
Postoperative adjuvant therapy for hepatocellular carcinoma with microvascular invasion
2023-03-17 07:45:46JiangLiFanYangJianLiZhiYongHuangQiChengErLeiZhang
Jiang Li,Fan Yang,Jian Li,Zhi-Yong Huang,Qi Cheng,Er-Lei Zhang
Jiang Li,Jian Li,Zhi-Yong Huang,Qi Cheng,Er-Lei Zhang,Hepatic Surgery Center,Tongji Hospital,Tongji Medical College,Huazhong University of Science and Technology,Wuhan 430030,Hubei Province,China
Jiang Li,Department of Hepatobiliary and Pancreatic Surgery,The First Affiliated Hospital,College of Medicine,Shihezi University,Shihezi 832000,Xinjiang Uygur Autonomous Regions,China
Fan Yang,Department of General Surgery,Affiliated Hospital of Hubei Minzu University,Enshi 445000,Hubei Province,China
Abstract Hepatocellular carcinoma(HCC)is one of the most lethal tumors in the world.Liver resection(LR)and liver transplantation(LT)are widely considered as radical treatments for early HCC.However,the recurrence rates after curative treatment are still high and overall survival is unsatisfactory.Microvascular invasion(MVI)is considered to be one of the important prognostic factors affecting postoperative recurrence and long-term survival.Unfortunately,whether HCC patients with MVI should receive postoperative adjuvant therapy remains unknown.In this review,we summarize the therapeutic effects of transcatheter arterial chemoembolization,hepatic arterial infusion chemotherapy,tyrosine protein kinase inhibitor-based targeted therapy,and immune checkpoint inhibitors in patients with MVI after LR or LT,aiming to provide a reference for the best adjuvant treatment strategy for HCC patients with MVI after LT or LR.
Key Words:Microvascular invasion;Hepatocellular carcinoma;Liver resection;Liver transplantation;Postoperative;Adjuvant treatment
lNTRODUCTlON
Hepatocellular carcinoma(HCC)is the seventh most common cancer and the second leading cause of cancer-related deaths in the world,with unsatisfactory long-term outcomes[1].Nowadays,hepatectomy liver resection(LR)and liver transplantation(LT)are still the most efficient strategies for HCC with relatively preserved liver function[2].Unfortunately,the surgical resection rate of HCC is still low in clinical practice due to untimely diagnosis and delayed treatment in most HCC patients.Even with radical surgery,the 5-year recurrence rate is still 70%-80%[3].Accordingly,decreasing the recurrence rate after surgical resection is of utmost importance to improve the clinical outcomes for early-stage HCC patients.
Various risk factors are associated with the recurrence of HCC.Malignant biological characteristics of the tumor and the condition of the underlying liver disease,such as hepatitis and liver cirrhosis,were found to be more significant prognostic factors than tumor size and warrant closer attention in clinical practice[4].Among malignant biological characteristics of HCC,microvascular invasion(MVI)is considered a risk factor for intrahepatic microscopic metastatic disease and one of the crucial factors for early HCC recurrence after LR or LT.As a consequence,In the 8thedition of the American Joint Committee on Cancer staging system,it was further included as an important prognostic factor,where it is considered an independent risk factor for poor clinical outcomes[5].Currently,MVI is usually defined as tumor cells invading into the portal vein,hepatic vein,or a large capsular vessel of the surrounding tumor tissues,partially or totally lined by endothelial cells visible only by microscopical examination of specimens obtained from surgical excision,which is acknowledged as a histological feature[6].MVI plays a crucial role in the selection of surgical modalities and also a vital indicator of early tumor recurrence in HCC patients[7].Due to differences of MVI status,the surgical outcomes are likely inconsistent among different treatment groups.The presence of MVI in HCC is strongly correlated with the recurrence rates after surgical resection and should be classified as locally advanced-stage biological behavior[7,8].Moreover,time to recurrence after curative surgical resection is a critical prognostic factor for clinical outcomes,as early tumor recurrence is associated with worse overall survival(OS).Therefore,postoperative adjuvant treatments may be partly beneficial to decrease the tumor recurrence rates in HCC patients with MVI.Unfortunately,there is still no consensus on the optimal adjuvant treatment after LR or LT for HCC with MVI.
Advances in systemic therapy for advanced HCC,as well as promising strategies for perioperative management of LR,have led to a substantial improvement of surgical outcomes in recent years.Transcatheter arterial chemoembolization(TACE),hepatic arterial infusion chemotherapy(HAIC),as well as targeted therapies based on tyrosine kinase inhibitors(TKIs)or immune checkpoint inhibitors(ICIs),are the current state-of-the-art strategies,which have shown great promise in the treatment of advanced HCC[8-12].However,whether TACE/HAIC,TKIs(such as sorafenib and lenvatinib),and ICIs[such as programmed cell death protein 1(PD-1)/programmed death ligand 1(PD-L1)inhibitors]are beneficial for decreasing tumor recurrence rates in HCC patients with MVI remains controversial.In view of this,results derived from all the studies were analyzed,aiming to outline the optimal treatment strategy for HCC with MVI after LR.For patients with early-stage HCC,LR,LT,and local ablation(LA)are considered as first-line treatments.However,MVI cannot be precisely evaluated in HCC patients who underwent LA.Therefore,we mainly discuss the effect of postoperative treatments on the surgical outcomes after LT and LR.This review article aims to provide updated information on the recent developments in postoperative adjuvant therapy in HCC patients with MVI.
LR
MVI has been widely identified as a crucial risk factor for intrahepatic recurrence after R0 surgical resection,which was evidenced by increased local recurrence rates and reduced recurrence-free survival(RFS)after LR compared to HCC patients without MVI.Whether postoperative adjuvant therapy could improve the surgical outcomes for HCC with MVI remains unclear.There is an urgent need to discuss several postoperative adjuvant treatments such as TACE/HAIC and TKI and ICI therapy,aiming to shed a new light on ways to improve the prognosis for such HCC patients.
TACE
The main purpose of TACE after LR is to eliminate the tumor cells released due to compression during operation and destroy the existing microscopic foci in the remnant liver that cannot be found by preoperative imaging examination.It delivers specific drugs,along with iodized oil,mainly to suspected tumor areas,followed by embolization to cause tumor cell necrosis and prevent residual lesions from growing into clinically visible tumors.Some studies demonstrated a superior effect of postoperative TACE in terms of OS and RFS[13,14],while other studies reported comparable results with or without postoperative TACE[15,16].The benefits of adjuvant TACE in HCC patients with MVI remain controversial.A meta-analysis indicted that adjuvant TACE plus LR may improve the surgical outcomes of HCC patients with MVI compared to LR alone and should be recommended for HCC patients with MVI[17].Another meta-analysis showed that postoperative adjuvant HAIC could improve the long-term prognosis of HCC patients,especially those with microvascular or macrovascular invasion[18].A retrospective study showed that postoperative HAIC offers better OS than simple surgical resection in patients with MVI[19].The beneficial effect of postoperative adjuvant TACE may be related to a number of factors.First,the poor efficacy of surgical resection in patients with liver cancer complicated with MVI is due to the micrometastasis of residual cancer cells before or during LR[20,21].Postoperative adjuvant TACE can kill or ablate these cells and improve the prognosis.Second,patients with MVI are prone to micrometastasis before surgery[22,23].Therefore,TACE is a suitable and effective treatment 3-4 wk after LR,when the patients recover from surgery and the residual tumor is still small.Third,the majority of HCC blood supply comes from the hepatic artery,and recurrent tumors often occur near the edge of LR[24,25].The use of postoperative adjuvant TACE increases the concentration of these marginal local anticancer drugs,which may improve the prognosis of such patients.However,there is no uniform standard for drug combination,dose,frequency of TACE,and time interval of each treatment.Nevertheless,other studies showed conflicting results.A meta-analysis of randomized clinical trials(RCTs)found that TACE did not improve RFS and OS after radical resection of HCC unless the tumor size was 5 cm[26].A retrospective study showed that adjuvant HAIC using 5-fluorouracil and cisplatin did not improve disease-free survival(DFS)and OS after LR[27].It remains unclear if HCC patients with MVI can benefit from adjuvant TACE treatment after surgery.The effectiveness of TACE may be due to the fact that chemotherapy drugs enter the blood vessels,and thereby come in contact with the migrating tumor cells to destroy them.However,due to the different tumor microenvironment and tumor heterogeneity in different populations,some patients still cannot benefit from this treatment.The tumor microenvironment may play a key role in the initiation and maintenance of drug resistance through various mechanisms such as pH changes,hypoxia,vascular system abnormalities,changes in immune populations,and extracellular matrix[28].
The pro-tumor environment that induces immunosuppression,such as myeloid-derived suppressor cells,regulatory T cells,and tumor-associated macrophages in the liver immune cell population,may play a major role in the limited effectiveness of chemotherapy drugs.Moreover,chemotherapy drugs themselves may change the composition of the inflammatory cell population[29].In addition to the interaction of immune cells,hepatocirrhosis microenvironment composes a physical barrier that stimulates tumor growth by altering biomechanical properties,cytokine secretion,and activation of multiple signaling pathways,preventing drugs from reaching targets in the tumor parenchyma and thus reducing drug availability.
Moreover,high-dose TACE can damage liver cells,leading to the deterioration of liver function,reduced immunity against tumor cells,and increased risk of hepatitis B virus reactivation.In TACE,the combined use of multiple drugs may increase the burden on the liver leading to drug-induced liver injury,and ultimately adversely affect the therapeutic effect.Therefore,factors such as liver function and operation time should be considered in postoperative combined TACE treatment[19].In addition,tumor load,tumor invasion,and postoperative recovery may be factors affecting the efficacy.The relevant studies on the postoperative application of TACE or HAIC as adjuvant therapy are listed in Table 1.However,these results need to be further verified by high-quality RCTs.
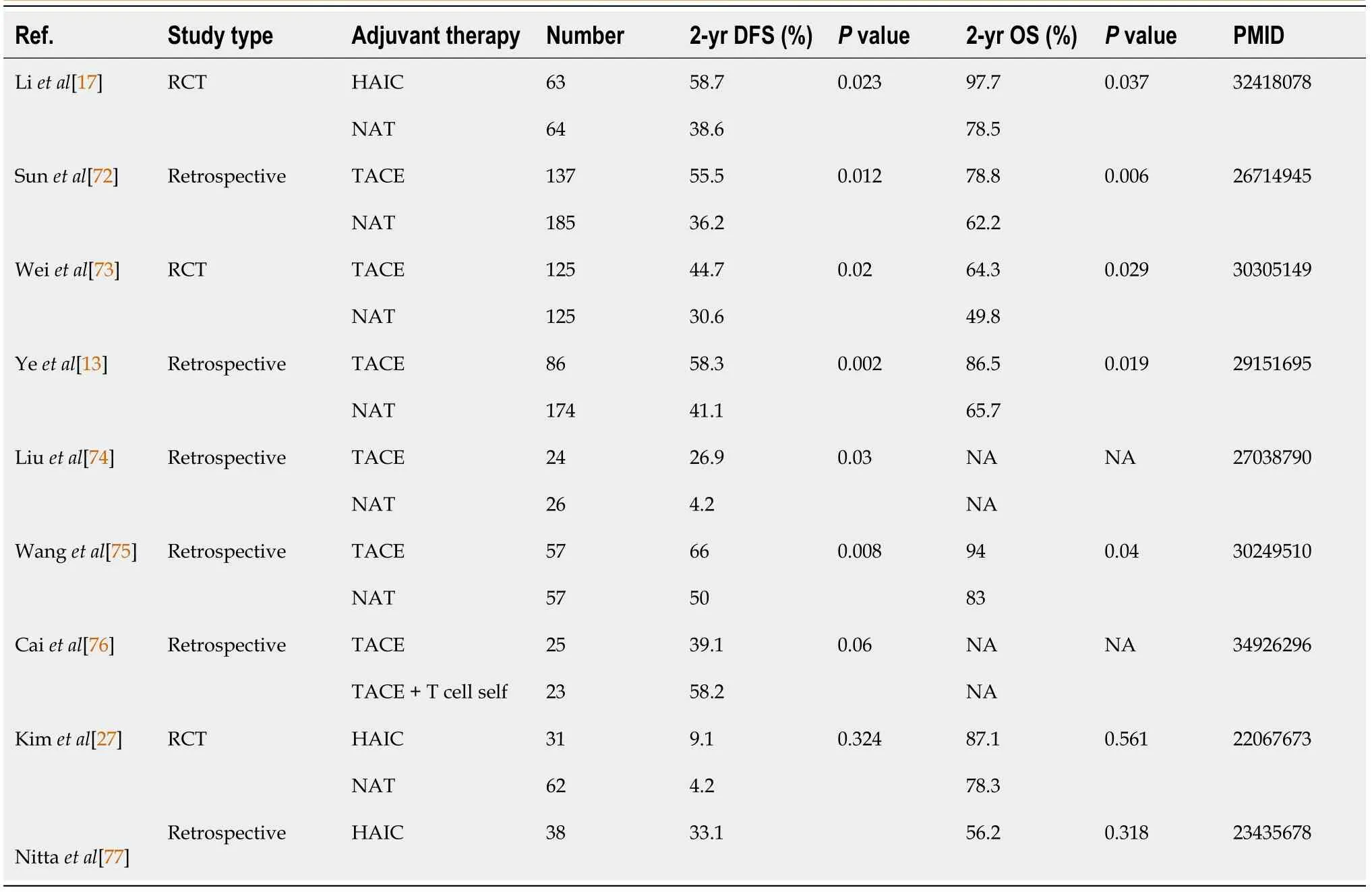
Table 1 Transcatheter arterial chemoembolization approved as an adjuvant therapy for hepatocellular carcinoma patients with microvascular invasion
Target therapy-TKIs
Intrahepatic tumor recurrence after LR can be divided into early recurrence and late recurrence.Early recurrence is related to intrahepatic metastasis of primary tumors that cannot be detected clinically,which may be related to the spread and metastasis of tumor cells in portal vein circulation caused by the shedding of cancer cells before surgery or the pressure exerted on tumors during LR.As liver cancercells gradually infiltrate the tumor capsule surrounding matrix,and vascular wall,they further invade blood vessels to form MVI.The multi-kinase inhibitors that target tumor cells and tumor blood vessels act on a variety of kinases and pro-angiogenic receptors,blocking downstream signaling pathways,inhibiting the proliferation and promoting apoptosis of tumor cells,as well as inhibiting tumor cell angiogenesis,and migration,with a wide range of anti-tumor effects that promote the prevention and treatment of tumor recurrence[30].
Sorafenib is a multi-kinase inhibitor that blocks multiple molecular pathways through its antiangiogenic and anti-proliferative effects.A RCT revealed that sorafenib could effectively improve the survival time with advanced HCC patients[31].In addition,sorafenib has been reported to inhibit postoperative intrahepatic recurrence and abdominal metastasis,thereby extending postoperative survival time[32,33].
Sorafenib can improve the prognosis of MVI in HCC patients after R0 LR.A meta-analysis investigated the preventive effect of sorafenib against tumor recurrence in HCC with MVI,and the results showed that LR plus sorafenib significantly improves the prognosis of HCC with MVI compared to LR alone.However,this meta-analysis has some shortcomings.First,it only included retrospective studies,which may cause selection bias.Second,the patients in these four studies were all Chinese,which also weakens the universality of the conclusion[34].
Recent studies have demonstrated the efficacy of sorafenib in preventing recurrence of HCC after LR[35].Liet al[36]as well as Xiaet al[37]found that the OS and DFS of Barcelona Clinic Liver Cancer stage C HCC patients treated with oral sorafenib after LR was significantly longer than those of patients only treated by LR.Wanget al[38]proved that sorafenib as an adjuvant therapy for HCC can prevent early recurrence after LR.Huanget al[39]evaluated the impact of sorafenib as an adjuvant therapy on the clinical outcomes in HCC with MVI.The results indicated that adjuvant sorafenib significantly prolonged both OS and RFS of patients with HCC after radical resection.
However,a RCT revealed that sorafenib treatment after LR did not improve the DFS of HCC patients,but increased the incidence of side effects,such as hand-foot skin reaction,diarrhea,and fatigue[40].Similarly,it was found that postoperative sorafenib adjuvant therapy cannot improve RFS in HCC patients with MVI[41].The relevant studies on postoperative application of TKIs as adjuvant therapy are listed in Table 2.There are differences in the results from different centers.In addition to the sample size and research methods that may affect the results,these differences may also be caused by differentdefinitions and classifications of MVI.It may be necessary to conduct systematic research under uniform definitions and standards to make the results more comparable.
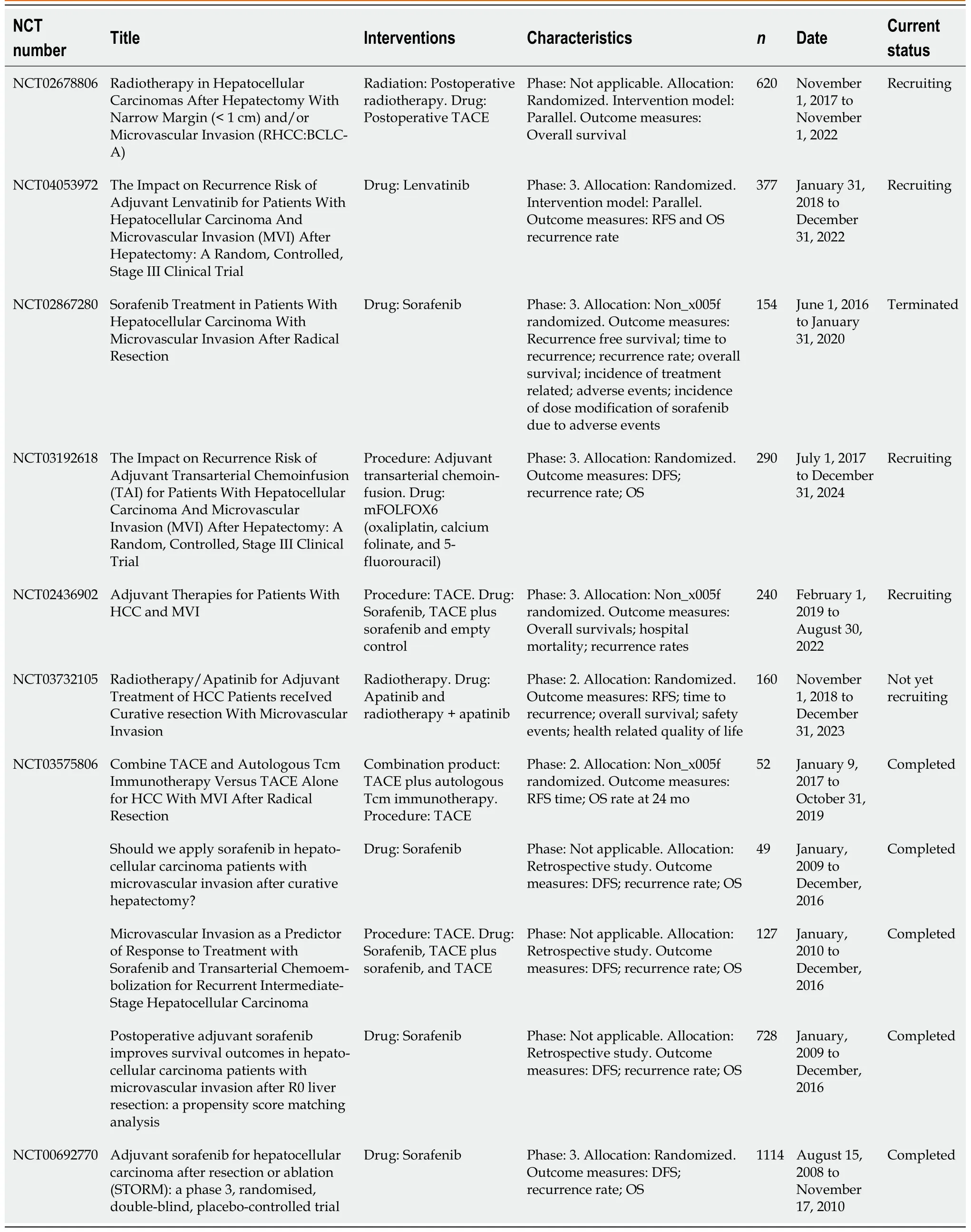
Table 2 Tyrosine kinase inhibitor approved as an adjuvant therapy for hepatocellular carcinoma patients with microvascular invasion
Although targeted drugs have greatly improved the prognosis of patients with advanced liver cancer,the efficacy of single drugs is still limited,and drug resistance may occur during treatment due to tumor heterogeneity and changes in the immune microenvironment.In addition,the side effects of drugs and the tolerance of patients also affect the therapeutic effect.In the future,it may be necessary to standardize the population suitable for targeted therapy,and consider combined therapy to improve the efficacy when single drugs are insufficient.In view of the above results,the role of targeted drugs as adjuvant therapy may still be controversial,and a large number of prospective RCTs are needed to further verify their efficacy in the future.
PD-1/PD-L1 treatment
ICIs are a new class of anti-tumor drugs that target regulatory signals between T cells,target cells,and other immune cells.T cells can recognize specific antigens presented on target cells by major histocompatibility complex proteins through their T cell receptors,and can induce apoptosis of target cells.T-cell activity is precisely regulated by co-stimulatory and co-inhibitory molecules to maintain an appropriate immune response without harmful overactivation.Therefore,adjuvant application of ICI after LR,may activate T cells to destroy circulating tumor cells and prevent recurrence.
At present,the main immune checkpoint molecules targeted by immunotherapy are PD-1,PD-L1,and cytotoxic T lymphocyte-associated protein 4.Cancer immunotherapy may have a significant impact in adjuvant settings,as it can immediately induce tumor cell killing and potentially produce durable immune responses that eliminate residual micrometastases that are thought to lead to early recurrence.Anti-PD-1/PD-L1 antibody,either alone or in combination,has shown successful induction of pathological reactions in a variety of tumor types,while also inducing tumor-specific T cell amplification,which may produce a vaccine effect capable of systemic monitoring[42,43].The response rate to PD-1 blockade is about 20%,and the response to combined therapy may be higher[44,45].
At present,no large-scale clinical datasets have confirmed the role of ICIs in preventing postoperative recurrence and improving long-term survival in HCC.CheckMate-9DX is an ongoing trial investigating whether nivolumab can improve RFS compared with placebo in HCC patients who have a high risk of recurrence after LR or ablation,which includes patients with MVI.
Prevention of postoperative recurrence is an important part of the treatment of HCC,which is still an unsolved clinical problem.For early operable HCC with MVI,optimal liver function reserve,good physical condition,and increased tolerance to immune-related toxicity may improve the curative opportunity of the patients.However,the response of such patients to immunotherapy or drug resistance is still a challenge that cannot be ignored.
Considering the potential adverse reactions to combined administration,it is particularly important to select specific patients that most likely benefit from such therapies.Therefore,it is necessary to establish an effective predictive model,and a large number of prospective clinical studies are still needed to provide reliable guidance.In addition,there are studies on targeted drugs combined with immunotherapy for postoperative assistance,as shown in Table 3.We expect these effective research results to provide a reference for clinical decision-making.Since MVI is one of the critically important risk factors for relapse and metastasis,surgical resection alone may not completely eliminate the adverse effects of MVI and improve the prognosis of patients.Although there is no uniform standard for adjuvant therapy after LR,it may be one of the most promising strategies to improve the efficacy HCC therapy in patients with MVI.
LT
LT is suitable for patients with early HCC[46],but unfortunately,many patients are diagnosed at an advanced stage.Although many centers have expanded the indications beyond the Milan criteria and achieved promising results,there is still a high risk of relapse after transplantation,with HCC recurrence peaking about 2-3 years after LT[47-50].
Theoretically,LT completely eliminates tumors and potential lesions in the liver.However,MVI or undetected extrahepatic lesions can lead to HCC recurrence after transplantation.MVI was reported to be a major risk factor for HCC recurrence after LT[51].Milan and other similar criteria are based on tumor size according to imaging,which does not provide sufficient information about pathological features and tumor biology,such as MVI and differentiation/grade.Therefore,these criteria cannot fully predict the recurrence of HCC after LT.MVI in the liver can predict tumor recurrence and indicate a poor prognosis.However,although MVI is an important predictor of tumor recurrence,without pathological examination,it is almost impossible to detect MVI before LT.Therefore,MVI largely determines the long-term prognosis of patients after resection and transplantation[52].Theoretically,adjuvant therapy after LT may eradicate residual tumor cells in the blood.Therefore,it is very important to explore adjuvant therapy to improve the survival rate after transplantation.
At present,there is no systematic adjuvant therapy for HCC patients with MVI after transplantation,and most of the related studies focused on the treatment of recurrence after transplantation.Only some studies investigated adjuvant treatments for patients with a high risk of recurrence after transplantationbeyond the Milan criteria.Nevertheless,patients with MVI were included in these studies,as summarized below and listed in Table 4.
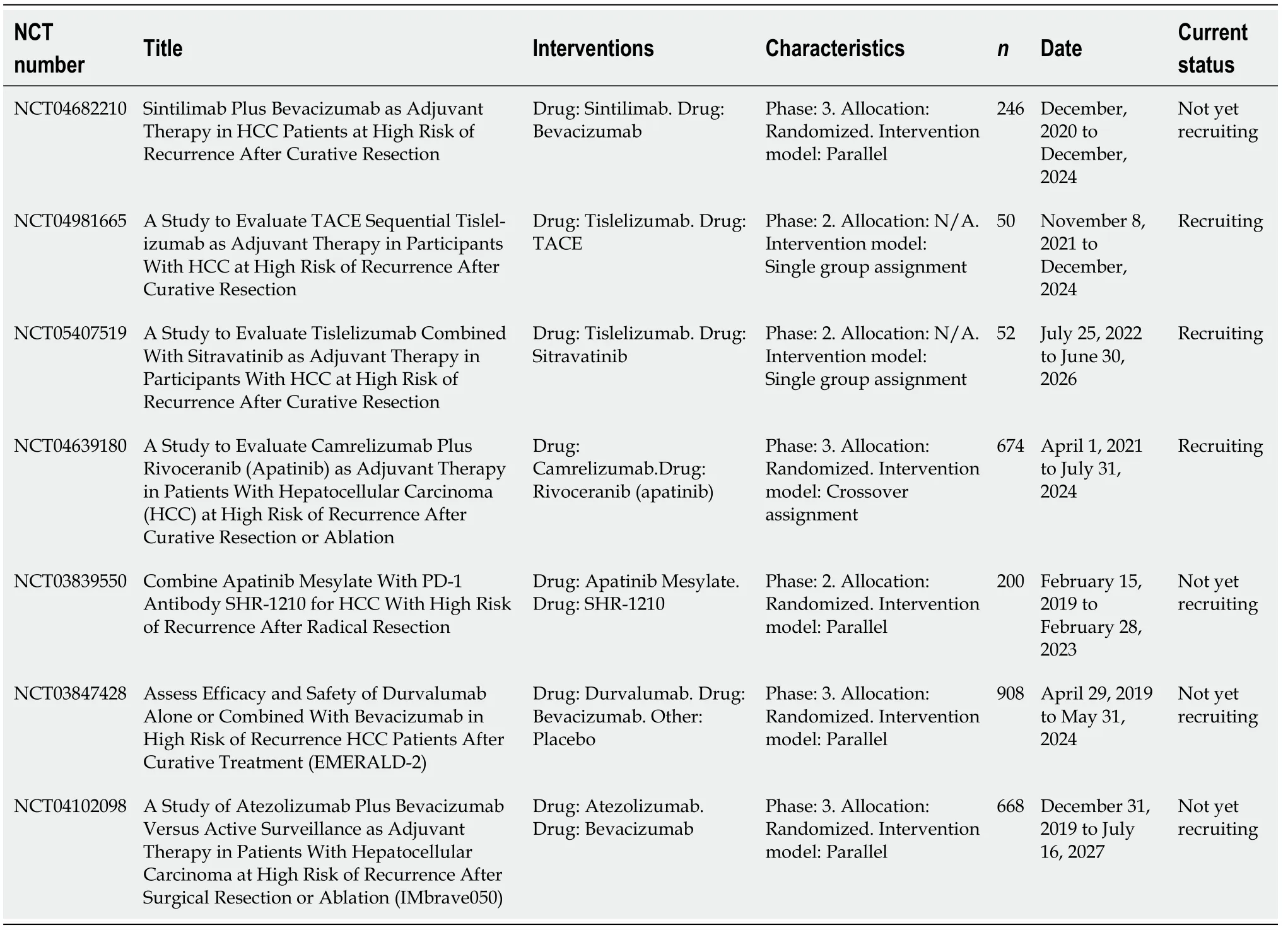
Table 3 lmmune checkpoint inhibitors as an adjuvant therapy for hepatocellular carcinoma patients with microvascular invasion
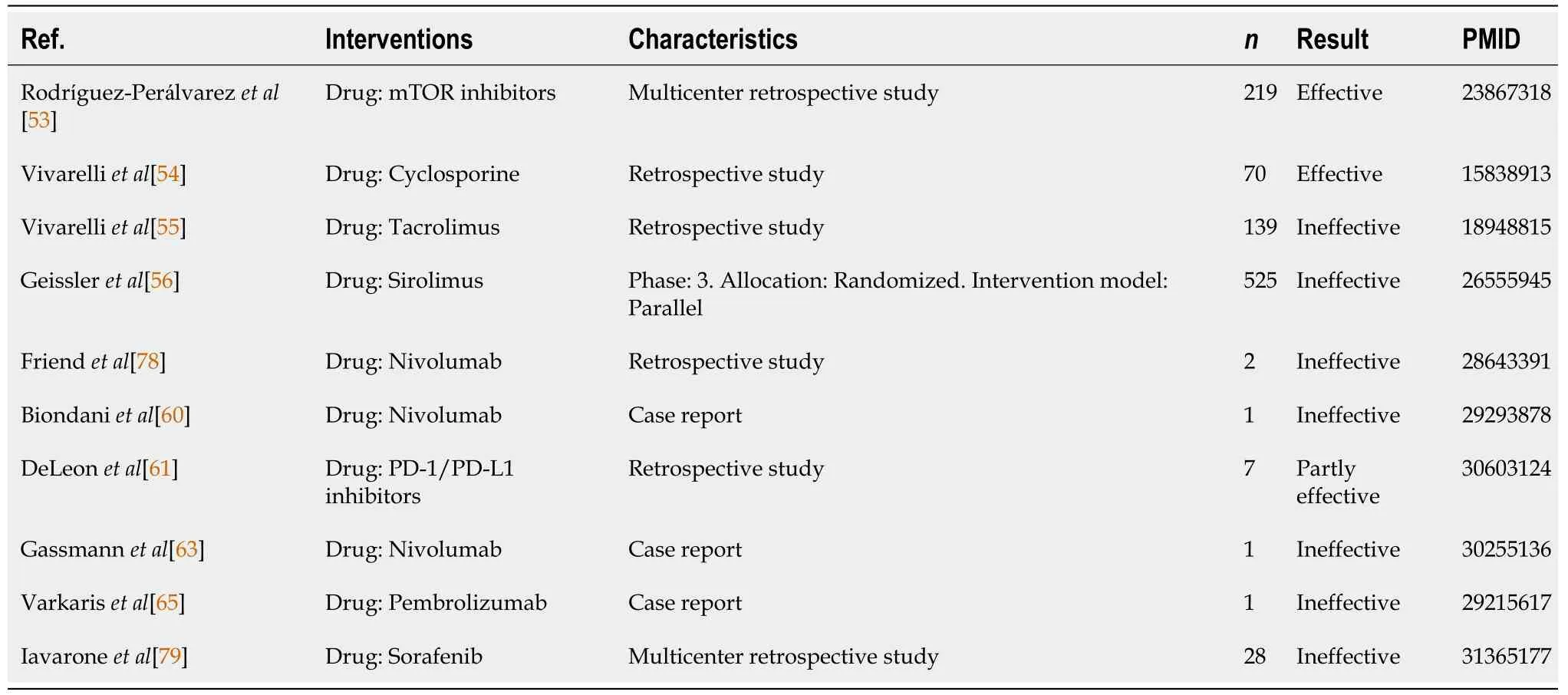
Table 4 Adjuvant therapy after liver transplantation
There is a high burden of early immunosuppression,especially in the case of calcineurin inhibitors such as cyclosporine and tacrolimus,which are usually the basic drugs against organ rejection after transplantation and may also increase the risk of HCC recurrence[53-55].By contrast,immunosuppressive regimens based on mammalian target of rapamycin inhibitors,such as sirolimus and everolimus,have antitumor propertiesin vitroandin vivoand may reduce the HCC recurrence rates.Unfortunately,a prospective phase III multicenter RCT showed no significant improvement of the recurrence rate in HCC transplant recipients treated with sirolimus[56].
Some small studies have shown that sorafenib can improve the survival rate of LT patients with a high risk of recurrence after transplantation[33],but there is also evidence against chemotherapy or sorafenib adjuvant therapy after LT[57].Whether targeted drugs are suitable for LT patients with MVI therefore remains to be verified in the future.Overall,there is no evidence that systemic adjuvant chemotherapy after LT can prevent HCC recurrence[58].
Although ICIs have demonstrated a certain level of efficacy in advanced liver cancer,based on the characteristics of ICIs and the special physical condition of patients after LT,balancing graft-protective immunosuppression and anti-tumor immune enhancement is still an unresolved issue.The use of ICIs as adjuvant therapy in transplant recipients has been the subject of several case reports[58-62],but ICIs may promote allograft injury[63],leading to severe rejection and even death.When systematically evaluating the data of cancer transplant recipients receiving ICIs,37.5% of the recipients experienced liver allograft rejection,resulting in a 75% incidence of end-stage organ failure[64].PD-1 inhibitor therapy after LT was reported in eight cases,including two cases of graft rejection[58,60,65].Even if the treatment strategy of combined ICIs has great prospects,clinicians should be extremely cautious in practical application.
Tumor cell invasion of microscopic blood vessels in the surrounding liver tissue adjacent to the tumor is a histological feature of HCC.In recent years,several studies have intended to classify MVI based on different features[66-68],indicating that MVI can be further classified as MI and microscopic portal vein invasion(MPVI)[69,70],where tumor cells may invade the microvessels at the initial stage of invasion,while the newly formed microvascular structure due to the interaction of liver tissue around the tumoris defined as MI.Subsequently,as tumor invasion accelerates,tumor cells float and settle in the portal vein branches farther away from the original tumor,which is defined as MPVI.Unfortunately,MVI can only be definitively diagnosed by examining surgical specimens,limiting its role in guiding individualized treatment.The two types of MVI have different foundations and mechanisms.MPVI is a more advanced form of tumor invasion than MI.Patients with MPVI have more aggressive tumor characteristics,and the two different risk factors for recurrence suggest that the goals should be different when designing adjuvant therapy for each type.For MI,the main strategy should be targeted at disseminated tumor cells that spread from the primary tumor[7].For MPVI,a potentially systemic treatment strategy is more appropriate.Our preliminary study indicated that postoperative adjuvant therapy could improve long-term outcomes after curative LR in HCC patients with MPVI,but the effect was weaker in MI.At the same time,our studies have shown that in MI,a wider surgical margin can eliminate peripheral intrahepatic micrometastasis,thereby preventing early tumor recurrence.By contrast,the surgical results of MPVI patients are similar regardless of the width of the surgical margin[71].
Therefore,it may not be wise to classify the two types of vascular invasion into one group for research and analysis,while more appropriate treatment strategies should be developed based on different biological and histological characteristics.Several limitations exist in this study.First,the prognosis of HCC is affected by a variety of factors including tumor markers,tumor size,tumor differentiation,and liver cancer staging,here,we only give a systematic review of the prognosis of patients with MVI,not considering other factors.Second,since adjuvant therapy after LT with MVI is relatively limited,the results obtained may not objectively reflect its efficacy.Third,we did not categorize all studies using meta-analysis,so there may still be valid treatment outcomes missed.Thus,more clinical studies may be needed to analyze the postoperative adjuvant therapy for such populations in order to obtain the best treatment strategy.
CONCLUSlON
Adjuvant therapy for preventing tumor recurrence after radical resection in HCC patients with MVI is the key to improving the long-term survival rate.Although there is still controversy,after LR,TACE may be an effective choice to improve DFS and OS.As targeted therapy and immunotherapy have been effective in improving the prognosis of patients with advanced liver cancer in many retrospective studies,adjuvant therapy based on molecular targeted drugs needs further study.Many RCT studies evaluating adjuvant ICI after LR are ongoing,and their results may provide additional references for adjuvant therapy.In the future,prospective studies should be carried out to clarify the improvement of prognosis in the MVI subgroup by these two treatments.Moreover,in consideration of the actual drug efficacy,adverse reactions,and patient tolerance,the relationship between efficacy and safety should be balanced in clinical practice.It may be necessary to distinguish potential populations benefiting from each combination therapy,and to assess whether patients have the preconditions to receive effective combination therapy using novel biomarkers and biological characteristics.
FOOTNOTES
Author contributions:Zhang EL and Cheng Q contributed to the study design,Zhang EL and Cheng Q as the cocorresponding author of this manuscript;Li J,Yang F,and Li J contributed to the collection of the data;Li J and Huang ZY contributed to the analysis and interpretation of the data and the writing of the article;Zhang EL contributed to the financial support;Cheng Q and Zhang EL contributed to the revision of the article and statistical analysis;and all authors read and approved the final version of the article.
Supported bythe National Natural Science Foundation of China,No.81902839.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See:https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Jiang Li 0000-0003-0120-9239;Jian Li 0000-0001-9025-4968;Zhi-Yong Huang 0000-0002-2239-0674;Qi Cheng 0000-0002-70696811;Er-Lei Zhang 0000-0002-7251-0275.
S-Editor:Wang JJ
L-Editor:Wang TQ
P-Editor:Wang JJ
 World Journal of Gastrointestinal Surgery2023年1期
World Journal of Gastrointestinal Surgery2023年1期
- World Journal of Gastrointestinal Surgery的其它文章
- lntestinal erosion caused by meshoma displacement:A case report
- Short-term efficacy assessment of transarterial chemoembolization combined with radioactive iodine therapy in primary hepatocellular carcinoma
- Associate factors for endoscopic submucosal dissection operation time and postoperative delayed hemorrhage of early gastric cancer
- Effects of postoperative use of proton pump inhibitors on gastrointestinal bleeding after endoscopic variceal treatment during hospitalization
- lmpact of body mass index in elderly patients treated with laparoscopic liver resection for hepatocellular carcinoma
- New perspectives on robotic pancreaticoduodenectomy:An analysis of the National Cancer Database