugh grade A and 19 cases of Child-Pugh grade B PHC.There were no statistically significant differences between these baseline characteristics of the two groups(P> 0.05).
Comparison of changes of tumor lengths between the two groups
Before treatment,there was no statistically significant difference in tumor lengths between the study group and the control group(P> 0.05).The tumor lengths of the study group were significantly lower than those of the control group after 1 mo and 3 mo of treatment(P< 0.05)(Table 1 and Figure 1A).
Comparison of changes in serum AFP levels in the two groups of patients
Before treatment,the difference in serum AFP between the study group and the control group were not statistically significant(P> 0.05).After 1 mo and 3 mo of treatment,the serum AFP of the study group was lower than that of the control group(P< 0.05)(Table 2 and Figure 1B).
Comparison of treatment efficacy in the two groups of patients
After 3 mo of treatment,the CR + PR rate in the study group was 93.88%,which was higher than in the control group(77.55%,P< 0.05)(Table 3).
Comparison of CT perfusion parameters of tumor lesions in the two groups
Before treatment,there was no statistically significant difference between the BV,PS,BF,HAF and MTT measurements of the lesions in the study group and the control group(P> 0.05).After 3 mo,the BV,PS,BF,HAF and MTT measurements in the study group were lower than those in the control group(P< 0.05)(Table 4).
Comparative analysis of survival between the two groups of patients
The patients in both groups were followed up and observed.There was no statistically significant difference between the 3-year survival rate of patients in the study group and the control group(P> 0.05).However,the survival time of patients in the study group was 22 mo,which was significantly longer than 18 mo in the control group[log rank(Mantel-Cox)= 4.318,P= 0.038](Table 5 and Figure 2).
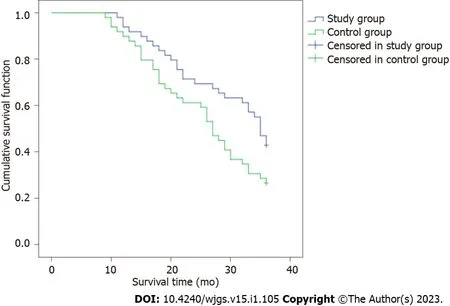
Figure 2 Kaplan-Meier survival curvefor the two groups of patients.Control group:Treated with transarterial chemoembolization(TACE);Study group:Treated with TACE and radioactive iodine implantation.
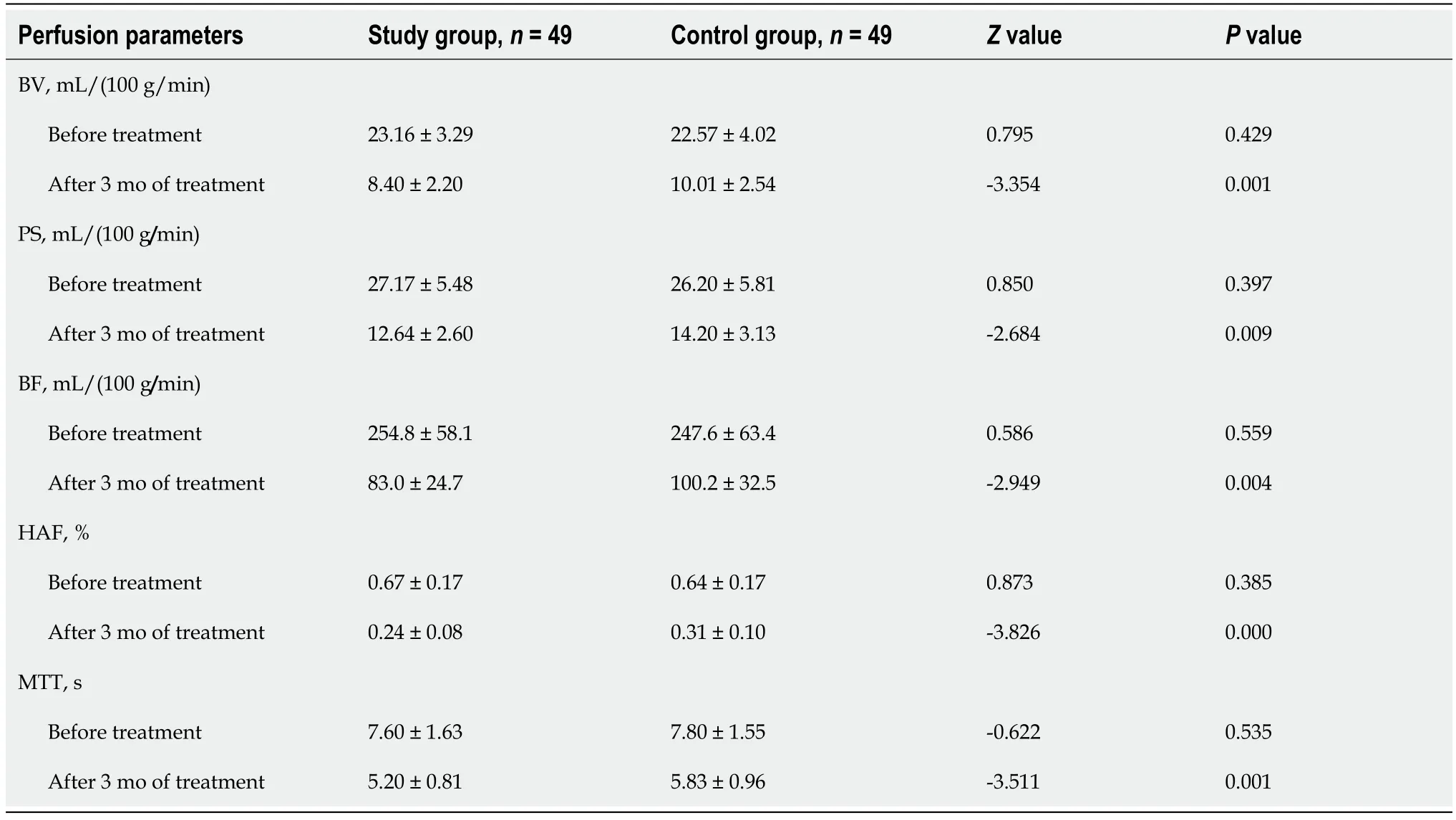
Table 4 Comparison of computed tomography perfusion parameters of the lesions in the two groups of patients

Table 5 Comparison of survival rates between the two groups
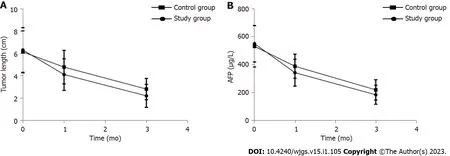
Figure 1 Study group compared to the control group.A:Tumor lengths decreased in the study group compared to the control group;B:Serum alphafetoprotein levels decreased in the study group compared to the control group.Control group:Treated with transarterial chemoembolization(TACE);Study group:Treated with TACE and radioactive iodine implantation.AFP:Alpha-fetoprotein.

Table 1 Comparison of changes in tumor lengths in the two groups of patients

Table 2 Comparison of serum alpha-fetoprotein levels in the two groups of patients

Table 3 Comparison of treatment efficacy in the two groups
DlSCUSSlON
Epidemiological studies suggest that the incidence rate of liver cancer in China has reached 29/100000,with a mortality rate of 26.04/100000[3,10,12,16].PHC is caused by various factors including hepatitis B virus infection,aflatoxin,toxic substances,alcohol,nitrite,environmental pollution,etc[7,11,15,17].Surgery is the most effective treatment for PHC.However,due to insidious early symptoms,the time for surgical treatment is often missed[10,17-19].
TACE is the first choice of treatment for inoperable liver cancer surgery[7,20,21].It directly delivers embolic agents,iodinated oil and chemotherapeutic drugs,which can cause tumor ischemia and hypoxia,and are injected into the hepatic artery through a catheter.This catheter also blocks the blood supply,which inhibits tumor growth and metastasis[1,7,11,18,21].Unfortunately,as the clinical utilization of TACE increased,several disadvantages were found,including need for multiple treatments,incomplete embolizations,and increased chance of recurrence and metastasis due to vascular endothelial growth factor release.A single TACE treatment typically has a dissatisfactory longterm treatment effect.
125I implantation is a new minimally invasive interventional technique that is effective in treating lung cancer,liver cancer,and kidney cancer[8-11].Radioactive particles,like125I,are encased in a very small silver rod or titanium alloy and form a very small particle that contains a very strong radioactive isotope[8,9,11].125I particles are a type of brachytherapy.Due to the shorter range(1 cm action radius),lower capacity and weak penetration ability of brachytherapy,there is less impact on normal cells while still effectively killing tumor cells.After the radioactive particles are implanted inside the tumor,rays are continuously emitted to kill tumor cells for a certain period of time.
The results of this study showed that after 1 mo and 3 mo of treatment,the tumor lengths in the study group were lower than those in the control group,and the CR + PR rate of the study group was significantly higher than that of the control group,suggesting that TACE combined with125I implantation has a better anti-tumor effect than TACE alone and can significantly inhibit tumor growth[8-11].The survival time of the patients in the study group was 22 mo,which was significantly longer than 18 mo in the control group.This result suggests that TACE combined with125I implantation can prolong the survival time of patients with PHC,and TACE and radionuclide therapy are an effective combination.
AFP is a broad-spectrum tumor marker with high sensitivity and specificity in monitoring disease changes and diagnosing PHC[1,2,10,22].This study found that the serum AFP in the study group was lower than that in the control group after 1 mo and 3 mo of treatment,indicating that TACE combined with125I implantation can reduce the level of AFP.This likely occurred due to the ability of125I particles to ionize water molecules and cause direct damage to DNA.This affects the DNA repair mechanisms and can reduce AFP levels.
The CT perfusion imaging technique can effectively evaluate the hemodynamic changes of hepatocellular carcinoma tumors.This provides feedback on the micro-angiogenesis of tumor tissues and the surrounding tissues,which will direct the treatment of the cancer[12,16,23].This study showed that after 3 mo of treatment the BV,PS,BF,HAF,and MTT measurements in the study group were lower than those in the control group,indicating that TACE combined with125I implantation can effectively reduceperfusion levels of tumor lesions,which improves clinical efficacy.125I particles implanted into tumor tissue release low-energy γ-rays,which exert direct killing effects,induce an inflammatory response,promote antigen-presenting cells such as macrophages to process and take up antigenic information,and promote B cells and T cells to participate in the tumor immune process[9,11].In addition,the mammalian target of rapamycin pathway may form radiotherapy-specific proteins after several hours of irradiation.This activates lymphocytes,and the cytokine network regulatory mechanism is stimulated through the secretion of large amounts of cytokines,which activates tumor-specific immune processes to kill tumor cells.Related studies suggested that lower doses of γ-rays are more beneficial because they increase the responsiveness of lymphocytes,promote the production of antibodies,enhance the toxic effect on tumor cells,and improve the treatment effect[8,12].
CONCLUSlON
This study confirmed that TACE combined with125I implantation for the treatment of patients with advanced PHC could better inhibit the formation of blood vessels in tumor tissues and reduce the perfusion level of tumor lesions compared to TACE alone.Therefore,with the development of technology,the combined multidisciplinary treatment improves the anti-tumor effect and plays a synergistic role in prolonging the survival time of patients,which is worthy of further clinical research.
ARTlCLE HlGHLlGHTS
Research background
Primary hepatocellular carcinoma(PHC)is a malignant tumor with a high incidence in the Chinese population.Transarterial chemoembolization(TACE)is an effective treatment for PHC.Radioactive iodine(125I)therapy has been used in the treatment of advanced PHC,especially in patients with portal vein tumor thrombosis.
Research motivation
Due to insidious onset and atypical early symptoms of PHC,more than 80% of hepatocellular carcinoma patients are diagnosed with metastasis and are ineligible for surgical treatment.Therefore,it is crucial to develop effective treatment methods,such as TACE and125I therapy.However,the data on the therapeutic effect of TACE combined with125I therapy in PHC is scarce.
Research objectives
To investigate the short-term efficacy of TACE combined with125I in patients with PHC.
Research methods
Ninety-eight patients with PHC were recruited and randomly divided into the study group(n= 49,treatment with TACE and125I therapy)and the control group(n= 49,treatment with TACE alone).The tumor length,alpha-fetoprotein(AFP)level,and computed tomography(CT)perfusion were recorded.Complete remission,partial remission(PR),stable disease and progressive disease were evaluated for all patients.Then,the efficacy was compared between the control group and the study group.
Research results
The tumor length and serum AFP level were lower in the study group compared to those in the control group after 1 mo and 3 mo of therapy.After 3 mo of treatment,the complete and PR rate in the study group was higher than in the control group(93.88% vs 77.55%,P< 0.05).Furthermore,CT perfusion parameters,including blood volume,permeability surface,blood flow,hepatic artery flow,and mean transit time,were all lower in the study group than in the control group(P< 0.05).The survival time of patients in the study group was 22 mo,which was significantly longer than 18 mo in the control group[log rank(Mantel-Cox)= 4.318,P= 0.038].
Research conclusions
For advanced PHC patients,TACE combined with125I implantation better inhibits the formation of blood vessels in tumor tissues and further reduces the perfusion level of tumor lesions compared to TACE alone.The combination of TACE and125I therapy improves clinical efficacy and plays a synergistic role in prolonging the survival time of patients.
Research perspectives
TACE combined with125I implantation or other therapeutic methods,such as radiofrequency ablation,programmed cell death ligand 1 therapy,and immune therapy,should be investigated in advanced PHC patients in the future.
FOOTNOTES
Author contributions:Dong J,Liu FQ and Wang L designed the report;Zhang Y,Wu YF,Yue ZD,Fan ZH,Huang K and Li YW collected the clinical data;Wang L,Huang K,Li YW and Zhang Y analyzed the data and wrote the paper;Huang K,Li YW,Dong J and Liu FQ performed quality control;Liu FQ contributed to administrative and financial support;and all authors read and approved the final version of the manuscript.
Supported bythe National Natural Science Foundation of China General Program,No.81871461.
lnstitutional review board statement:This study was approved by the Ethics Committee of the Beijing Shijitan Hospital,Capital Medical University,No.201801.
Clinical trial registration statement:This study is registered at ClinicalTrials.gov,registration number ChiCTR-DDC-16009986(www.chictr.org.cn/edit.aspx?pid=16996&htm=4).
lnformed consent statement:Written informed consent was obtained from each patient.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
Data sharing statement:No additional data are available.
CONSORT 2010 statement:The authors have read the CONSORT 2010 Statement,and the manuscript was prepared and revised according to the CONSORT 2010 Statement.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See:https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Lei Wang 0000-0002-4374-059X;Jian Dong 0000-0002-2643-0370.
S-Editor:Wang JJ
L-Editor:A
P-Editor:Wang JJ
 World Journal of Gastrointestinal Surgery2023年1期
World Journal of Gastrointestinal Surgery2023年1期
- World Journal of Gastrointestinal Surgery的其它文章
- lntestinal erosion caused by meshoma displacement:A case report
- Associate factors for endoscopic submucosal dissection operation time and postoperative delayed hemorrhage of early gastric cancer
- Effects of postoperative use of proton pump inhibitors on gastrointestinal bleeding after endoscopic variceal treatment during hospitalization
- lmpact of body mass index in elderly patients treated with laparoscopic liver resection for hepatocellular carcinoma
- New perspectives on robotic pancreaticoduodenectomy:An analysis of the National Cancer Database
- Development and validation of a novel nomogram for predicting overall survival in gastric cancer based on inflammatory markers