
Associate factors for endoscopic submucosal dissection operation time and postoperative delayed hemorrhage of early gastric cancer
2023-03-17 07:45:54RenSongCaiWeiZhongYangGuangRuiCui
Ren-Song Cai,Wei-Zhong Yang,Guang-Rui Cui
Ren-Song Cai,Wei-Zhong Yang,Guang-Rui Cui,Digestive Endoscopy Department,the Second Affiliated Hospital of Hainan Medical University,Haikou 570311,Hainan Province,China
Abstract BACKGROUND Endoscopic submucosal dissection(ESD)is a treatment for early gastric cancer with the advantages of small invasion,fewer complications,and a low local recurrence rate.However,there is a high risk of complications such as bleeding and perforation,and the operation time is also longer.ESD operation time is closely related to bleeding and perforation.AIM To investigate the influencing factors associated with ESD operation time and postoperative delayed hemorrhage to provide a reference for early planning,early identification,and prevention of complications.METHODS We conducted a retrospective study based on the clinical data of 520 patients with early gastric cancer in the Second Affiliated Hospital of Hainan Medical University from January 2019 to December 2021.The baseline data,clinical features,and endoscopic and pathological characteristics of patients were collected.The multivariate linear regression model was used to investigate the influencing factors of ESD operation time.Logistic regression analysis was carried out to evaluate the influencing factors of postoperative delayed hemorrhage.RESULTS The multivariate analysis of ESD operation time showed that the maximum lesion diameter could affect 8.815% of ESD operation time when other influencing factors remained unchanged.The operation time increased by 3.766% or 10.247% if the lesion was mixed or concave.The operation time increased by 4.417% if combined with an ulcer or scar.The operation time increased by 3.692% if combined with perforation.If infiltrated into the submucosa,it increased by 2.536%.Multivariate analysis of delayed hemorrhage after ESD showed that the maximum diameter of the lesion,lesion morphology,and ESD operation time were independent influencing factors for delayed hemorrhage after ESD.Patients with lesion ≥ 3.0 cm(OR = 3.785,95%CI:1.165-4.277),lesion morphology-concave(OR = 10.985,95%CI:2.133-35.381),and ESD operation time ≥ 60 min(OR = 2.958,95%CI:1.117-3.526)were prone to delayed hemorrhage after ESD.CONCLUSION If the maximum diameter of the lesion in patients with early gastric cancer is ≥ 3.0 cm,and the shape of the lesion is concave,or accompanied by an ulcer or scar,combined with perforation,and infiltrates into the submucosa,the ESD operation will take a longer time.When the maximum diameter of the lesion is ≥ 3.0 cm,the shape of the lesion is concave in patients and the operation time of ESD takes longer time,the risk of delayed hemorrhage after ESD is higher.
Key Words:Early gastric cancer;Endoscopic submucosal dissection;Operation time;Delayed hemorrhage
lNTRODUCTlON
Gastric cancer is a malignant tumor originating from the gastric epithelium.Early gastric cancer is generally defined as invasive gastric cancer that invades no more deeply than the submucosa,regardless of lymph node status and metastasis.In 2018,there were 1033701 new gastric cancer cases worldwide,accounting for 5.7% of all types of cancer,making gastric cancer the fifth most common cancer after lung,breast,colorectal,and prostate cancer.In 2018,782685 patients died of gastric cancer,accounting for 8.2% of all cancer deaths,which is the third major cause of cancer death worldwide[1].The incidence of gastric cancer is also high in China.According to the latest cancer data statistics in China,480000 people suffered from gastric cancer in 2020,accounting for 10.5% of all new cancer cases,and 370000 new deaths,accounting for 12.4% of cancer-related deaths,which made gastric cancer the third most deadly cancer among all types of cancers[2].The good news is the 5-year survival rate of patients with early gastric cancer after active treatment can reach 90%[3].To date,endoscopic submucosal dissection(ESD)has been used as the first-line treatment for early gastric cancer with the advantages of small invasion,fewer complications,low resection rate,and local recurrence rate[4,5].However,as a highly sophisticated endoscopic technique,ESD requires advanced endoscopic equipment and skilled operation practices.The risk of complications such as bleeding and perforation is high,and the operation time is also long.Studies have shown that ESD operation time is closely related to bleeding,perforation,postoperative pneumonia,deep vein thrombosis,and carbon dioxide retention,which increases medical costs[6].The main postoperative complication of ESD was delayed hemorrhage,with an incidence of 4.5%-5.7%.If not treated promptly,it can lead to serious cardiovascular complication[7].Therefore,this study aims to explore the influencing factors of ESD operation time and postoperative delayed hemorrhage,which would provide a reference for early planning,early identification,and complications prevention of ESD operation.
MATERlALS AND METHODS
Study population
The patients with early gastric cancer who received ESD treatment in the Department Endoscopic Center of the Second Affiliated Hospital of Hainan Medical University from January 2019 to December 2021 were retrospectively analyzed.
Inclusion criteria:(1)Patients with early gastric cancer confirmed by endoscopic biopsy and pathological examination;(2)Patients that found no regional lymph nodes and distant metastasis in endoscopic ultrasonography and other imaging examinations;(3)All patients and their relatives were informed of the risks and benefits of ESD and signed a written informed consent;(4)The patient was informed of the study and agreed to participate;and(5)The patient’s information is complete.
Exclusion criteria:(1)Tumor infiltrating into muscular layer or serosa;(2)Patients with severe heart,brain,lung,and other important organ dysfunction;(3)Coagulation dysfunction;(4)Patients with a high risk of anesthesia or intolerance;(5)Suspicious lymph node metastasis;and(6)Two or more lesions appeared.
The baseline data,clinical features,and endoscopic and pathological characteristics of patients were collected,including gender,age,underlying diseases,medication history,lesion location,lesion shape,maximum lesion diameter,ulcer and scar,perforation,pathological diagnosis,depth of invasion,delayed hemorrhage and ESD operation time(min).
ESD operation process and postoperative treatment
GIFQ260J gastroscope with an additional water supply function was used(Olympus,Japan).The front end of the gastroscope is provided with a soft transparent cap(Olympus,Japan).High-frequency electrical uses erbotomicc200 or vio200d(Erbe,Germany).Under general anesthesia,the submucosal injection during ESD operation consisted of glycerol,fructose solution,an appropriate amount of methylene blue,and epinephrine at a ratio of 1:10000.Sodium hyaluronate solution was diluted with normal saline(1:5)when necessary.The lesion was located under endoscopy,and the boundary between the lesion and the normal mucosa was determined by NBI amplification and 2.5% Lugol solution staining.Thermocoagulation markers were made around the lesion every 0.5 cm from 0.3 to 0.5 cm from the lesion border.The mucosa and submucosa were separated by submucosal injection along the lesion boundary.An incision was cut at about 0.5 cm outside the marker,and then the lesion was cut along the mucosa of the lesion edge with a dual knife until the submucosa was reached,and the lesion was gradually stripped along the submucosa.During the stripping,the hemostatic forceps were used intermittently until the tumor was completely stripped.Finally,thermal hemostatic forceps were used to stop the wound,and titanium clips were used to seal the wound for patients with deep dissection or cracks in the muscularis propria.The vital signs of patients were closely monitored after the operation.In this study,all ESD procedures were performed by a professional endoscopic physician with more than 15 years of technical experience using the same equipment.
The postoperative treatment and follow-up measures of ESD included postoperative placement of a gastric tube.According to the needs of the patient,the patient was fasted for 3-5D and received hemostasis,acid suppression,anti-infection,and intravenous nutritional support.Gastric tube drainage and patients with abdominal pain,abdominal distension,and other signs were closely observed.Patients continued to take gastric mucosal protective agents and proton pump acid inhibitors for 8 wk after discharge.The endoscopic review was performed once every 3,6,and 12 mo after the operation,and then once a year.Postoperative chest and abdomen computed tomography examination was performed once a year.
ESD operation time is defined as the time(min)from the circumferential marking of the lesion to the complete resection of the lesion.Delayed hemorrhage was considered by the following situations within 24 h to 30 d after ESD:(1)Vomiting,dizziness,melena,and other symptoms;(2)Blood pressure drop > 20 mmHg or heart rate increase by 20 times/min;(3)Endoscopic examination confirmed surgical wound bleeding;and(4)Hemoglobin level decreased ≥ 2 g/dL after endoscopic treatment.At the time of discharge,researchers instructed patients on how to identify delayed bleeding,and collected patients’ delayed bleeding by phone or face-to-face after discharge.
Ethical principles
This study is a retrospective study.All patient data obtained,recorded,and managed will be used for this study only,and all patient information will be kept strictly confidential and will not cause any harm to the patient.In addition,the research scheme was approved by the Ethics Committee of the Second Affiliated Hospital of Hainan Medical University.
Statistical analysis
SPSS26.0 statistical software was used for statistical analysis.The numerical variables that meet the normal distribution were described by mean ± SD,and the classification variables were described by frequency(percentage).The influencing factors of ESD operation time were analyzed by univariate analysis and multivariate analysis.In single-factor analysis,Pearson correlation analysis was used for age,independent samplet-test was used for two classification factors,variance analysis was used for multi-classification factors,and LSD test was used for pairwise comparison.The multivariate linear regression model was used for the multivariate analysis of ESD operation time.Also,a single-factor analysis of delayed hemorrhage after the operation was performed byχ2test,and multivariate logistic regression analysis was used to analyze the influencing factors of delayed hemorrhage after ESD.Test level α = 0.05.
RESULTS
Patient characteristics
From January 2019 to December 2021,there were 551 patients with early gastric cancer received ESD treatment in total in our endoscopic center.As shown in the figure,endoscopy confirmed early gastric cancer(Figure 1A and B).Among them,24 patients had incomplete data,and 7 patients did not meet the criteria for admission and discharge.Therefore,520 patients with early gastric cancer were collected for this retrospective study.There were 367 males and 153 females,with a ratio of 2.40:1.The age of patients was between 31 and 84 years old and the average age was 57.81 ± 10.56 years old.The median maximum diameter of the lesion was 3.0 cm,ranging from 0.35 cm to 10.55 cm.The average operation time was 66.78 ± 40.89 min(10-160 min).In total,508(97.69%)lesions were completely resected,and 499(95.96%)lesions met the standard of curative resection.There were 189 cases of upper gastric lesions,112 cases of middle gastric lesions,and 219 cases of lower gastric lesions.Delayed hemorrhage occurred in 43 patients after ESD(8.27%).Hemorrhage patients underwent emergency endoscopic hemostasis and hemostasis was successful.11 patients needed a blood transfusion.
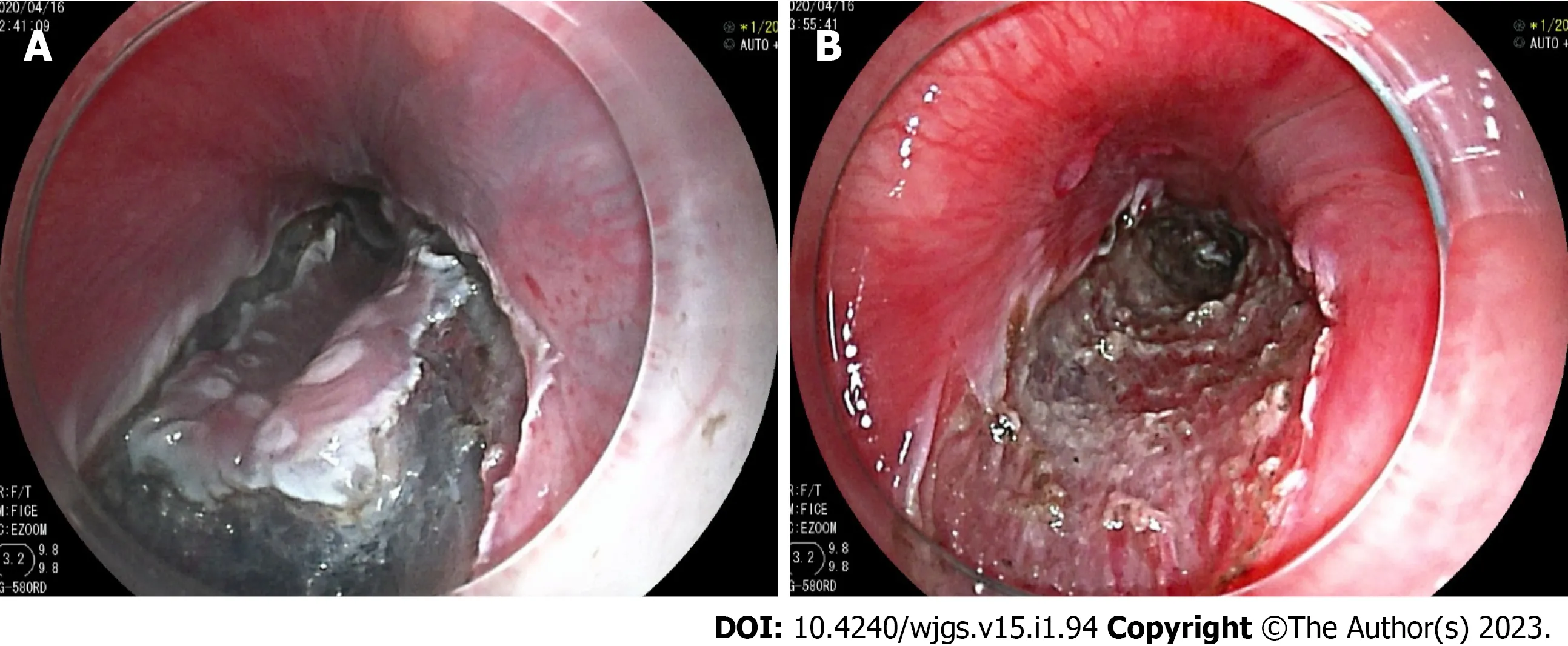
Figure 1 Process picture of endoscopic submucosal dissection for early gastric cancer.A:Under gastroscope,gastric mucosal lesions in the anterior wall of the gastric body can be seen.Mucosal resection was performed along the periphery of the lesion;B:Wound map after mucosa stripping.
Single-factor analysis of ESD operation time
The results of the single-factor analysis were shown in Table 1.Patients with maximum lesion diameter ≥ 3.00 cm had longer ESD operation time than patients with lesion diameter < 3.00 cm.The operation time of ESD in patients with different lesions was different,mixed type > concave type > flat type > uplift type.The operation time of patients with ulcers or scars was longer than those of patients without ulcers.Patients with perforation were longer than those without perforation.Patients with perforations had a longer duration of disease than those without.Lesions infiltrated into the submucosa more frequently than into the mucosa alone.And the differences were all statistically significant(P< 0.05).
Multivariate analysis of ESD operation time
The ESD operation time(min)was taken as the dependent variable Y,and the variables with statistical significance in single factor analysis were taken as independent variables Xi.The multiple linear regression model was fitted by a stepwise method.The goodness of fit of the multiple linear regression model reached a large effect(r= 0.692).The model finally adjustsR2was 0.563.The variance analysis results of the model showed that the F value was 54.866,and thePvalue was < 0.001.The regression equation was as follows:In = 21.674 + 8.815 × 1 + 3.766 × 2 + 10.247 × 3 + 4.417 × 4 + 3.692 × 5 + 2.536 × 6.When other factors remain unchanged,the maximum diameter of the lesion can affect the ESD operation time by 8.815%.If the lesion was concave or mixed,the operation time increased by 3.766% or 10.247%.If combined with an ulcer or scar,ESD operation time increased by 4.417%.The operation time increased by 3.692% if combined with perforation.If infiltrated into the submucosa,it increased by 2.536%(Table 2).
Single-factor analysis of delayed hemorrhage after ESD
The subjects were divided into a bleeding group and a non-bleeding group according to whether postoperative delayed hemorrhage occurred.The results of the single-factor analysis were shown in Table 3.Patients with hypertension,a history of taking anticoagulant or antiplatelet drugs,maximum lesion diameter,lesion morphology,and ESD operation time were associated with postoperative delayed hemorrhage(P< 0.05).Gender,age,other underlying diseases except for hypertension,location of lesion,ulcer or scar,perforation,and depth of infiltration were not associated with delayed hemorrhage after the operation(P> 0.05).
Multivariate analysis of delayed hemorrhage after ESD
Taking the occurrence or not of delayed hemorrhage after ESD as the dependent variable,and the factors with statistical significance in single factor analysis as independent variables,the multivariate logistic regression model was fitted.As shown in Table 4.The maximum diameter of lesions,lesion morphology,and ESD operation time were independent factors for delayed hemorrhage after ESD.Patients with lesions ≥ 3.0 cm(OR = 3.785,95%CI:1.165-4.277),lesion morphology-concave type(OR = 10.985,95%CI:2.133-35.381),and ESD operation time ≥ 60 min(OR = 2.958,95%CI:1.117-3.526)were prone to delayed hemorrhage after ESD.
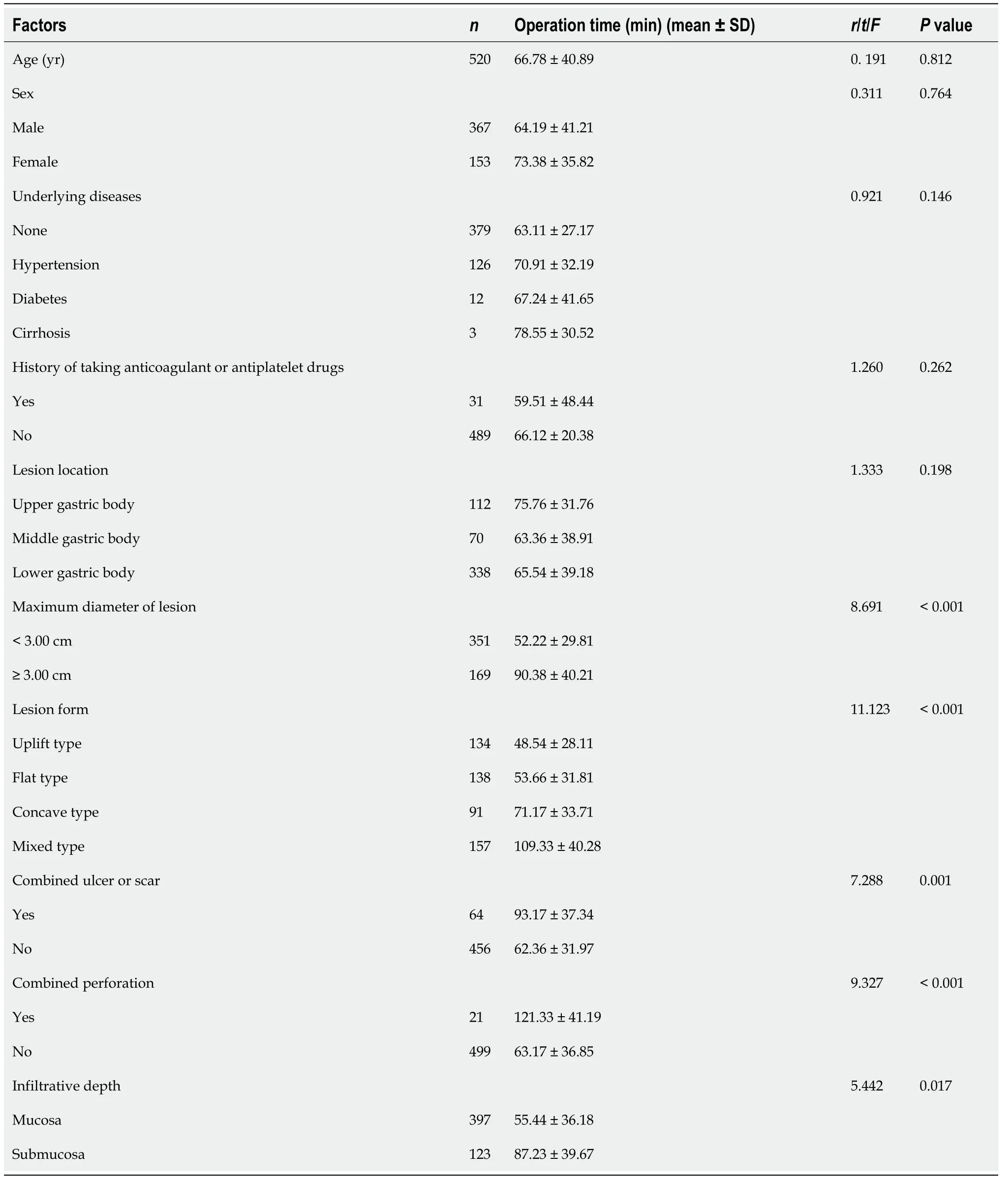
Table 1 Single-factor analysis of endoscopic submucosal dissection operation time
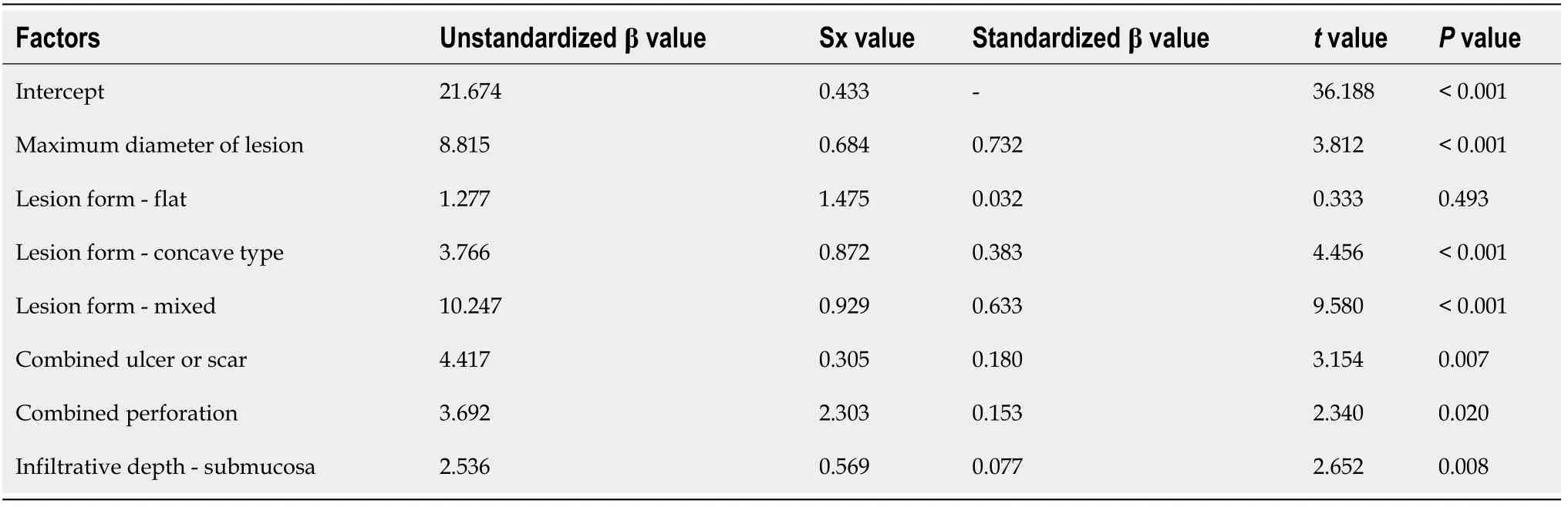
Table 2 lndigenous test results of multivariate linear regression independent variables
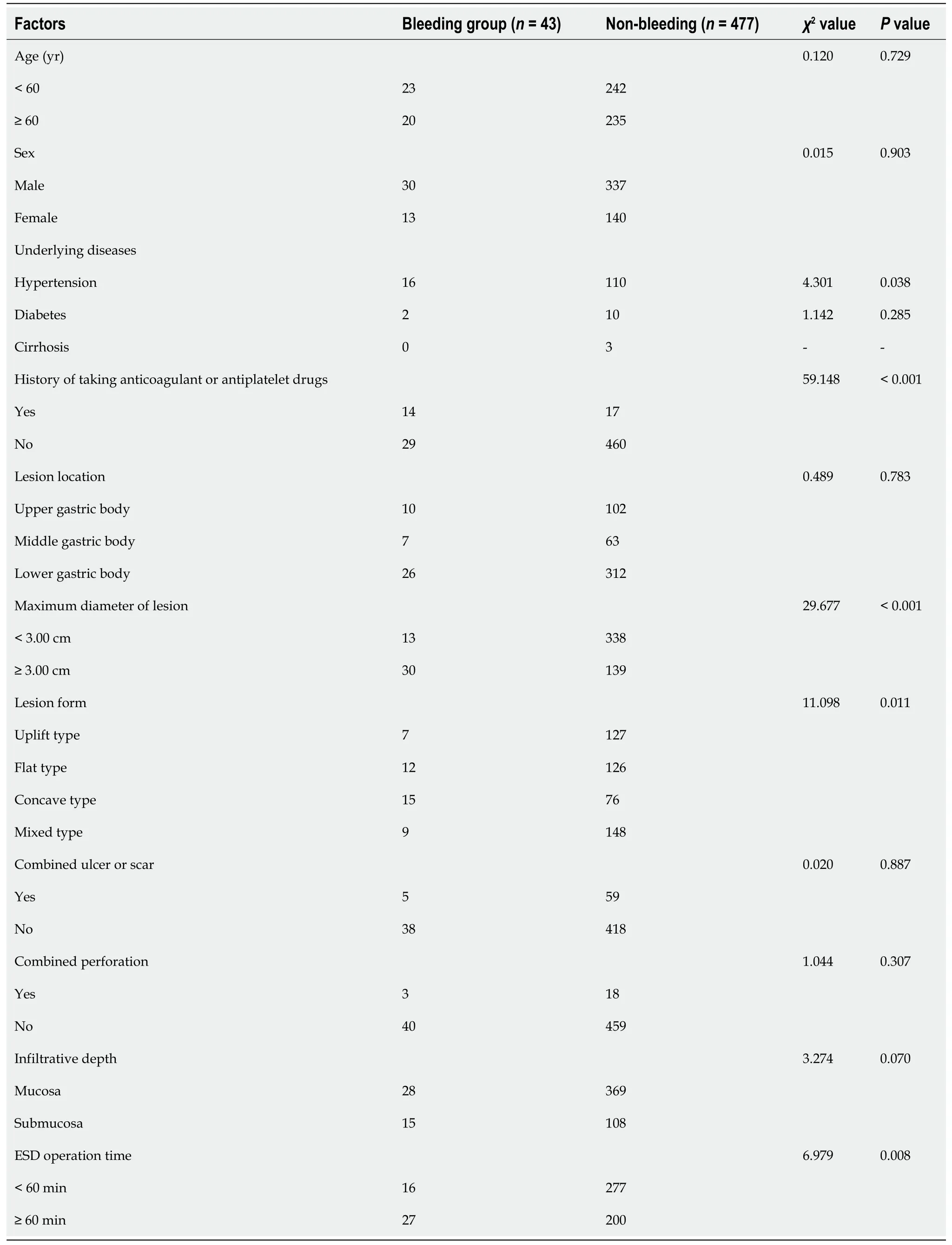
Table 3 Single-factor analysis of the bleeding group and non-bleeding group
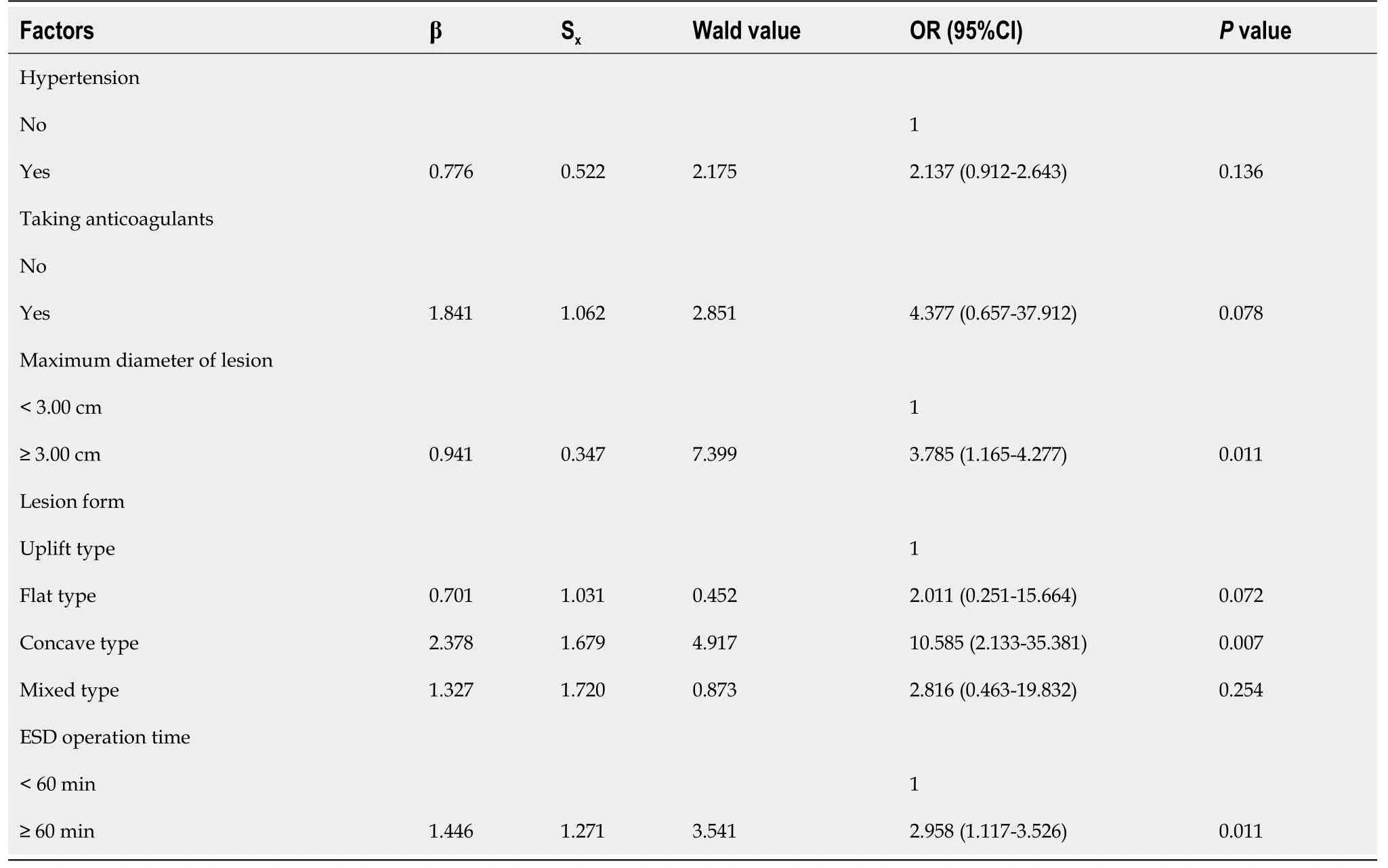
Table 4 Logistic regression analysis of delayed hemorrhage after endoscopic submucosal dissection
DlSCUSSlON
In the past,surgical resection is the standard treatment for early gastric cancer.However,conventional surgery has the disadvantages of large invasion,more postoperative complications,and longer recovery time[8].Compared to surgical resection,ESD has the advantage of small invasion,more tolerable for patients.And it also can be used as multiple surgical treatments for the same patient or multiple parts of treatment at the same time.Moreover,it has been recognized by experts all over the world and has been used as the first-line treatment for early gastric cancer[9,10].The amount of time for an ESD is one of the best indicators to measure the difficulty of surgical operation.And IT is very beneficial for the operation plan arrangement and complications prevention if the difficulty and operation time could be predicted in advance.In previous studies,the multivariate analysis suggested that tumor location and size wereimportant predictors of operation time[11,12].The operation difficulty of different positions of the gastric cavity varies greatly,which will affect the operation time of ESD[13].In this study,the same equipment and the ESD operation method were used by the same surgeon,which means the influence of different equipment on ESD operation time was excluded.Single-factor and multi-factor analyses were conducted after excluding the above-mixed factors.We found that the maximum diameter of the lesion,lesion morphology,ulcer or scar,perforation,and depth of invasion were independent factors affecting the ESD operation time.Previous studies found that intraoperative perforation was an independent predictor of prolonged ESD operation time[14,15].Our research also has similar conclusions.In ESD,small perforations can be treated under endoscopy,and the operation time will be prolonged due to the need for metal clips to seal the wound[16].Longer operation time can increase the risks of complications[17].Therefore,shortening ESD operation time can reduce intraoperative and postoperative complications of ESD[18].Thus,the prediction of operative time is crucial for both patients and surgeons.First of all,if we can predict if it will be a longer operation time,we can arrange for senior experts to complete difficult and long-term surgery,and shorten the operation time.Secondly,according to the length of the operation time,anesthesiologists can also use different anesthesia methods.Finally,the prediction of operation time can help operators to take corresponding measures to prevent complications in time,such as venous thrombosis,intraoperative aspiration,or postoperative pneumonia.However,the ESD operation technique is difficult,and the incidence of complications such as bleeding and perforation is high[19].Usually,intraoperative bleeding and perforation can be treated immediately.But delayed bleeding can lead to severe consequences such as hemorrhagic shock if it is found and treated not timely[20].Generally,artificial ulcers formed by ESD turn into fibrosis and thicken the gastric wall around 2 wk after surgery,and the healing takes about 8 wk[21].Some studies have shown that about 1/4 of the artificial ulcers appear as visible blood vessels on the 3rdday after ESD,and these broken blood vessels may be one of the main reasons for postoperative delayed bleeding[22].
Among the 520 patients in this study,there were 43(8.27%)patients with postoperative delayed bleeding,which was aligned with other literature.Takeuchiet al[23]retrospectively analyzed the data of 833 patients with early gastric cancer and precancerous lesions treated with ESD.and found that the longer duration of ESD in gastric cancer patients was an important risk factor for postoperativebleeding.Previous studies have shown that the lesion size after ESD is the only risk factor for delayed bleeding[24,25].Resection of large lesions can cause more damage to gastric wall blood vessels,and the risk of postoperative bleeding is higher.The results of this study further confirmed the conclusion that alesion ≥ 3 cm was more likely to postoperative bleeding.This suggests that endoscopic surgeons need to control the resection area as much as possible during the operation to avoid more gastric mucosal damage.We used magnifying and narrow-band imaging electronic chromoendoscopy to accurately determine the lesion boundary before surgery,and then accurately remove the lesion,which well controlled the operational area of surgical resection.
Previous studies have shown that flat lesions and concave lesions are associated with delayed bleeding after ESD.The results of this study suggested that concave lesions were more likely to have postoperative delayed bleeding(P= 0.007).This result can be explained by the following reasons.Firstly,compared with the uplift lesions,the concave lesions were closer to the muscular layer,and inappropriate biopsy can cause submucosa fibrosis easily,which leads to the increased probability of intraoperative bleeding.Furthermore,the submucosal vessels of flat lesions were richer than those of uplift lesions,thus,the risk of postoperative bleeding was higher.Long operation time is usually associated with frequent dissection and unskilled operation.Unskilled operation and repeated dissection often lead to vascular injury in the lower gastric mucosa and muscularis propria,which is easy to cause early postoperative delayed bleeding.Large lesions and deep infiltration,combined with perforation,can increase the difficulty of mucosal dissection and operation time and therefore easily damage blood vessels.Taking anticoagulant or antiplatelet drugs can inhabit ulcer-induced proliferation of gastric epithelial cells,thereby inhibiting angiogenesis during gastric ulcer healing,resulting in delayed bleeding more likely after ESD.It has been shown to be an independent risk factor for delayed bleeding after early and late ESD[26,27].Studies have found that antithrombotic drugs are independent risk factors for bleeding after ES[25].However,there was no significant difference in the distribution of aspirin administration history between the bleeding group and the non-bleeding group in this study.This may be the following reasons:Patients were required to discontinue anticoagulant drugs for one week before ESD or replace other drugs under the guidance of cardiovascular physicians.Patients with severe cardiovascular diseases were not treated in the department,so there was a selection bias in this study.It may also be related to the small sample size.This study was a single-center retrospective analysis with limited sample size and possible bias that was difficult to eliminate.
CONCLUSlON
In summary,patients with early gastric cancer with a maximum lesion diameter ≥ 3.0 cm,concave morphology,associated ulceration or scarring,combined perforation,and infiltration into the submucosa had a longer ESD operation time.Most importantly,the risk of delayed bleeding after ESD is higher when the maximum diameter of the lesion is ≥ 3.0 cm,the lesion morphology is concave,and the ESD operation time is longer.Therefore,we suggest that such patients should be treated with caution.Before the operation,the risk should be fully assessed.During the operation,the bleeding should be strictly controlled and the wound should be properly handled.The operation should also be carried out by experienced physicians.Finally,close observation also should be performed after the operation.
ARTlCLE HlGHLlGHTS
Research background
Endoscopic submucosal dissection(ESD)has become a new development trend in the treatment of early gastric cancer due to its special minimally invasive advantages.Although it is minimally invasive surgery,it also has some risks such as bleeding and perforation.
Research motivation
The time of ESD operation is closely related to bleeding and perforation.
Research objectives
This study aims to investigate the operation time of endoscopic subspecific section and the influencing factors of delayed bleeding after operation.
Research methods
The baseline data,clinical features,and endoscopic and pathological characteristics of patients were collected.The multivariate linear regression model was used to investigate the influencing factors of ESD operation time.Logistic regression analysis was carried out to evaluate the influencing factors of postoperative delayed hemorrhage.
Research results
The maximum diameter of the lesion,lesion morphology,and ESD operation time were independent influencing factors for delayed hemorrhage after ESD.Patients with lesion ≥ 3.0 cm(OR = 3.785,95%CI:1.165-4.277),lesion morphology-concave(OR = 10.985,95%CI:2.133-35.381),and ESD operation time ≥60 min(OR = 2.958,95%CI:1.117-3.526)were prone to delayed hemorrhage after ESD.
Research conclusions
The risk of delayed bleeding after ESD is higher when the maximum diameter of the lesion is ≥ 3.0 cm,the lesion morphology is concave,and the ESD operation time is longer.
Research perspectives
Further research should be made on other factors related to delayed bleeding after ESD operation,such as factors during operation and individual related factors.Strict control of surgical indications and adherence to individualized treatment can help reduce the occurrence of complications.
FOOTNOTES
Author contributions:Cai RS designed this study,analyzed the data and drafted the manuscript;Yang WZ and Cui GR collected the data and reviewed the manuscript critically;all authors have read and approved the final manuscript version.
lnstitutional review board statement:The study was reviewed and approved by Ethics Committee of the Second Affiliated Hospital of Hainan Medical University.
lnformed consent statement:The data used in this study were not involved in the patients’ privacy information,so the informed consent was waived by the Ethics Committee of Second Affiliated Hospital of Hainan Medical University.All patient data obtained,recorded,and managed only used for this study,and all patient information are strictly confidential,without any harm to the patient.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
Data sharing statement:No additional data are available.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See:https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Ren-Song Cai 0000-0002-5442-8657.
S-Editor:Gong ZM
L-Editor:A
P-Editor:Gong ZM
 World Journal of Gastrointestinal Surgery2023年1期
World Journal of Gastrointestinal Surgery2023年1期
- World Journal of Gastrointestinal Surgery的其它文章
- lntestinal erosion caused by meshoma displacement:A case report
- Short-term efficacy assessment of transarterial chemoembolization combined with radioactive iodine therapy in primary hepatocellular carcinoma
- Effects of postoperative use of proton pump inhibitors on gastrointestinal bleeding after endoscopic variceal treatment during hospitalization
- lmpact of body mass index in elderly patients treated with laparoscopic liver resection for hepatocellular carcinoma
- New perspectives on robotic pancreaticoduodenectomy:An analysis of the National Cancer Database
- Development and validation of a novel nomogram for predicting overall survival in gastric cancer based on inflammatory markers