
Transcutaneous dorsal penile nerve stimulation for the treatment of premature ejaculation:A novel technique
2022-09-20 03:30:18
Asian Journal of Urology 2022年3期
Dear editor,
Premature ejaculation(PE)is a common male sexual dysfunction.It occurs in 4%-39% of men across studies in community samples[1].It is impossible to establish accurately the real prevalence of PE because it lacks a widely accepted definition.Furthermore,PE is frequently a self-reported,self-rated complaint,making it difficult to appreciate its real epidemiology.In addition,the fact that in some couples PE is diagnosed based on distress rather than as an objective symptom complicates the matter even further[2].Oral dapoxetine has been recommended as first-choice therapy for PE.When using this drug,side effects were uncommon,dose-dependent,including nausea,diarrhea,headache,and dizziness[1].Although since the early 1930s,many drugs have been used to treat PE such as topical local anesthetics and selective serotonin reuptake inhibitors.There are currently only two drugs that have been recommended to manage lifelong and acquired PE,the on-demand,oral drug dapoxetine and the topical lidocaine or prilocaine spray(anesthetic)[3].As treatment with fewer side effects and lower cost,behavioral therapy aims to improve self-confidence and relieve anxiety and depression by continuously training men to master certain sexual skills to delay ejaculation time.Studies have shown that the short-term effect of behavioral therapy can reach 45% to 65%,but the long-term effect is still unclear[4].
Ejaculation comprises two distinct phases:the emission and expulsion phases.Emission phase consists of the secretion of multiple components of sperm into the urethra.The expulsion phase consists of sperm release by rhythmic contraction of multiple perineal muscles such as the bulbospongiosus and ischiocavernosus[5].The dorsal penile nerve(DPN)is a sensory branch of the pudendal nerve that transmits afferent signals from the penis to the lumbosacral trunk.The emission phase is controlled by the autonomic neurons mainly the sympathetic chain while the expulsion phase is controlled by somatic neurons[6].The soma of the preganglionic sympathetic neurons involved in the control of ejaculation is located in the intermediolateral cell column and the central autonomic region of the thoracolumbar segments(T12-L1).Axons of motoneurones involved in the control of expulsion phase are found in the Onuf’s nucleus in the sacral spinal cord,which gives motor branches to the pudendal nerve that innervates the pelvic floor striated muscles[7].
Gruenwald et al.[8]used new methods to treat PE by inhibiting the rhythmic contractions of bulbospongiosus and ischiocavernosus muscles using transcutaneous neuromuscular electrical stimulation.By stimulating the perineal muscle,the pudendal nerve afferents were activated,which results in contractions of the muscles in the pelvic floor,keeping them in a sub-tetanic sustained contraction for several minutes[8].Uribe et al.[9]conducted a phase II trial to assess the efficacy and safety of transcutaneous posterior tibial nerve stimulation(TPTNS)for PE treatment.Twelve men with PE and no prior treatment were enrolled in the study.TPTNS was given as 30-min sessions(it consisted of the application of 20 Hz with a pulse amplitude of 200 μs).The fold increase of the intravaginal ejaculation latency time(IELT)to baseline was 2.8 at Week 6,4.8 at Week 12,6.8 at Week 24,and 5.4 at Week 48.Patients treated with TPTNS did not present adverse events that affected adherence to the therapy[9].
Based on the previous results,we tested the feasibility of stimulating the DPN,a component of the pudendal nerve in persons with refractory PE.We treated a 28-year-old man with lifelong PE diagnosed according to the Diagnostic and Statistical Manual of Mental Disorders Fifth Edition and International Society for Sexual Medicine[10].He was in a stable heterosexual relationship for more than 12 months,with a frequency of intercourse not less than twice perweek,and had no erectile dysfunction,any cardiovascular or neurologic disease,or major psychiatric or psychological illness including depression.The patient had a mean of IELT of 40 s experienced on almost all occasions of sexual activity.In this case,the PE was resistant to selective serotonin reuptake inhibitor treatment for 12 months and topical anesthetics used also for 6 months without any improvement.After a washout period of 3 months,the patient was treated by transcutaneous DPN stimulation(TDPNS).
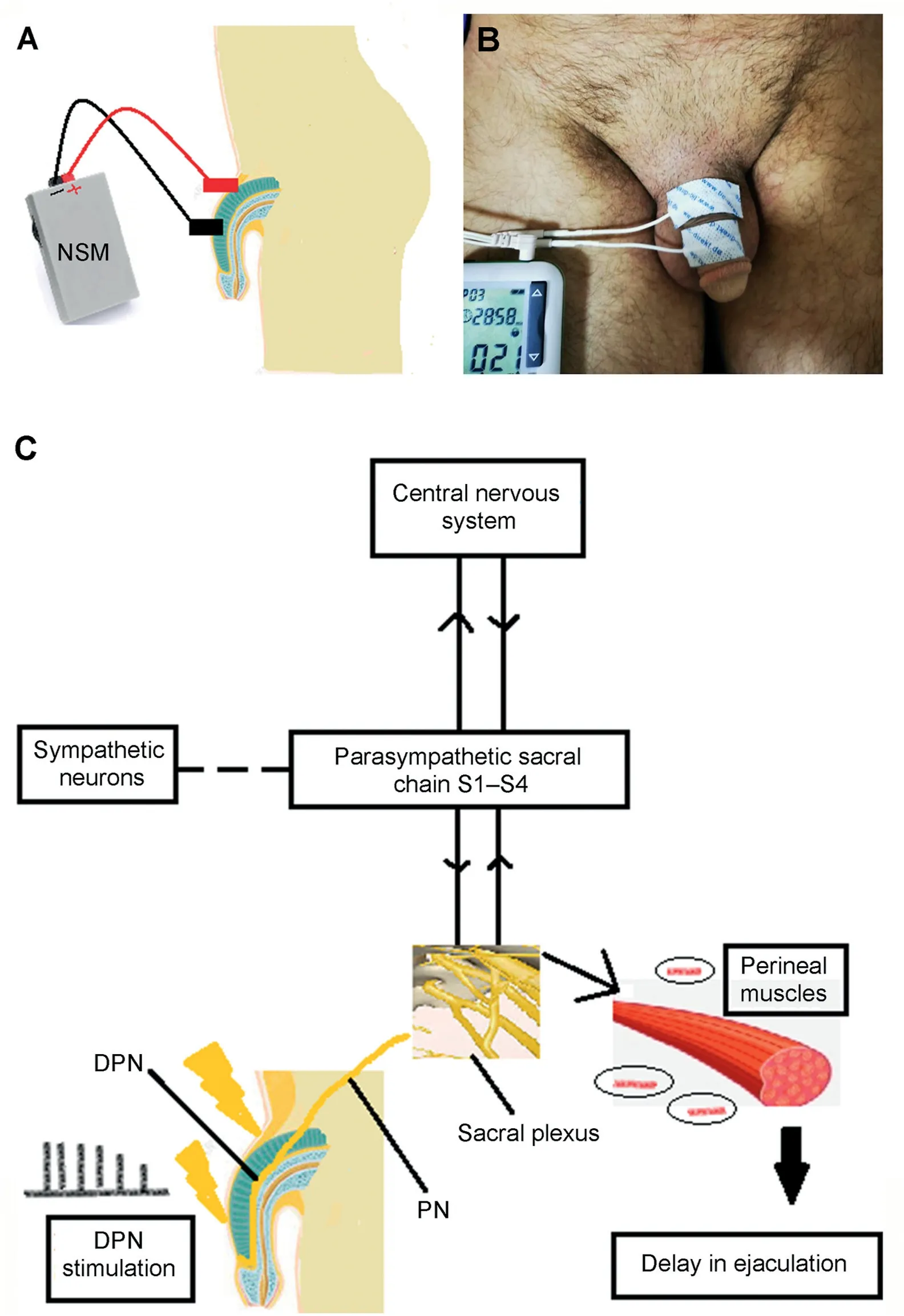
Figure 1 TDPNS.(A)Schematic drawing of the position of electrodes for TDPNS;(B)Photo of the position of electrodes on patient for TDPNS;(C)Mechanism of action of TDPNS.The stimulation of the DPN modulates the sacral plexus and acts at the parasympathetic segment which inhibits the contraction of the ischiocavernosus and bulbospongiosus muscles.It can affect the sympathetic neurons that control the emission phase of ejaculation.TDPNS could also target different neural circuitry in the central nervous system.TDPNS,transcutaneous dorsal penile nerve stimulation;NSM,nerve stimulator machine;PN,pudendal nerve;DPN,dorsal penile nerve;S1-S4,sacral spinal nerves(1-4).
Two round surface electrodes were placed on the dorsum of the penile shaft.The cathode and anode were placed at 2 cm apart.The cathode was placed proximally and the anode was placed distally(Fig.1A and B).Three sessions per week were conducted for 24 weeks,during which TDPNS was performed in a 30 min session using the following settings:a continuous current,with a frequency of 20 Hz and a pulse width of 200 μs.The current was set between 20 mA and 60 mA,at a level equal to twice the threshold for contraction of the anal sphincter.This intensity of stimulus pulse to DPN was suggested by Kirkham et al.[11].The follow-up period was 9 months.The patient agreed to participate in this study by signing informed written consent and contented to have his case published.The patient tolerated the treatment well with no reported adverse event.
The IELT is defined as the time from vaginal penetration to intravaginal ejaculation.IELT was determined by the stopwatch method for every intercourse.The primary outcome was stopwatch-measured IELT,which was reported for each intercourse episode.During the TDPNS,the mean of IELT increased significantly from 0.6 min at baseline to 3.9 min at Week 24(upon finishing of treatment),4.0 min at Week 36,4.8 min at Week 48,4.9 min at Week 60.
This TDPNS was chosen because it is less invasive than the percutaneous technique and more accepted by patients;therefore,we avoided the drop-out from treatment.The exact mechanism of how this new modality can affect ejaculation is not fully understood.We could extrapolate some theories from the studies that assess the effect of DPN stimulation on overactive bladder.The DPN is a terminal branch of the pudendal nerve.In overactive bladder,somatic inputs via the pudendal nerve reduce the output of the parasympathetic efferent innervation of the bladder by direct post-synaptic inhibition[12].DPN stimulation may inhibit the parasympathetic ejaculatory outputs and modulate the Onuf’s nucleus in the sacral spinal cord,which inhibits the motor response of the bulbospongiosus,and ischiocavernosus muscles(Fig.1C).The nerve is also a direct branch of the pudendal nerve and has therefore,in theory,shorter access to the nerves that control lower urinary tract function compared to the TPTNS.
TDPNS had multiple advantages over percutaneous tibial nerve stimulation.It is a noninvasive procedure;it reduces the risk of iatrogenic infections or complications.
Despite that we reported in one case the success of TDPNS in the treatment of PE by improving IELT,this case suggests that TDPNS if studied further could be a safe,nonpharmacological treatment for PE.Future trials with a larger group of patients,with objective measurements,are needed to prove this new strategy to manage PE.
Author contributions
Study concept and design:Mohamad Moussa,Mohamad Abou Chakra,Youssef Fares,Baraa Dabboucy,Athanasios Papatsoris,Athanasios Dellis.
Data acquisition:Mohamad Moussa,Mohamad Abou Chakra.
Data analysis:Mohamad Abou Chakra,Baraa Dabboucy.
Drafting of manuscript:Mohamad Moussa,Mohamad Abou Chakra,Baraa Dabboucy.
Critical revision of the manuscript:Mohamad Moussa,Mohamad Abou Chakra,Youssef Fares,Baraa Dabboucy,Athanasios Papatsoris,Athanasios Dellis.
Conflicts of interest
The authors declare no conflict of interest.
Mohamad Moussa
Chairman of Urology Department,Lebanese University,Beirut,Lebanon
Mohamad Abou Chakra*
Department of Urology,Lebanese University,Beirut,Lebanon
Baraa Dabboucy
Department of Neurosurgery,Faculty of Medicine,Lebanese University,Beirut,Lebanon
Youssef Fares
Department of Neurosurgery,Neuroscience Research Center,Faculty of Medical Sciences,Lebanese University,Beirut,Lebanon
Athanasios Dellis
Department of Urology/General Surgery,Areteion Hospital,Athens,Greece
Athanasios Papatsoris
2nd Department of Urology,School of Medicine,Sismanoglio Hospital,National and Kapodistrian University of Athens,Athens,Greece
*Corresponding author.
E-mail address:mohamedabouchakra@hotmail.com(M.A.Chakra)
7 July 2021
 Asian Journal of Urology2022年3期
Asian Journal of Urology2022年3期
- Asian Journal of Urology的其它文章
- Burned-out testicular seminoma with retroperitoneal metastasis and contralateral sertoli cell-only syndrome
- Endoscopic management of adolescent closed Cowper’s gland syringocele with holmium:YAG laser
- Bilateral calcified Macroplastique? after 12 years
- Culture-positive urinary tract infection following micturating cystourethrogram in children
- A phase II study of neoadjuvant chemotherapy followed by organ preservation in patients with muscle-invasive bladder cancer
- Augmentation cystoplasty in children with stages III and IV chronic kidney disease secondary to neurogenic bladder