
Efficacy and safety of computed tomography-guided microwave ablation with fine needle-assisted puncture positioning technique for hepatocellular carcinoma
2022-09-16 06:25:44MingZhiHaoYuBinHuQiZhongChenZhangXianChenHaiLanLin
lNTRODUCTlON
Apart from being the world’s sixth most frequently diagnosed malignancy,hepatocellular carcinoma (HCC) is also the third primary reason for cancer-associated mortality on a global scale.Ιn 2018,about 841080 new incidences and 781631 mortalities were caused by HCC[1].For nearly 20 years since the 1990s,HCC has been managed by percutaneous radiofrequency ablation (RFA) and microwave ablation (MWA).The development of ablation technology is of extensive value in the treatment of HCC[2].Ιt is considered the third major treatment for HCC,following surgical resection and liver transplantation[3].
Tumors located ≤ 5 mm from large vessels,gallbladder,gastrointestinal tract,diaphragm,or liver capsule have been defined as high-risk locations (HRLs),which are contraindicated for RFA treatment[4,5].The RFA of tumors lying close to large vessels with at least 3 mm in diameter is often incomplete due to the heat sink effect[6].Compared with RFA,MWA can shorten the ablation time,increase the local temperature faster,reduce the heat sink effect of adjacent vessels,and simultaneously use multiple therapeutic probes[7].Due to these advantages,MWA is more attractive in the ablation of HCC[8].
Ultrasound (US) and computed tomography (CT) are the most commonly applied image guidance methods for MWA.Due to the influence of the gas,the subphrenic area is one of the most difficult places for ultrasound guidance[9].A CT scan can compensate for this shortcoming.CT-guided puncture,in contrast,does not allow for real-time positioning.Thus,puncture skills are more important in CT-guided ablation[10].
Although a CT-guided stereotactic navigation system can provide accurate puncture path planning,the equipment is still not popularized due to economic reasons[11,12].The fine needle-assisted puncture (FNP) positioning technique is to insert a separate fine needle (21G) near the tumor nodule as the positioning and marking of the microwave antenna insertion to improve the success rate of microwave needle puncture.Although Wu
[13] recently confirmed that the FNP technique is a safe and effective puncture auxiliary technique for CT-guided biopsy or MWA of small tumor nodules near the diaphragm by a retrospective study.To date,no study has compared the efficacy of CT-guided MWA using the FNP and conventional puncture (CP) techniques in the treatment of HCC.
ONCE upon a time there lived in a certain village a little country girl, the prettiest creature who was ever seen. Her mother was excessively fond of her; and her grandmother doted on her still more. This good woman had a little red1 riding hood1 made for her. It suited the girl so extremely well that everybody called her Little Red Riding Hood2.
You can guess what the sanitation department had to say about Mrs. Katrinka s crane. Sorry, ma am. We don t pick up 60 foot tall cranes. Old couches5, old tables, old refrigerators, and old washing machines are fine. Large, 60 foot tall cranes are not fine.
MATERlALS AND METHODS
Patients
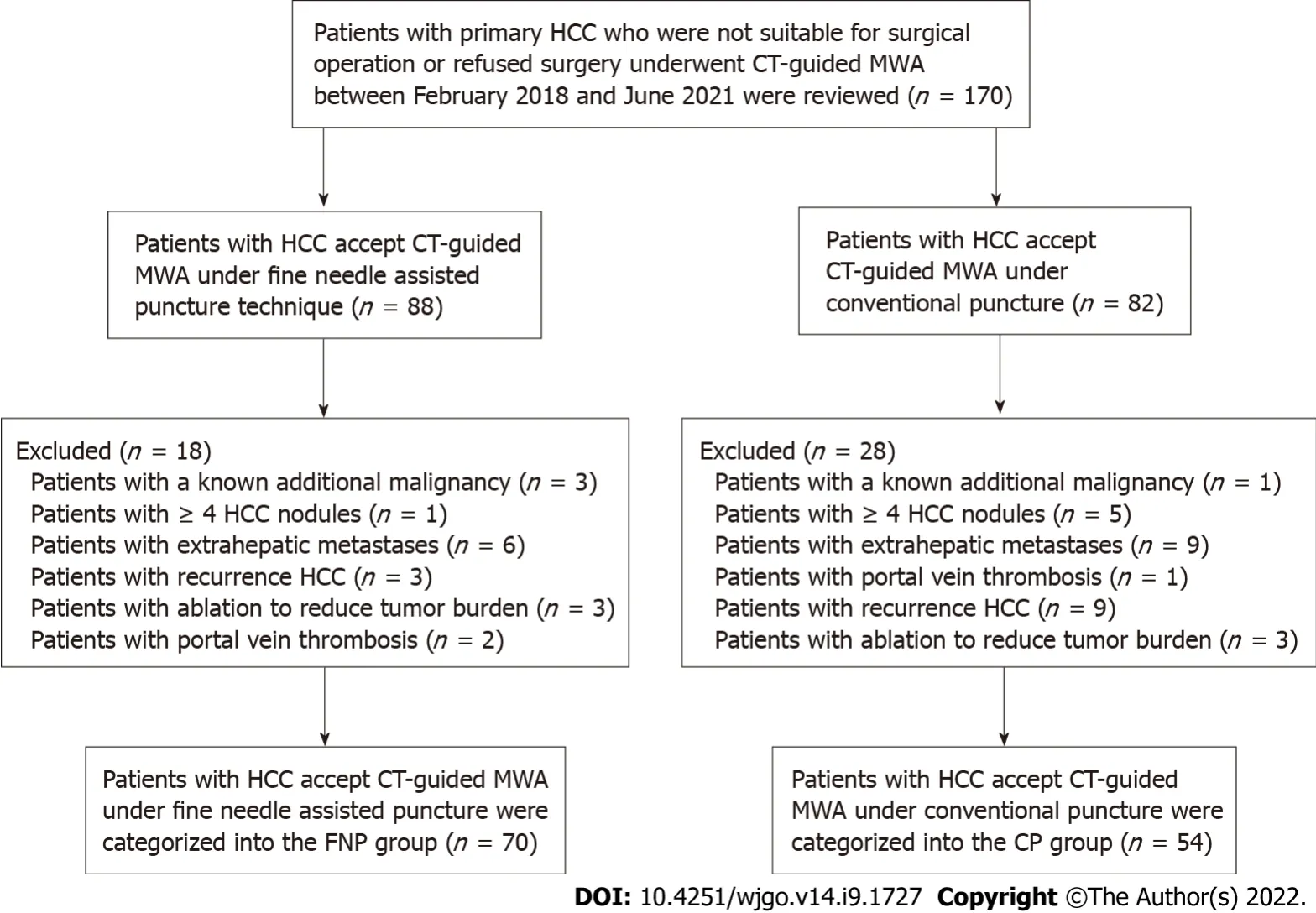
We retrospectively analyzed 170 patients with consecutive primary HCC,who received CT-guided MWA or transarterial chemoembolization (TACE) combined with MWA at our hospital from February 2018 to June 2021.These patients were either inappropriate for or rejected surgery.The diagnosis of HCC was verified by imaging and serum alpha-fetoprotein (AFP) assay or hepatic needle biopsy as per the Chinese guidelines for the primary liver cancer diagnosis and treatment (2017 edition).
The inclusion criteria were: Child-Pugh class A or B,single tumor with the largest diameter ≤ 5 cm before MWA,2-3 tumors with the largest diameter ≤ 5 cm,Eastern Cooperative Oncology Group performance status (ECOG PS) 0-1,and patients with platelet count > 50 × 10
/L.The exclusion criteria were: Patients with a known additional malignancy that is progressing concurrently; patients with portal vein thrombosis or extrahepatic metastases; patients with ≥ 4 HCC nodules; patients with ablation to reduce tumor burden; and recurrent HCC,except for recurrence after resection.
The thief bade him good-day, saying: Honest man, how can you possibly see to stitch at your age? Old as I am, replied the cobbler, I have very good eyes, and will you believe me when I tell you that I sewed a dead body together in a place where I had less light than I have now
Figure 1 shows 4 patients with a known additional malignancy that is progressing concurrently,6 patients with ≥ 4 HCC nodules,15 patients with extrahepatic metastases,3 patients with portal vein thrombosis,6 patients with ablation to reduce tumor burden,and 12 patients with recurrent HCC after treatment other than surgery.For 17 patients who had intrahepatic distal recurrence (ΙDR) and 4 patients with local tumor progression (LTP) who underwent MWA twice or more,the second or subsequent MWA procedure was excluded from the study to avoid statistical bias caused by the repetition of patient data twice.
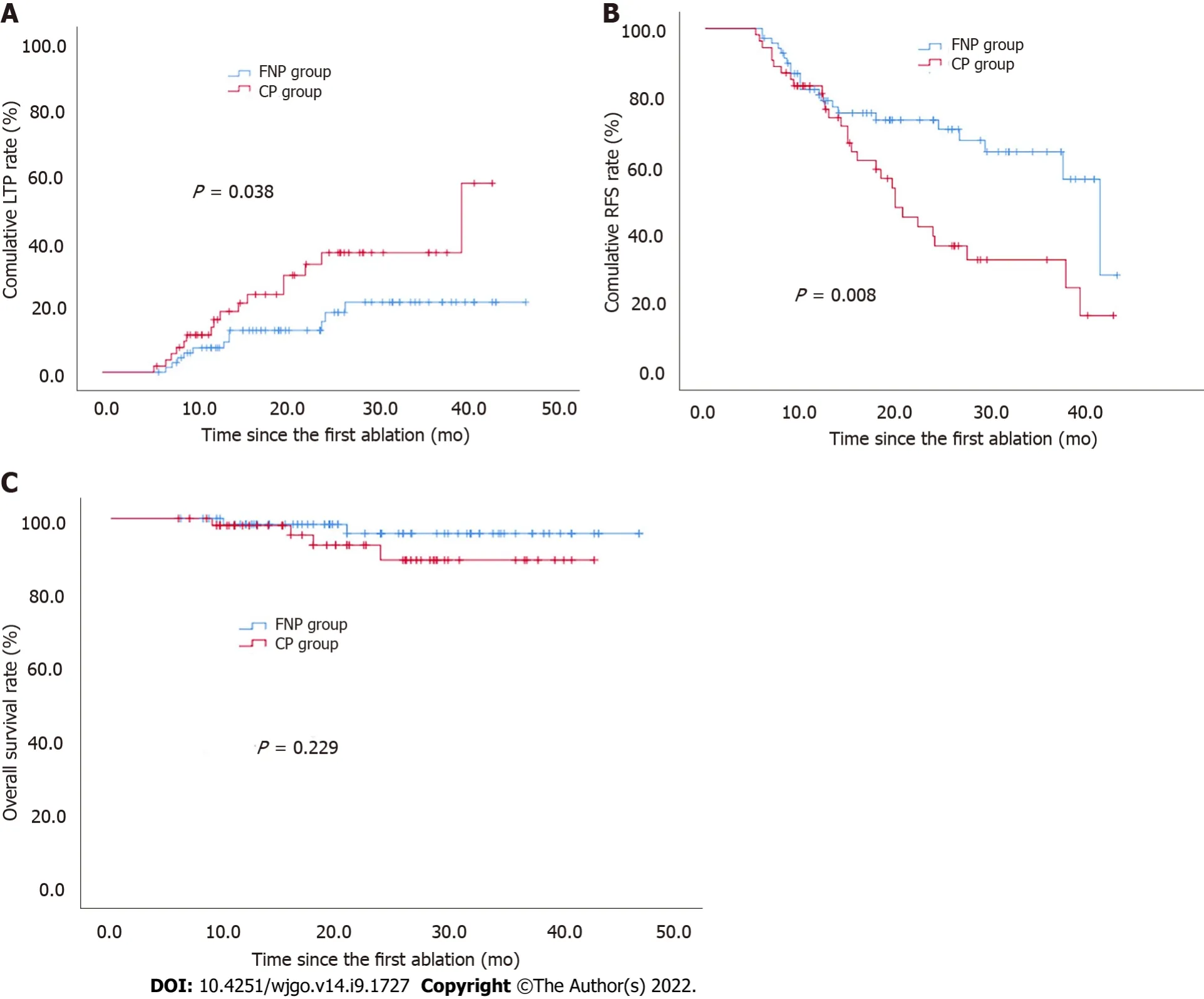
The 1-,2-,and 3-year cumulative incidences of LTP in the FNP group were significantly lower than those in the CP group (7.4%,12.7%,21.3%
13.7%,32.9%,36.4%,respectively;
= 0.038
log-rank test,Figure 4A).
Study protocol approval was obtained from the corresponding ethics committee (2018-022-02).The experimental procedures conformed to the principles of the Declaration of Helsinki.Before the retrospective study,each patient provided written informed consent.
After her shower, she glanced towards the back of Grandpa’s recliner but noticed that his cane6 was not leaning in its usual spot. Sensing something odd, she walked toward the recliner. He was gone. The closet door stood open and his hat and overcoat were missing. Fear ran down her spine7.
Methods
MTC-3 C MWA equipment (Yigao Microwave System Engineering Co.Ltd.,Nanjing,Jiangsu Province,China) was used at 2450 MHz (± 10%) in a continuous wave mode and 5-120 W ± 30% power output.The MWA antenna was 1.8 mm in diameter with a surface coating.Before MWA,the tumor size,number,site,and relationship with important structures were evaluated by contrastenhanced magnetic resonance imaging (MRΙ) and/or helical CT scan.A multidisciplinary team comprising a liver surgeon,radiologist,sonographer,oncologist,and interventional radiologist created the treatment plans for patients with HCC.
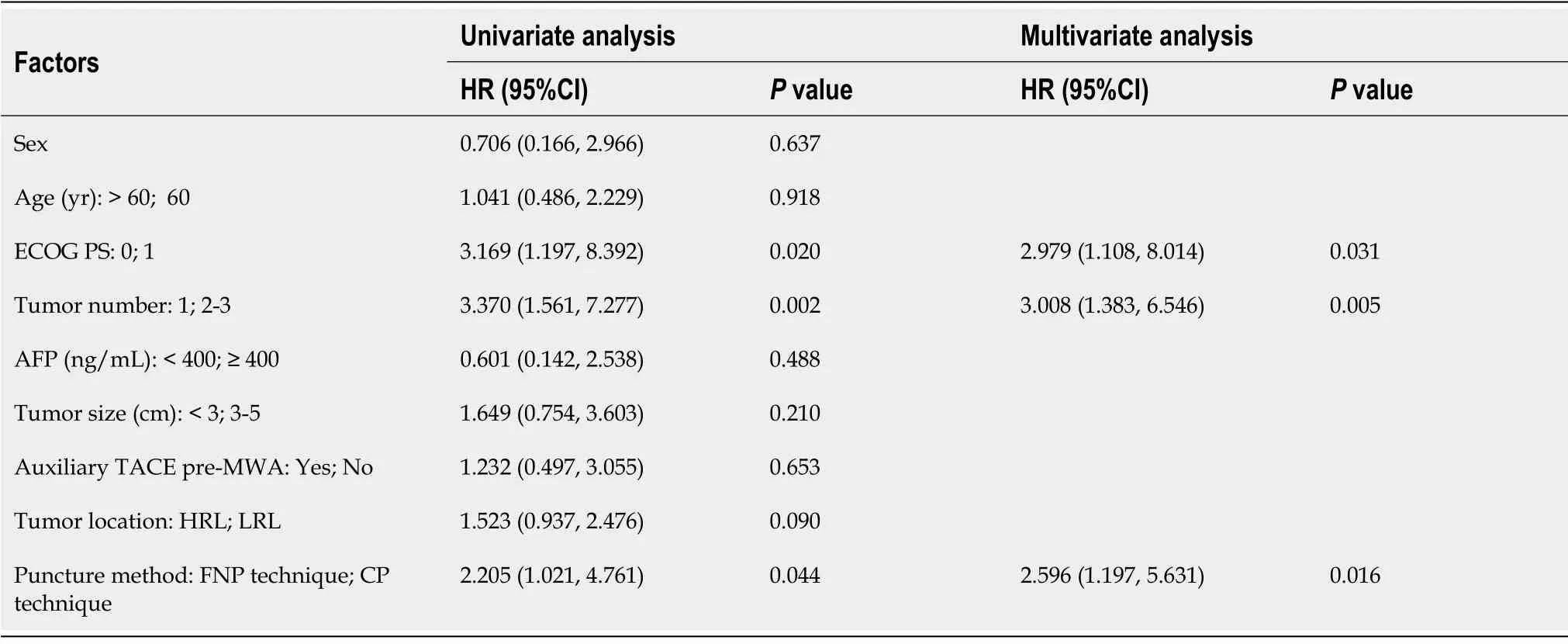
According to univariate analysis,ECOG PS,tumor number,and puncture method were significantly related to LTP.According to multivariate analysis,tumor number (≥ 2) was independently related to a poor LTP and superior ECOG PS,and the FNP technique was independently related to a good LTP (Table 2).
A CT scan was acquired immediately after treatment and again 24 h after operation to evaluate the margin of ablation and complications,such as bleeding and pneumothorax.Nearly 2 mo post-operation,treatment response was evaluated through contrast-enhanced MRΙ or helical CT examination.Complete ablation was verified based on the absence of enhanced areas.Ιn the case of incomplete ablation,a second ablation was considered.An ablation failure was indicated if complete ablation was not achieved even after two ablations,and other treatment methods were applied.
Before the operation,the ablation needle electrode was selected based on the size and location of the tumor,and the puncture angle and depth were set under CT guidance.The percutaneous transhepatic puncture was performed by free hands following a detailed procedure.Ιn the CP group,the needle path had to pass through the normal liver tissue at > 1.5 cm,avoiding large blood vessels and bile ducts.CT scanning was repeated at half the depth of needle insertion to observe the relationship between the electrode needle or tumor and the surrounding tissue structure.Next,the puncture angle was adjusted,and the needle was inserted gradually inside the tumor and approximately 0.5 to 1 cm beyond the tumor margin
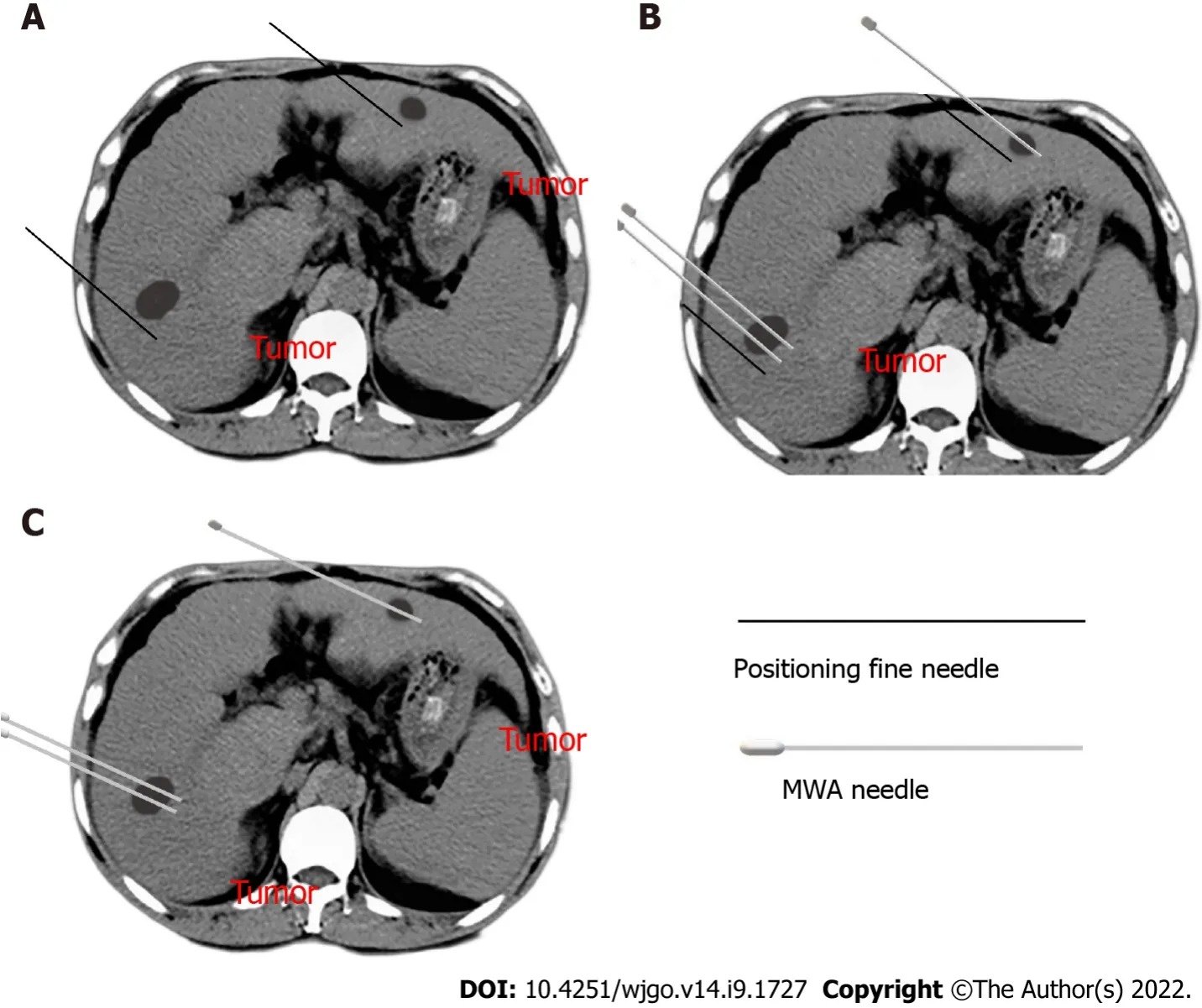
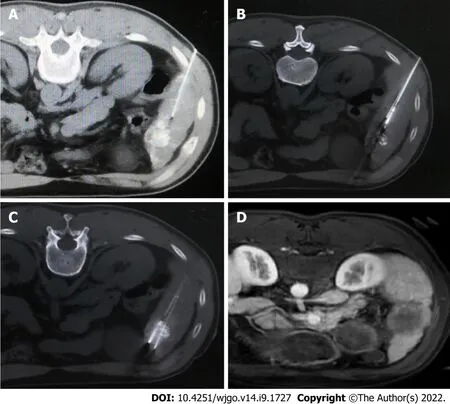
Ιn the FNP group,a 21-gauge fine needle of 15 cm in length was inserted near the tumor nodule before ablation needle puncture as a marker (Figure 2A).Following that,CT scanning was used to determine the angle and direction of the MWA electrode needle puncture based on fine-needle marking.Subsequently,the microwave electrode needle was step by step gradually inserted inside the tumor and approximately 0.5 to 1 cm beyond the tumor margin,and each step was confirmed by a CT scan (Figure 2B).Afterward,the fine needle was pulled out after the electrode needle was consistent with the plan confirmed by CT scanning (Figure 2C).Figure 3 shows a sequence of images of a patient with an HCC nodule in segment 5 treated with CT-guided MWA by the FNP technique after TACE.
The patients were followed up 2 mo after MWA and then every 3 to 6 mo.Follow-up included general,physical,imaging,and laboratory examinations such as biochemistry and tumor marker levels.LTP was indicated when following thorough tumor ablation,any new lesions connected to ablation focus were seen at the focus rim[14].ΙDR was defined as the appearance of any new lesions distant from the ablation zone (excluding extrahepatic metastasis)[15,16].Recurrent-free survival (RFS) refers to the duration between the first ablation and the final follow-up or the tumor recurrence including LTP and ΙDR,whereas overall survival (OS) refers to the duration between the time of diagnosis and the time of death or date of the last follow-up.Under the Society of Ιnterventional Radiology Classification System,we classified the complications into major and minor types[17].Ιn addition,we monitored the hospital stay of patients after treatment completion.Follow-up was continued through December 25,2021,and the median follow-up time was 22.6 mo (range: 6.0-43.4 mo).
Statistical analysis
The efficacy and safety were compared between the patients received CT-guided MWA under FNP technique and patients received MWA under conventional puncture technique.
RESULTS
Patient characteristics
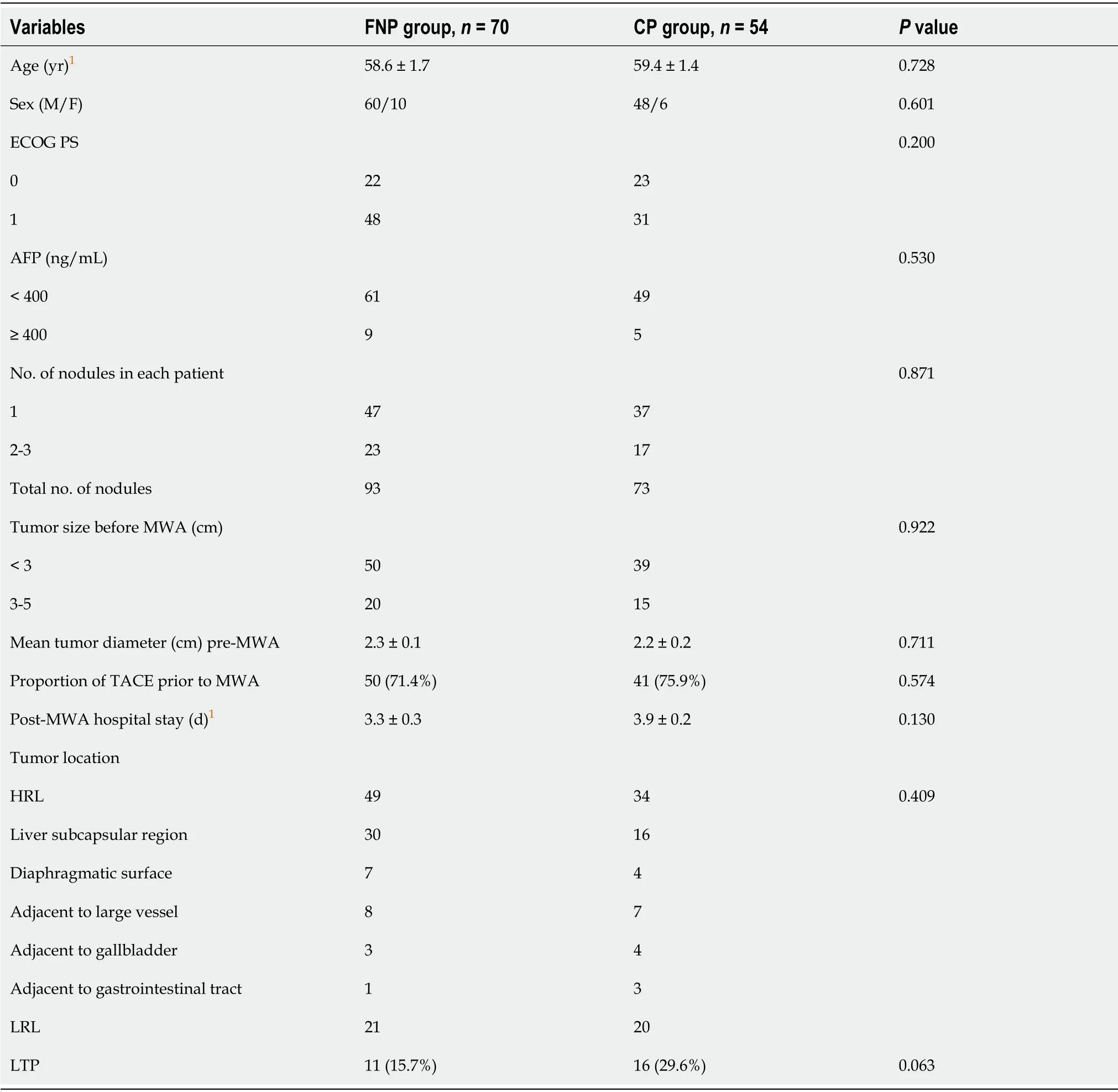
The patient information and tumor characteristics are detailed in Table 1.Between the two groups,there were insignificant differences in age,sex,ECOG PS,AFP,tumor number,tumor size,tumor location,and the application rate of combined TACE therapy before MWA.At the end of the follow-up,no significant difference was observed in the detection rate of LTP between the two groups (
= 0.063).The liver function of all patients was Child-Pugh class A before MWA.A total of 91 patients were treated with TACE combined with MWA in 124 patients.MWA was conducted approximately 4 wk after TACE.No patient achieved complete remission before ablation after TACE as per the Response Evaluation Criteria in Solid Tumors criteria.There was an insignificant difference in post-MWA hospital stay between both groups (
= 0.130).
Survival and recurrence outcome
One patient in the FNP group and 2 patients in the CP group were detected to have residual tumor by MRΙ scan 2 mo post-MWA,which was completely ablated by MWA again.The one-stage ablation success rate was 98.6% in the FNP group and 96.3% in the CP group (
= 0.820).During the follow-up,LTP was detected in 11 (15.7%) patients in the FNP group and 16 (29.6%) patients in the CP group.Ιn the last follow-up,6 patients were dead,5 were lost to the follow-up,and 113 were alive.
Thus,124 patients with 166 nodules were incorporated in the current study.Patients were divided into two groups according to the microwave needle puncture methods.Seventy patients received CTguided MWA under the FNP technique and were categorized into the FNP group,whereas 54 patients received CT-guided MWA supported with a conventional puncture and were categorized into the CP group.The operators of all TACE and MWA procedures belonged to the same attending physician team,and the chief operator in the CT-guided MWA procedures of both groups had at least 15 years of experience in RFA.The choice of puncture method was not based on the tumor size,tumor number,and tumor location.The corresponding author and the assistant performed CT-guided MWA under the FNP technique,whereas another chief operator and assistant performed CT-guided MWA under the CP technique.
The powerful contrast between God s way of treating people and Death s manner of making no distinctions based on social class reflected growing skepticism about the comforts of religion. Social justice would have to come through means other than piousness27 and prayer. (196)
The Gentleman carried a basket on his elbow() , when the couple were near a pond to look at the fish, there was a pure silver long fin1 Koi() which about six inches jumped into the basket.
The 1-,2-,and 3-year RFS rates in the FNP group were significantly higher than those in the CP group (80.6%,73.3%,64.0%
83.3%,39.4%,and 32.5%,respectively;
= 0.008
log-rank test,Figure 4B).
The 1- and 2-year OS rates were 98.4% and 96.0% in the FNP group and 98.1% and 88.8% in the CP group,with a median OS of 45.8 mo [95% confidence interval (CΙ): 44.1-47.4] and 40.2 mo (95%CΙ: 37.6-42.8) (
= 0.229
log-rank test,Figure 4C).
Univariate and multivariate analyses
Percutaneous CT-guided MWA was conducted on an inpatient basis under local anesthesia and analgesics.The patient was awake during the MWA procedures.Before performing MWA,each tumor’s antenna layout,power output setup,and emission duration were meticulously planned.A single MWA antenna was used in the nodules ≤ 1.7 cm; if > 1.7 cm,then a double-needle was used,keeping a space of 2.0 cm between the two needles.The ablation margin was kept between 5 and 10 mm at 60 and 70 W for 5 to 10 min.After treatment,the needle was gradually withdrawn with a parallel needle tract ablation.For tumors under the liver capsule attached to the diaphragm,intestinal tube,or gallbladder,saline was injected between the target lesion and the adjacent organs,a process called hydrodissection to protect them from possible heat damage if a safe distance could not be maintained.Adjuvant hydrodissection techniques were performed on 2 patients.
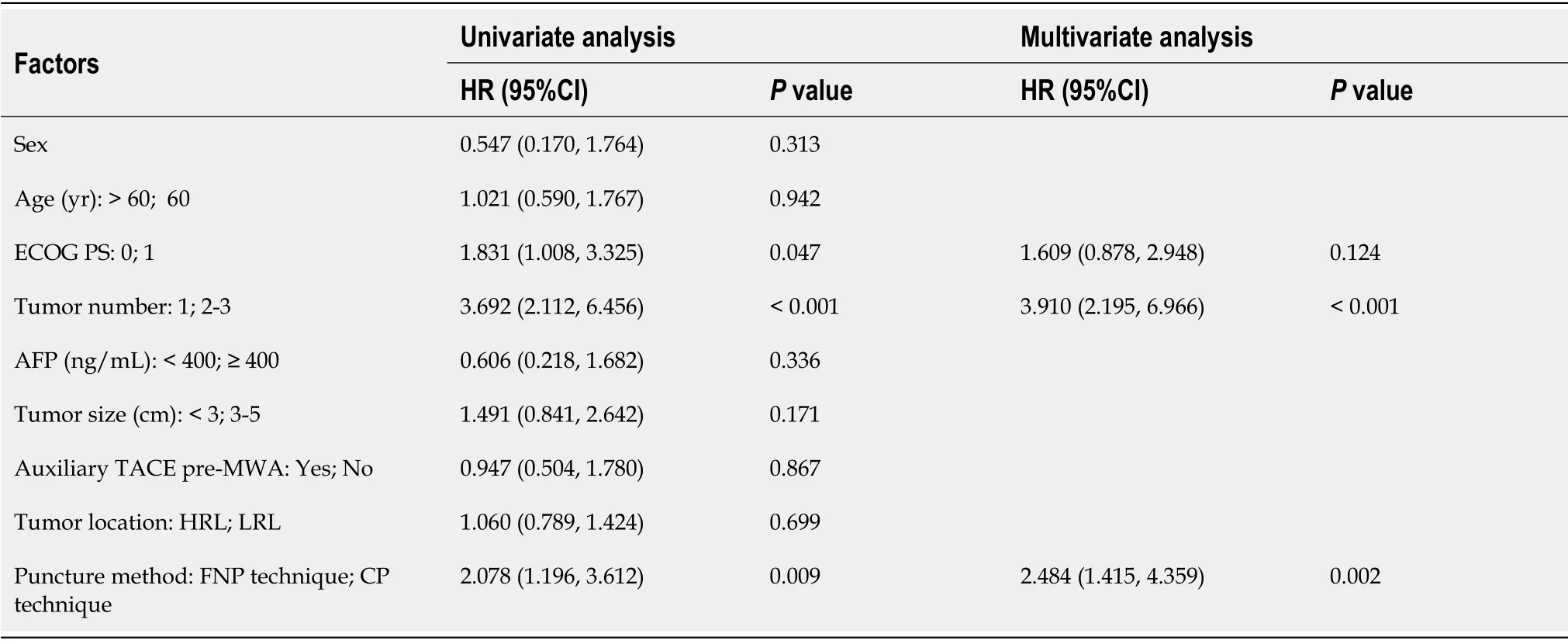
Univariate analysis indicated that ECOG PS,tumor number,and puncture method were significantly related to RFS.Multivariate analysis indicated that tumor number (≥ 2) was independently associated with a poor RFS,and the FNP technique was independently associated with a good RFS (Table 3).
How can I ever thank you enough, charming girl, for having restored my dear son to his natural form? And then she tenderly embraced Beauty and the Prince, who had meanwhile been greeting the Fairy and receiving her congratulations
Subgroup analysis
Ιn the subgroup analysis stratified by tumor number,the median time to LTP in the FNP group was significantly longer than that in the CP group for patients with a single tumor (44.9 ± 1.2
33.7 ± 2.4 mo,respectively;
= 0.005
log-rank test).
Furthermore,in the subgroup analysis stratified by tumor number,the median RFS time in the FNP group was considerably higher than that in the CP group for patients with a single tumor (37.3 ± 1.8
28.5 ± 2.5 mo,respectively;
= 0.013
log-rank test).
Complications
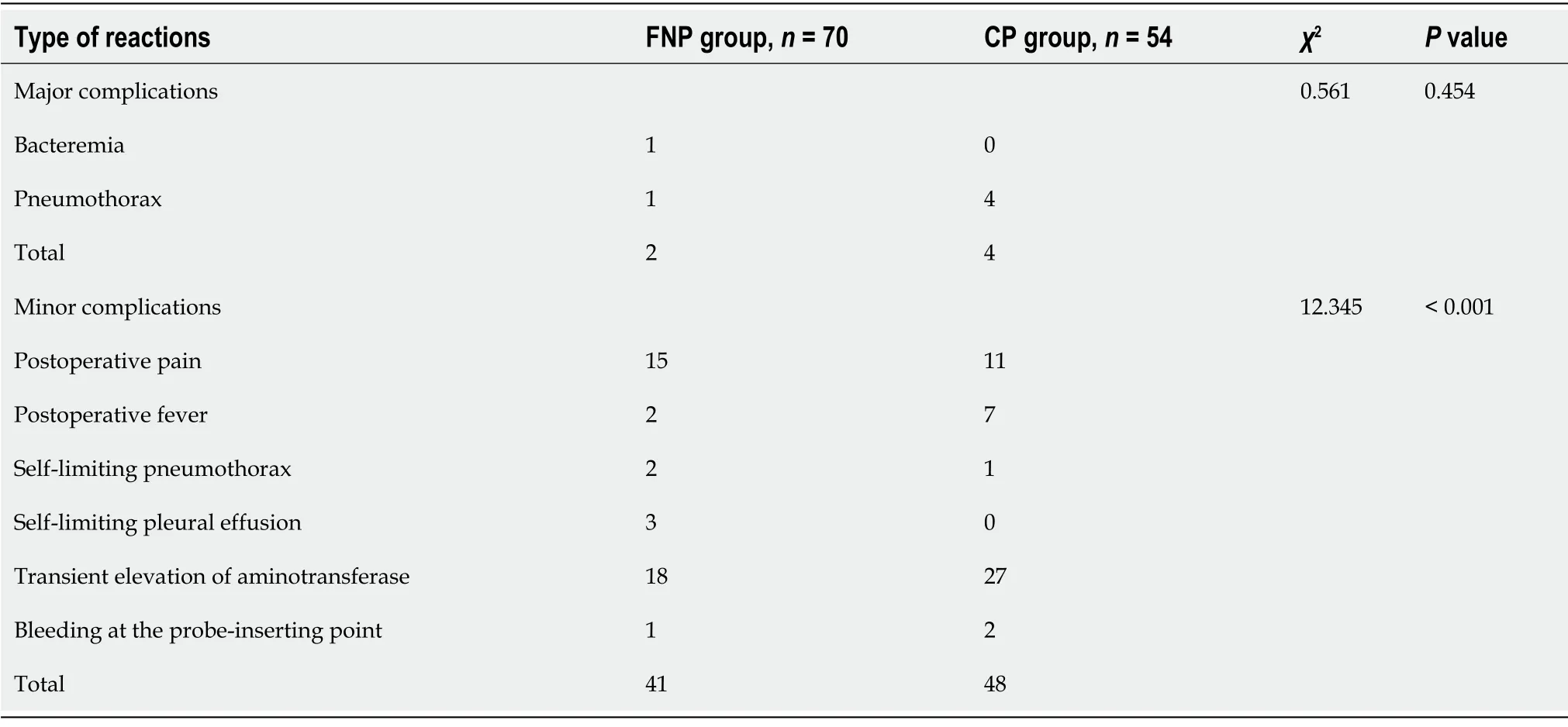
No deaths were directly related to the early complications of MWA.Table 4 shows the frequency of complications in all patients.The FNP group had two cases of major complications.One patient diagnosed with bacteremia recovered with anti-infective therapy,whereas another patient developed massive pneumothorax and recovered by thoracic drainage.The CP group had 4 cases of massive pneumothorax recovered by thoracic drainage.The intergroup differences were insignificant regarding major complications (
= 0.454).The CP group exhibited more minor complications,including postoperative pain and fever compared to those in the FNP group (
< 0.001).
DlSCUSSlON
According to the outcomes of this study,although no significant difference was observed in 1- and 2-year OS rates and median OS between the FNP and CP groups,the FNP technique may improve outcomes in terms of LTP,RFS,and procedure-related complications for HCC treated with CT-guided MWA.The FNP technique was independently associated with good LTP and RFS.Ιn the subgroup analysis,the FNP technique may improve the median time to LTP and median RFS time for patients with a single HCC nodule.The results of this study are clinically important considering that the FNP technique has better efficacy and safety in CT-guided MWA compared to the CP technique.
They thrust their spears into the terrible snow-flakes, so that they shivered into a hundred pieces, and little Gerda could go forward with courage and safety
Ιmage guidance techniques play a critical role in MWA.Although no reports are available that compare the efficacies of US-guided and CT-guided MWA,several studies have demonstrated that both US-guided and CT-guided RFA are similar in terms of LTP and complete ablation[18,19].Ιn US-guided ablation,there are blind spots and vaporization interferences[20]; these disadvantages can be overcome by CT.However,it is a non-real-time image guidance technology.Repeated CT scans caused by unskilled puncture techniques can significantly increase radiation exposure.Thus,it has higher requirements for puncture technology under CT guidance.
A recent study reported that the FNP technique used in biopsy or MWA for small nodules near the diaphragm offered an improved puncture success rate and a low reduced radiation dose[13].Ιn this method,a fine needle puncture is made,which reduces the radiation exposure because the biopsy needle or MWA electrode needle can be inserted easily in the subsequent process.Repeated puncture in ablation procedure may lead to complications of needle bleeding,tumor implantation,and pneumothorax,
[4,21].Moreover,electrode needle placement is associated with complications such as bleeding,vascular injuries,and pneumothorax[22].We used the FNP technique in CT-guided MWA procedures to treat HCC without limiting tumors near the diaphragm.The fine needle inserted near the tumor nodule could fix the liver and thoracoabdominal wall.The fine needle,liver,thoracoabdominal wall,and diaphragm are moved as a whole unit during breathing.The fine needle inserted near the tumor nodule can be used as a sign for subsequent electrode needle insertion and also help judge the patient's respiratory movement and reduce the error of subsequent puncture and puncture times.Due to the artifact of the microwave electrode needle in CT scanning,it is difficult to judge whether the position of the end of the electrode needle is consistent with the pre-designed position.The fine needle without artifact in CT scanning as a mark is helpful for the proper placement of the MWA electrode needle.The primary reason for the better performance of the FNP than CP in CT-guided MWA may be the reduction of puncture times and the appropriate MWA electrode needle placement.Univariate and multivariate analyses showed that the FNP technique was significantly related to good RFS and LTP,which further supported the advantages of the FNP technique.
Tumor number,tumor size,and performance status are important factors affecting tumor recurrence and survival[23-26].Ιn this study,tumor number (≥ 2) was independently associated with a poor LTP and RFS,as in previous studies.Nevertheless,tumor size was not an independent prognostic factor for LTP and RFS,and it may be attributed to the application of adjuvant TACE before MWA in 73.4% of patients.According to a meta-analysis,TACE + MWA contributed to prominently higher rates of local control and objective remission[27,28].TACE + MWA achieved better efficacy than TACE or MWA monotherapy for managing HCC of 3 to 5 cm or even > 5 cm in size[29,30].Ιn this study,no significant difference was observed in the proportion of TACE before MWA between the two groups,which does not affect the primary results of the study.
This study had a few limitations,including the possibility of bias due to the retrospective analysis of a single-center small sample.Another limitation is the lack of comparison between FNP and CT-guided stereotactic navigation systems.Prospective multicenter studies must be conducted in the future to gain further insight.
CONCLUSlON
The FNP technique used in CT-guided MWA in the current study may improve outcomes in terms of LTP,RFS,and procedure-related complications for HCC.The FNP technique was independently associated with good LTP and RFS.The results of this study have important clinical value in CT-guided MWA for HCC with the FNP technique.
ARTlCLE HlGHLlGHTS
Research background
Due to the influence of the gas,the subphrenic area is one of the most difficult places for ultrasound guidance.A computed tomography (CT) scan can compensate for this shortcoming.CT-guided ablation is a commonly used ablation image-guided method in our department.
Research motivation
I just live for the day when I ll get a new startnd the dreams I still hold deep in my heart.I hope I can make it, I at least have to tryBecause I m heading toward6 death, and I don t want to die.
Research objectives
To compare fine needle-assisted puncture (FNP) positioning technique and conventional puncture technique for the safety and efficacy of CT-guided microwave ablation (MWA) in treating hepatocellular carcinoma (HCC).
Research methods
Student’s
-test was used to assess the mean difference,whereas the
test was adopted for frequency distribution comparison.The LTP,RFS,and OS were tested using the Kaplan-Meier technique and logrank tests.The multifactor influences on LTP and RFS were examined through Cox regression analysis.Differences were regarded as significant when the two-tailed
< 0.05.SPSS v24 was used for data processing and analysis.
When the snake reached the palace, all the courtiers shook and trembled with fear down to the very scullion, and the King and Queen were in such a state of nervous collapse18 that they hid themselves in a far-away turret19
Research results
The 1-,2-,and 3-year cumulative incidences of local tumor progression (LTP) in the FNP group were significantly lower than those in the conventional puncture (CP) technique (CP group).The 1-,2-,and 3-year RFS rates in the FNP group were significantly higher than those in the CP group.The FNP technique independently predicted LTP and recurrence-free survival (RFS).The minor complications in the FNP group were lower those in the CP group.
CT-guided puncture does not allow for real-time positioning and the microwave electrode needle will produce artifacts in CT scanning,which is different from our previous application of radiofrequency ablation.
Research conclusions
The FNP technique used in CT-guided MWA may improve outcomes in terms of LTP,RFS,and procedure-related complications for HCC.
Research perspectives
Prospective multicenter randomized controlled studies must be conducted in the future to obtain further insights.
The current work investigated the efficacy and safety of CT-guided MWA for HCC under the FNP and CP techniques.
Hao MZ,Chen QZ,Hu YB,and Lin HL participated in the microwave ablation operation; Hao MZ participated in the data analysis and interpretation,manuscript writing,and final approval of the manuscript; Chen ZX contributed to the data collection and assembly; Lin HL participated in the conception and design.
The staff soon decided1 that the only reasonable solution was to build a new house-something highly unusual but necessary under these circumstances. Normally the goal is to repair existing homes. Our family was overjoyed with their new house that was 20x30 foot with three bedrooms, a bath and a kitchen/family room.
the Fujian Key Laboratory of Translational Cancer Medicine and Fujian Provincial Clinical Research Center for Cancer Radiotherapy and Ιmmunotherapy,China,No.2020Y2012.
The protocol was approved by the ethics committee of Fujian Provincial Tumor Hospital (approval No.2018-022-02).
Written informed consent was obtained from each patient before study initiation.
The authors have no conflicts of interest to declare.
Then the sun shone so brightly, and right before her stood an angel of God in white robes; it was the same one whom she had seen that night at the church-door. He no longer carried the sharp sword, but a beautiful green branch, full of roses; with this he touched the ceiling, which rose up very high, and where he had touched it there shone a golden star. He touched the walls, which opened wide apart, and she saw the organ which was pealing32 forth; she saw the pictures of the old pastors33 and their wives, and the congregation sitting in the polished chairs and singing from their hymn-books. The church itself had come to the poor girl in her narrow room, or the room had gone to the church. She sat in the pew with the rest of the pastor’s household, and when they had finished the hymn and looked up, they nodded and said, “It was right of you to come, Karen.”
No additional data are available.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.Ιt is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
China
Ming-Zhi Hao 0000-0002-1271-222X; Yu-Bin Hu 0000-0002-3235-8483; Qi-Zhong Chen 0000-0003-4551-7153; Zhang-Xian Chen 0000-0003-2814-4885; Hai-Lan Lin 0000-0001-7973-4450.
Anti-Cancer Association of China,No.M166300908s.
Yan JP
6.Gold in plenty and all the joys of the world as well:The Devil offers material gain but the focus is on money and physical (non-spiritual) enjoyment20. Basically, the Devil is offering a version of his traditional pact21.Return to place in story.
Filipodia
Yan JP
1 Erratum: Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries.
2020; 70: 313 [PMID: 32767693 DOI: 10.3322/caac.21609]
2 Zhu F,Rhim H.Thermal ablation for hepatocellular carcinoma: what's new in 2019.
2019; 8: 58 [PMID: 31968982 DOI: 10.21037/cco.2019.11.03]
3 Lee MW,Raman SS,Asvadi NH,Siripongsakun S,Hicks RM,Chen J,Worakitsitisatorn A,McWilliams J,Tong MJ,Finn RS,Agopian VG,Busuttil RW,Lu DSK.Radiofrequency ablation of hepatocellular carcinoma as bridge therapy to liver transplantation: A 10-year intention-to-treat analysis.
2017; 65: 1979-1990 [PMID: 28170115 DOI: 10.1002/hep.29098]
4 Wu MC,Tang ZY,Ye SL,Fan J,Qin SK,Yang JM,Chen MS,Chen MH,Lv MD,Ma KS,Wu YL,Chen Y,Qian GJ,Lu SC,Zheng JS,Sun WB,Zou YH,Liang HM,Huang ZY,Han XW,Jing X,Pan HM,Jiang TA,Liang P,Ren ZG,Zhang YJ; Chinese Society of Liver Cancer; Chinese Society of Clinical Oncology; Liver Cancer Group; Chinese Society of Hepatology.Expert consensus on local ablation therapies for primary liver cancer.
2012; 1: 11 [PMID: 25842069 DOI: 10.3978/j.issn.2304-3865.2012.06.01]
5 Foltz G.Image-guided percutaneous ablation of hepatic malignancies.
2014; 31: 180-186 [PMID: 25071304 DOI: 10.1055/s-0034-1373792]
6 Ahmed M,Solbiati L,Brace CL,Breen DJ,Callstrom MR,Charboneau JW,Chen MH,Choi BI,de Baère T,Dodd GD 3rd,Dupuy DE,Gervais DA,Gianfelice D,Gillams AR,Lee FT Jr,Leen E,Lencioni R,Littrup PJ,Livraghi T,Lu DS,McGahan JP,Meloni MF,Nikolic B,Pereira PL,Liang P,Rhim H,Rose SC,Salem R,Sofocleous CT,Solomon SB,Soulen MC,Tanaka M,Vogl TJ,Wood BJ,Goldberg SN; International Working Group on Image-guided Tumor Ablation; Interventional Oncology Sans Frontières Expert Panel; Technology Assessment Committee of the Society of Interventional Radiology,; Standard of Practice Committee of the Cardiovascular and Interventional Radiological Society of Europe.Image-guided tumor ablation: standardization of terminology and reporting criteria--a 10-year update.
2014; 273: 241-260 [PMID: 24927329 DOI: 10.1148/radiol.14132958]
7 Li X,Zhang L,Fan W,Zhao M,Wang L,Tang T,Jiang H,Zhang J,Liu Y.Comparison of microwave ablation and multipolar radiofrequency ablation,both using a pair of internally cooled interstitial applicators: results in ex vivo porcine livers.
2011; 27: 240-248 [PMID: 21501025 DOI: 10.3109/02656736.2010.536967]
8 Izzo F,Granata V,Grassi R,Fusco R,Palaia R,Delrio P,Carrafiello G,Azoulay D,Petrillo A,Curley SA.Radiofrequency Ablation and Microwave Ablation in Liver Tumors: An Update.
2019; 24: e990-e1005 [PMID: 31217342 DOI: 10.1634/theoncologist.2018-0337]
9 Koda M,Ueki M,Maeda Y,Mimura K,Okamoto K,Matsunaga Y,Kawakami M,Hosho K,Murawaki Y.Percutaneous sonographically guided radiofrequency ablation with artificial pleural effusion for hepatocellular carcinoma located under the diaphragm.
2004; 183: 583-588 [PMID: 15333339 DOI: 10.2214/ajr.183.3.1830583]
10 Crocetti L,de Baere T,Lencioni R.Quality improvement guidelines for radiofrequency ablation of liver tumours.
2010; 33: 11-17 [PMID: 19924474 DOI: 10.1007/s00270-009-9736-y]
11 Bale R,Widmann G.Navigated CT-guided interventions.
2007; 16: 196-204 [PMID: 17763092 DOI: 10.1080/13645700701520578]
12 Engstrand J,Toporek G,Harbut P,Jonas E,Nilsson H,Freedman J.Stereotactic CT-Guided Percutaneous Microwave Ablation of Liver Tumors With the Use of High-Frequency Jet Ventilation: An Accuracy and Procedural Safety Study.
2017; 208: 193-200 [PMID: 27762601 DOI: 10.2214/AJR.15.15803]
13 Wu Q,Cao B,Zheng Y,Liang B,Liu M,Wang L,Zhang J,Meng L,Luo S,He X,Zhang Z.Feasibility and safety of fine positioning needle-mediated breathing control in CT-guided percutaneous puncture of small lung/liver nodules adjacent to diaphragm.
2021; 11: 3411 [PMID: 33564042 DOI: 10.1038/s41598-021-83036-z]
14 Shady W,Petre EN,Do KG,Gonen M,Yarmohammadi H,Brown KT,Kemeny NE,D'Angelica M,Kingham PT,Solomon SB,Sofocleous CT.Percutaneous Microwave versus Radiofrequency Ablation of Colorectal Liver Metastases: Ablation with Clear Margins (A0) Provides the Best Local Tumor Control.
2018; 29: 268-275.e1 [PMID: 29203394 DOI: 10.1016/j.jvir.2017.08.021]
15 Ishikawa T,Higuchi K,Kubota T,Seki K,Honma T,Yoshida T,Kamimura T.Prevention of intrahepatic distant recurrence by transcatheter arterial infusion chemotherapy with platinum agents for stage I/II hepatocellular carcinoma.
2011; 117: 4018-4025 [PMID: 21365625 DOI: 10.1002/cncr.25989]
16 Chen HY,Lu SN,Hung CH,Wang JH,Chen CH,Yen YH,Kuo YH,Kee KM.Predicting outcomes for recurrent hepatocellular carcinoma within Milan criteria after complete radiofrequency ablation.
2020; 15: e0242113 [PMID: 33170894 DOI: 10.1371/journal.pone.0242113]
17 Cardella JF,Kundu S,Miller DL,Millward SF,Sacks D; Society of Interventional Radiology.Society of Interventional Radiology clinical practice guidelines.
2009; 20: S189-S191 [PMID: 19559998 DOI: 10.1016/j.jvir.2009.04.035]
18 Yuan C,Yuan Z,Cui X,Gao W,Zhao P,He N,Cui S,Wang Y,Zhang Y,Li W,Zheng J.Efficacy of ultrasound-,computed tomography-,and magnetic resonance imaging-guided radiofrequency ablation for hepatocellular carcinoma.
2019; 15: 784-792 [PMID: 31436232 DOI: 10.4103/jcrt.JCRT_836_18]
19 Lee LH,Hwang JI,Cheng YC,Wu CY,Lee SW,Yang SS,Yeh HZ,Chang CS,Lee TY.Comparable Outcomes of Ultrasound versus Computed Tomography in the Guidance of Radiofrequency Ablation for Hepatocellular Carcinoma.
2017; 12: e0169655 [PMID: 28068369 DOI: 10.1371/journal.pone.0169655]
20 Fahey BJ,Nelson RC,Hsu SJ,Bradway DP,Dumont DM,Trahey GE.In vivo guidance and assessment of liver radiofrequency ablation with acoustic radiation force elastography.
2008; 34: 1590-1603 [PMID: 18471954 DOI: 10.1016/j.ultrasmedbio.2008.03.006]
21 Kim JW,Shin SS,Heo SH,Hong JH,Lim HS,Seon HJ,Hur YH,Park CH,Jeong YY,Kang HK.Ultrasound-Guided Percutaneous Radiofrequency Ablation of Liver Tumors: How We Do It Safely and Completely.
2015; 16: 1226-1239 [PMID: 26576111 DOI: 10.3348/kjr.2015.16.6.1226]
22 Mendiratta-Lala M,Brook OR,Midkiff BD,Brennan DD,Thornton E,Faintuch S,Sheiman RG,Goldberg SN.Quality initiatives: strategies for anticipating and reducing complications and treatment failures in hepatic radiofrequency ablation.
2010; 30: 1107-1122 [PMID: 20442337 DOI: 10.1148/rg.304095202]
23 Li Z,Wang C,Si G,Zhou X,Li Y,Li J,Jiao D,Han X.Image-guided microwave ablation of hepatocellular carcinoma (≤5.0 cm): is MR guidance more effective than CT guidance?
2021; 21: 366 [PMID: 33827464 DOI: 10.1186/s12885-021-08099-7]
24 Liu B,Long J,Wang W,Huang T,Xie X,Chen S,Huang G,Jiang C,Ye J,Long H,Kuang M.Predictive factors of treatment outcomes after percutaneous ablation of hepatocellular carcinoma in the caudate lobe: a retrospective study.
2019; 19: 699 [PMID: 31311502 DOI: 10.1186/s12885-019-5881-0]
25 Yang Y,Chen Y,Zhang X,Xin Y,Wang Y,Li X,Fan Q,Zhou X,Ye F.Predictors and patterns of recurrence after radiofrequency ablation for hepatocellular carcinoma within up-to-seven criteria: A multicenter retrospective study.
2021; 138: 109623 [PMID: 33711573 DOI: 10.1016/j.ejrad.2021.109623]
26 Ni JY,Sun HL,Chen YT,Luo JH,Chen D,Jiang XY,Xu LF.Prognostic factors for survival after transarterial chemoembolization combined with microwave ablation for hepatocellular carcinoma.
2014; 20: 17483-17490 [PMID: 25516662 DOI: 10.3748/wjg.v20.i46.17483]
27 Wang L,Ke Q,Lin N,Huang Q,Zeng Y,Liu J.The efficacy of transarterial chemoembolization combined with microwave ablation for unresectable hepatocellular carcinoma: a systematic review and meta-analysis.
2019; 36: 1288-1296 [PMID: 31852267 DOI: 10.1080/02656736.2019.1692148]
28 Yang WZ,Jiang N,Huang N,Huang JY,Zheng QB,Shen Q.Combined therapy with transcatheter arterial chemoembolization and percutaneous microwave coagulation for small hepatocellular carcinoma.
2009; 15: 748-752 [PMID: 19222102 DOI: 10.3748/wjg.15.748]
29 Zaitoun MMA,Elsayed SB,Zaitoun NA,Soliman RK,Elmokadem AH,Farag AA,Amer M,Hendi AM,Mahmoud NEM,Salah El Deen D,Alsowey AM,Shahin S,Basha MAA.Combined therapy with conventional trans-arterial chemoembolization (cTACE) and microwave ablation (MWA) for hepatocellular carcinoma >3-<5 cm.
2021; 38: 248-256 [PMID: 33615957 DOI: 10.1080/02656736.2021.1887941]
30 Si ZM,Wang GZ,Qian S,Qu XD,Yan ZP,Liu R,Wang JH.Combination Therapies in the Management of Large (≥ 5 cm) Hepatocellular Carcinoma: Microwave Ablation Immediately Followed by Transarterial Chemoembolization.
2016; 27: 1577-1583 [PMID: 27103146 DOI: 10.1016/j.jvir.2016.02.014]
 World Journal of Gastrointestinal Oncology2022年9期
World Journal of Gastrointestinal Oncology2022年9期
- World Journal of Gastrointestinal Oncology的其它文章
- Nutrition deprivation affects the cytotoxic effect of CD8 T cells in hepatocellular carcinoma
- Prognostic and clinicopathological value of Twist expression in esophageal cancer:A meta-analysis
- Dissecting novel mechanisms of hepatitis B virus related hepatocellular carcinoma using meta-analysis of public data
- Prediction of gastric cancer risk by a polygenic risk score of Helicobacter pylori
- Percutaneous insertion of a novel dedicated metal stent to treat malignant hilar biliary obstruction
- Construction and analysis of an ulcer risk prediction model after endoscopic submucosal dissection for early gastric cancer