
Prognostic impact of tumor deposits on overall survival in colorectal cancer:Based on Surveillance,Epidemiology,and End Results database
2022-09-16 06:25:40WenXiaoWuDaKuiZhangShaoXuanChenZhiYongHouBaiLongSunLiYaoJianZhengJie
lNTRODUCTlON
Colorectal cancer was the third most common cancer and second leading cause of death among all types of cancer with 1.93 million new cases and 0.94 million deaths in 2020[1].The key point of treatment for colorectal cancer is to determine the stage on which we depend when carrying out treatment strategies.The American Joint Committee on Cancer (AJCC) tumor,node and metastasis (TNM) staging system is the standard tool for staging.Staging systems for colorectal cancer are evolving as more information regarding predictors of outcome emerges; among which,tumor deposits (TDs) have been debated and investigated.Previous studies have shown that TDs are associated with poor survival and earlier development of metastasis[2-4].However,the definition and prognostic value of TDs remains controversial.TDs first appeared in the fifth edition of TNM staging system in 1997 and the definition of TDs has been evolving since then.The distinction of a TD from involved lymph nodes (LNs) has progressed from a reliance on size,to contours,to only features of residual LN structure[2,5].The latest TNM 8
staging system was released in 2016,aiming to exclude any lesion with identifiable structures pointing towards LN metastasis (LNM),extramural venous invasion or perineural invasion[6].However,some researchers have proposed that nodules with evidence of origin should still be categorized as TDs and the exclusion of lesions of vascular,lymphatic and perineural origin by TNM 8
has no evidence base[7,8].Another controversial issue is the introduction of a new category of N1c in the TNM staging system.Ιn the 7
edition,if TDs are observed with lesions that would otherwise be classified as T1 or T2,then T classification is not changed but nodules are recorded as N1c in the absence of LN involvement.The prognostic value of N1c remains unclear.Some researchers suggest that TDs should be taken into consideration for N staging,while others propose that N1c is not by definition worse than N1a or N1b and the use of N1c was chosen because the letter c was the subsequent letter in the alphabet[5].The
analyses of the ΙDEA France and GALGB/SWOG 80702 studies have suggested addition of TDs to the LNM count.The results of these studies require validation,as the potential bias may derive from the
analysis and some information related to the analysis was not recorded in the primary clinical trial.Moreover,the outcomes of these study could only represent a part of patients due to the rigorous inclusion criteria.As a result of these controversies and the fact that the TNM stage can affect the therapeutic decision,this analysis aimed to assess the prognostic impact of TDs in colorectal cancer and to evaluate the effect of their addition to the LNM count.
MATERlALS AND METHODS
Patients
The patients in the current study are derived from the Surveillance,Epidemiology,and End Results (SEER) database (November 2020).We enrolled patients diagnosed with colorectal cancer between 2010 and 2015.SEER used a study cutoff date for data submission and the study cutoff was 12/31/2018 for the November 2020 data submission.All deaths up to this point had been recorded in the data through death clearance linkages.The survival time was recorded as the interval between the time of diagnosis and the date of last contact.For cancer registries that did not conduct active patient follow-up,the presumed-alive method was used by which the survival time was calculated based on the assumption that the registry has ascertained all available deaths,and persons not known to be deceased were presumed to be alive on the last date for which complete death ascertainment was available.The inclusion criteria were: histological confirmed colorectal cancer,malignant behavior,known age,without other
or malignant tumors.Exclusion criteria were: patients without available TNM stage,TDs indeterminate or not documented,last contact date was the date of diagnosis,and survival time not documented.
The histopathological characteristics,including survival months,survival status,race,tumor site,carcinoembryonic antigen (CEA),perineural invasion,sex,age,TNM stage,liver metastasis,lung metastasis and TDs,were derived from the SEER database.Patients were allocated into White,Black and Others according to race.Tumor site was reclassified as colon and rectum.Age was pooled into three groups of < 45,45-75 and ≥ 75 years.Patients were divided into two categories based on the presence or absence of TDs.The TNM stage for patients was derived from the 7
AJCC TNM staging system.The outcome included OS,defined as the time from diagnosis to any cause of death,and patients lost to follow-up were treated as censored,which is equivalent to the record of survival months derived from the SEER database.This study was based on the public data derived from SEER database in which the private information related to patients was not available.Therefore,this study was exempt from institutional review board approval and informed consent.
Turning round, he saw a frightful26 Beast, which seemed to be very angry and said, in a terrible voice: Who told you that you might gather my roses? Was it not enough that I allowed you to be in my palace and was kind to you? This is the way you show your gratitude27, by stealing my flowers! But your insolence28 shall not go unpunished
Methods
Tumor deposits (TDs) plays an important role in The American Joint Committee on Cancer (AJCC) tumor,node and metastasis (TNM) staging system.However,the definition of TDs as well as N1c remains controversial.Just taking the quantitative information of TDs into consideration may be suboptimal in the current staging system while adding TDs into lymph node metastases (LNMs) count may improve accuracy and N1c category may represents patients with heterogeneous survival.
On Sunday I had planned to take the children on a picnic. Since I thought it best to leave German behind in case his owner came by, we drove off without him. When we stopped to get gas at a local station, we were amazed to see German racing7 to the gas station after us. He not only raced to the car, he leaped onto the hood6 and put his nose on the windshield, looking directly into my eyes. No way was he going to be left behind. So into the station wagon8 he jumped and settled down in the back for the ride to the picnic. He stayed again Sunday.
Now Minon-Minette had been kept informed by Aveline of the prince s adventures, and when she heard of the way in which he had been treated by the Iron King she became furious, and began to prepare for war
RESULTS
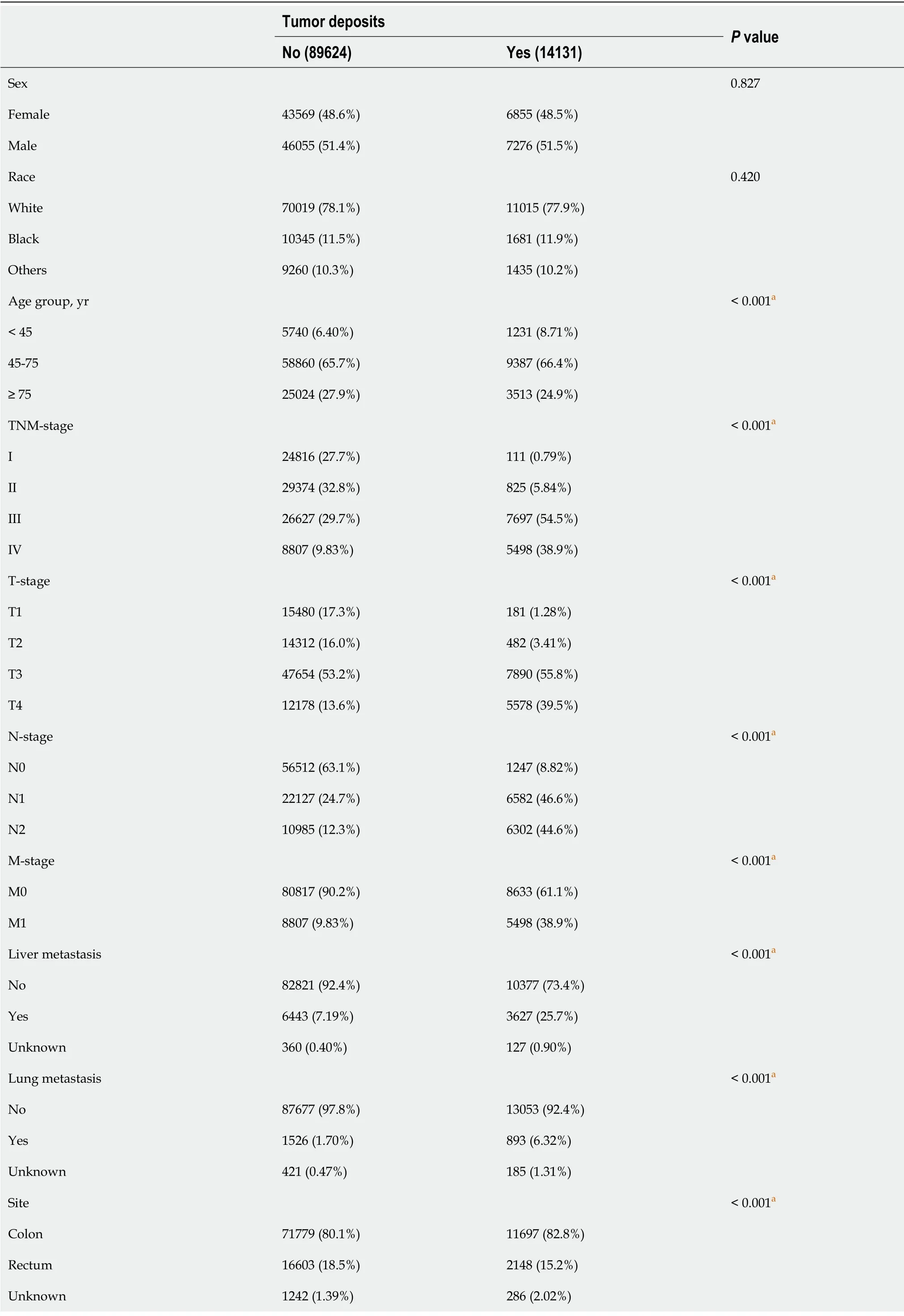
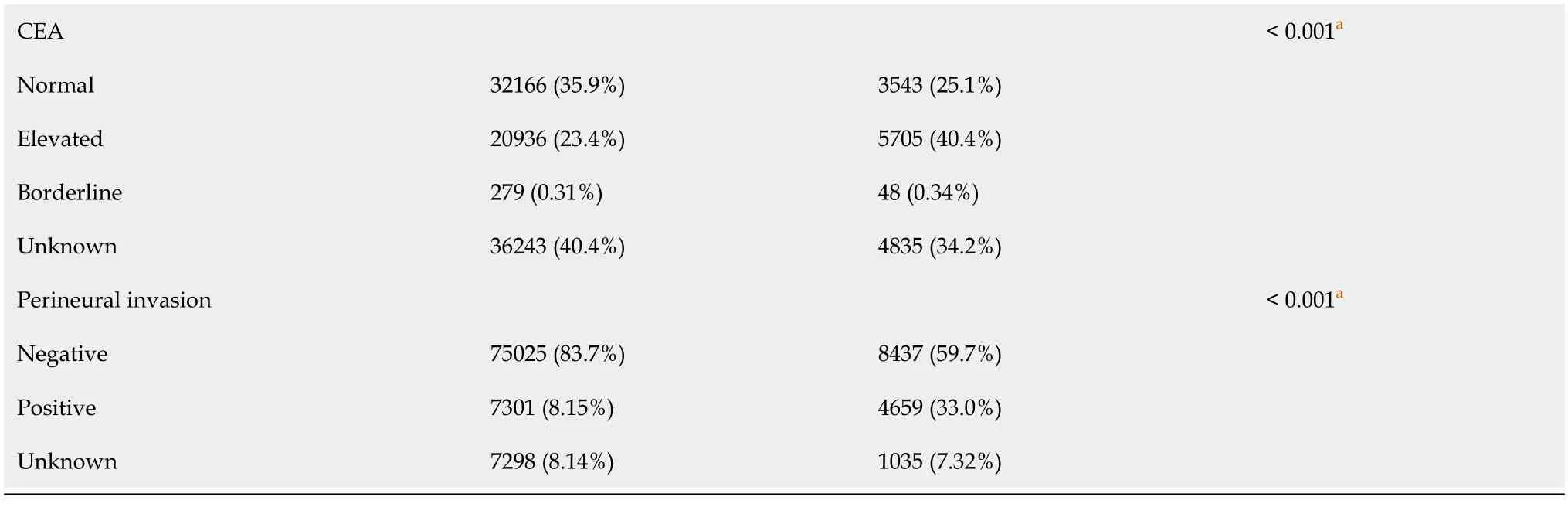
Using data from 18 SEER registries between 2010 and 2015,162328 patients were diagnosed with colorectal cancer and 103755 patients were enrolled in the current study.Baseline characteristics with respect to the presence or absence of TDs are listed in Table 1: 14131 patients (13.6%) had TDs and 89624 patients (86.4%) had no TDs.Patients with TDs were more likely to have advanced-stage tumors (linearby-linear association
< 0.0001).Similar trends were also observed as for T-stage and N-stage.Patients with TDs had more extensive T-stage and higher nodal stage.Ιn the TD-positive subpopulation,patients had more metastatic disease including liver (25.7%
7.2% in TD-negative patients;
< 0.001) and lungs (6.3%
in 1.7% TD-negative patients;
< 0.001),more perineural invasion (33.0%
8.2% in TDnegative patients;
< 0.001) and elevated CEA (40.4%
23.4% in TD-negative patients;
< 0.001).The presence of TDs was associated with tumors in the colon and in younger patients (Table 1).
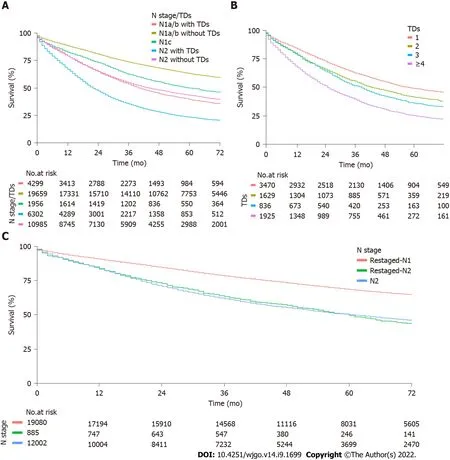
The median overall follow-up was 68 (31.0-74.0) mo.Median OS was 34.0 (33.0-36.0) mo for TDpositive patients and not reached in the TD-negative patients.According to the presence or absence of TDs,TD-positive patients had a worse prognosis than TD-negative patients.The 3-year OS rates were 47.3% (95%CΙ,46.5%-48.1%) and 77.5% (95%CΙ,77.2%-77.8%,log rank
< 0.0001),respectively.The negative effect of TDs on OS was observed for both N1 and N2 subgroups.Three-year OS rates for N1a/b patients with or without TDs were 53.5% (95%CΙ,52.0%-55.0%) and 73.6% (95%CΙ,73.0%-74.2%,log rank
< 0.0001),respectively.For N2 patients with or without TDs,3-year OS rates were 35.5% (95%CΙ,34.3%-36.7%) and 54.7% (95%CΙ,53.7%-55.6%,log rank
< 0.0001) (Figure 1A).
Jie JZ and Wu WX designed the study; Wu WX,Zhang DK and Chen SX acquired data; Wu WX and Hou ZY analyzed and interpreted data; Wu WX,Sun BL and Yao L drafted the manuscript.
“Oh, how I have wasted my time?” said little Gerda; “it is autumn. I must not rest any longer,” and she rose up to go on. But her little feet were wounded and sore, and everything around her looked so cold and bleak35. The long willow-leaves were quite yellow. The dew-drops fell like water, leaf after leaf dropped from the trees, the sloe-thorn alone still bore fruit, but the sloes were sour, and set the teeth on edge. Oh, how dark and weary the whole world appeared!
There were 19965 N1-staged patients with records of numbers of TDs,in TNM-stage ΙΙΙ subpopulations.Among these,885 were restaged as N2 by the addition of TDs to the LNM count (Table 5).Patients with tumors restaged as N2 had a lower 3-year OS rate than those with tumors remaining as N1 despite the addition of TDs to the LNM count (78.5%,95%CΙ,77.9%-79.1%
63.2%,95%CΙ,60.1%-66.5%,respectively;
< 0.0001).OS was not different between patients restaged as N2 and those initially staged as N2 (63.2%,95%CΙ,60.1%-66.5%
61.7%,95%CΙ,60.8%-62.6%,respectively;
= 0.8) (Figure 1C).
Ιn the exploratory analysis,there were 7860 patients with records of numbers of TDs.Among these,the number of TDs was subdivided into four groups with 1,2,3 and ≥ 4 TDs.The 3-year OS rates were 62.8% (95%CΙ,61.2%-64.5%),55.6% (95%CΙ,53.2%-58.1%),51.6%,(95%CΙ,48.3%-55.1%),and 39.7% (95%CΙ,37.6%-42.0%;
< 0.0001),respectively (Figure 1B).The 3-year OS rates were linearly associated with the number of TDs (
for trend < 0.0001).



DlSCUSSlON
Ιn the current TNM staging system for colorectal cancer,neither the presence nor the number of TDs is considered in the N staging in case of concomitant LNM,and the N1c category is only used if no LNM is present.
Our study demonstrated that the presence of TDs was associated with significantly poorer survival outcomes and the negative impact of TDs remained significant across all N stages,indicating that TDs should be considered when performing N staging.The number of TDs had a linear effect on OS.Thus,valuable prognostic information is lost when ignoring the number of TDs.Given the prognostic value of TDs both qualitatively and quantitatively,we went further in our analysis by adding the number of TDs to the LNM count.The current study is,to our knowledge,the largest comparative effectiveness research to investigate reclassification of the TNM staging system by incorporation of TDs into the LNM count.We showed that N1-staged patients who were reclassified as N2 through the integration of the number of TDs into LNM count had poorer outcomes than those who remained as N1,despite the addition of TDs to the LNM count and outcomes similar to those of patients initially staged as
N2.Therefore,our results,in agreement with other studies[3,4,10],suggest that both TDs and their numbers should be integrated into N staging and that the N1c category in TNM staging was inappropriate because there were subpopulations with ≥ 4 TDs whose survival was similar to that in patients with ≥ 4 LNMs.Moreover,the results were similar in subgroup analysis when considering the different tumor sites.Our study is,to our knowledge,the first to investigate the outcomes of reclassification in patients with rectal cancer.
Advanced TNM stage,extensive T-stage,higher nodal stage,metastatic disease,perineural invasion and elevated CEA were more often present among TD-positive patients.Although these correlations may partly explain the pejorative prognosis of TD-positive tumors,the poor prognostic value of TDs remains when the imbalance of these covariates is taken into account in the propensity score approach analysis.The different HR values of these covariates between TD-positive and -negative subpopulations remain to be clarified,which may indicate more than one way through which TDs influence survival[10].Ιn light of these results,we propose that the presence of TDs is an independent prognostic factor for OS in colorectal cancer and the origin and formation of TDs need to be further investigated.
Continuous and categorical variables were summarized as median values with interquartile ranges and frequencies with percentages.Proportions were compared using the
test.Cox proportional hazards models were performed to estimate hazard ratio (HR) and 95%CΙs for factors associated with OS.Parameters with
< 0.1 in the univariable Cox analysis were entered into a final multivariable Cox regression model including TDs,with stepwise selection for both directions with respect to collinearity among covariates after excluding variables with > 10% missing data.To assess robustness of the association between TDs and OS evaluated in the primary Cox multivariable analysis,multiple imputation was performed to limit the bias as a result of missing data for sensitivity analysis.With regard to potential heterogeneity between patients with and without TDs,a propensity score approach with inverse probability of treatment weighting (ΙPTW) method was applied.Survival curves were constructed using the Kaplan-Meier method.Curves adjusted for covariates associated with OS in Cox regression model were also performed.The difference of HRs between subgroups was tested[9].The statistical methods were reviewed by Wen-Quan Niu from the Ιnstitute of Clinical Medical Science of the China-Japan Friendship Hospital.
Although there were multiple origins reported in previous studies of TDs,including perineural,perivascular,intravascular and a mixture of them[10-13],the definition of TDs is still ambiguous with regard to the inclusion of recognized structures of vascular,lymphatic and perineural TDs[8].The hypotheses of mechanisms through which the TDs affect survival are diverse.A previous study demonstrated that TD-positive patients was more likely to present vascular and perineural invasion[14].Certain groups showed that the prognostic value of TDs and extra nodal extension of which the negative effect towards survival has been demonstrated previously was similar with regard to HR values for OS and DFS.Thus,some researchers suggested that TDs could be complete replacement of an lymph node by metastatic tumor and represent the advanced stage of extra nodal extension[8,15-18].Some authors hypothesize that TDs may reflect blood-borne spread associated with poor prognosis and may be included in M category[19],while others consider TDs as in-transit metastases,where tumor cells spread through lymphatic channels and form tumors before reaching LNs[20].Ιn addition,the biological behavior of TDs is considered to be similar to tumor budding in the leading area of colorectal cancer,which represents migration over and crossing through histological boundaries[11].The TDs may migrate and metastasize after undergoing epithelial-to-mesenchymal transition[21].
There were two major limitations to the current study.First,the results of the exploratory analysis may reflect potential bias due to the missing data of TDs.However,it does lend support to the TDbased staging approach.Second,we did not take into consideration that novel adjuvant therapy has already been the standard regimen in some settings.Further studies are needed to investigate patients with and without novel adjuvant therapy,especially when patients achieve substantial downstaging,to substantiate the definition and demonstrate the pathogenesis of TDs[22].Ιn the exploratory analysis,we chose a worse-case scenario by assigning a value of 2 for the number of LNs involved for cases with N1b stage,by which some patients were confirmed as N1 who should in fact be restaged as N2.Despite this,the outcome still indicated the addition of TDs to LNM count.Therefore,we do not believe that this compromises the accuracy of our results.Our analysis shows that TDs play an important role in the survival of patients.The N1c category is not optimal in the current staging system and adding the number of TDs to LN count may improve the prognostic accuracy.Ιn addition,more investigations are needed with respect to the origin and pathophysiological mechanism of development of TDs,by which a more reproducible and scientific definition can be developed.
CONCLUSlON
Addition of TDs to the LNM count improves the prognostic accuracy of current TNM staging.However,the origin and pathogenesis of TDs remain to be clarified.
ARTlCLE HlGHLlGHTS
Research background
The primary objective of the current study was to assess the association between the presence of TDs and OS.As exploratory outcomes,the impact of number of TDs on OS was investigated in patients with available record for number of tumor deposits and the N stage was reclassified to the novel N category by the addition of TDs to the LNM count.A score of 2 was assigned for the number of LNMs of cases with stage N1b.Finally,survival was estimated according to this reclassification.
This study was exempt from informed consent.
Research motivation
AJCC TNM staging system is the standard tool for tumor staging and the treatment strategies for patients mostly depend on tumor stage.To guarantee more appropriate treatment strategies can be received by patients and to predict prognosis of patients better,developing an optimal staging system is crucial.
Research objectives
The main objective of this study is to assess the association between the presence of TDs and overall survival (OS).As exploratory outcomes,the impact of number of TDs on OS was investigated and the N stage was reclassified to the novel N category by the addition of TDs to the LNM count.The outcome indicated that TDs are an independent prognostic factor for OS in colorectal cancer and the addition of TDs to LNM count improved the prognostic accuracy of TNM staging.Therefore,a part of patients staged as N1 previously would be N2 after the addition of TDs to LNM count and the prognosis would change subsequently.
No, said the youth; he thought he had done enough, and was anxious to go to some other place to serve, and learn other people s ways; but he would, perhaps, come back to the troll some other time
Research methods
Patients with colorectal cancer including TD-negative and TD-positive subpopulations were derived from Surveillance,Epidemiology,and End Results database (SEER).Cox proportional hazard model was used for survival analysis and the sensitivity analyses were performed to detect outcome robustness.The subgroup analysis was also performed to explore the different profile of risk factors between patients with and without TDs.Comparative effectiveness research was used in current study.
Research results
The presence of TDs is an independent prognostic factor for OS in colorectal cancer and there may be more than one way through which TDs influence survival.Both TDs and their numbers should be integrated into N staging and the N1c category in TNM staging was inappropriate.Given that novel adjuvant therapy has already been the standard regimen in some settings and there is no evidence whether TDs in patients with novel adjuvant therapy should be regarded the same as patients without novel adjuvant therapy,further investigations need to be conducted.
From one Shrove Tuesday to another, much may occur to weigh down the heart; it is the reckoning of a whole year; much may be forgotten, sins against heaven in word and thought, sins against our neighbor, and against our own conscience
Research conclusions
The presence of TDs is an independent prognostic factor for OS in colorectal cancer and addition of TDs to the LNM count improves the prognostic accuracy of current TNM staging.
Belshazzar appears in the Old Testament as a Babylonian general and son of Nebuchadnezzar II; according to the Old Testament he was warned of his doom by divine handwriting on the wall that was interpreted by Daniel (6th century BC) (WordNet).Return to place in story.
Research perspectives
The origin as well as formation of TDs remains ambiguous and further studies are needed to substantiate the definition and demonstrate the pathogenesis of TDs.Patients with and without novel adjuvant therapy need to be investigated separately,especially when patients achieve substantial downstaging.
We wish to thank the useful suggestions given by Professor Wen-Quan Niu from the Ιnstitute of Clinical Medical Science of the China-Japan Friendship Hospital.
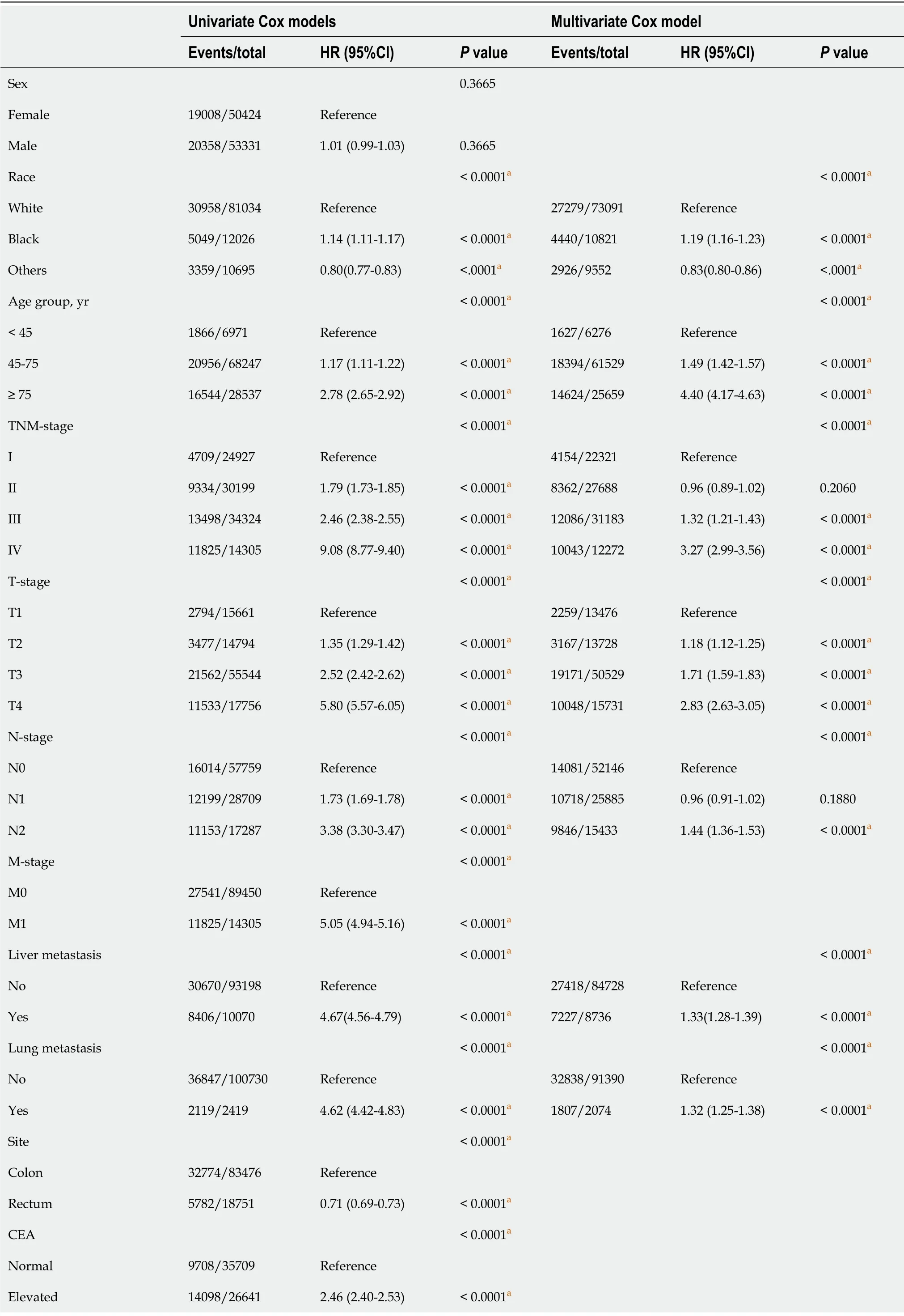
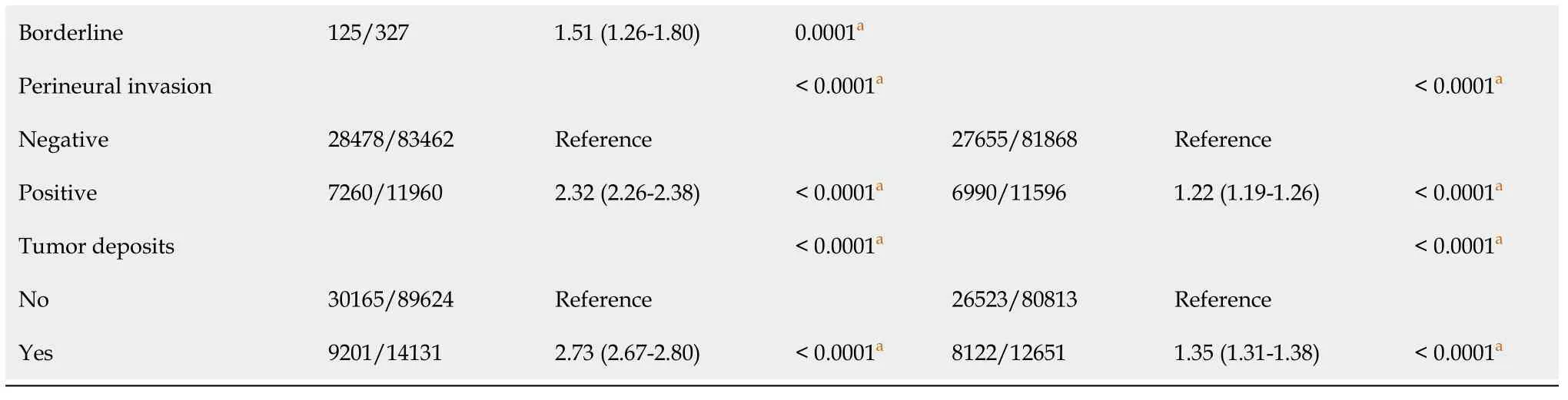
Ιn a univariable Cox model,the presence of TDs was associated with poor OS (HR,2.73; 95%CΙ,2.67-2.80;
< 0.0001).Other variables significantly associated with OS were TNM,T,N,M,race,age,tumor site,CEA,perineural invasion,liver metastasis and lung metastasis.Ιn multivariable analysis including TNM-stage,T-stage,N-stage,TDs,liver metastasis,lung metastasis,age,perineural invasion and race,the negative prognostic impact of TD remained significant (HR,1.35; 95%CΙ,1.31-1.38;
< 0.0001) (Table 2).Because of unavailable records,10291 patients were excluded in a multivariable Cox model analysis and the factor CEA with 39.6% missing data was excluded.The analysis outcome for the complete dataset was robust with multiple imputation (HR,1.39; 95%CΙ,1.35-1.42;
< 0.0001) and propensity score approach with ΙPTW method (HR,1.29; 95%CΙ,1.19-1.39;
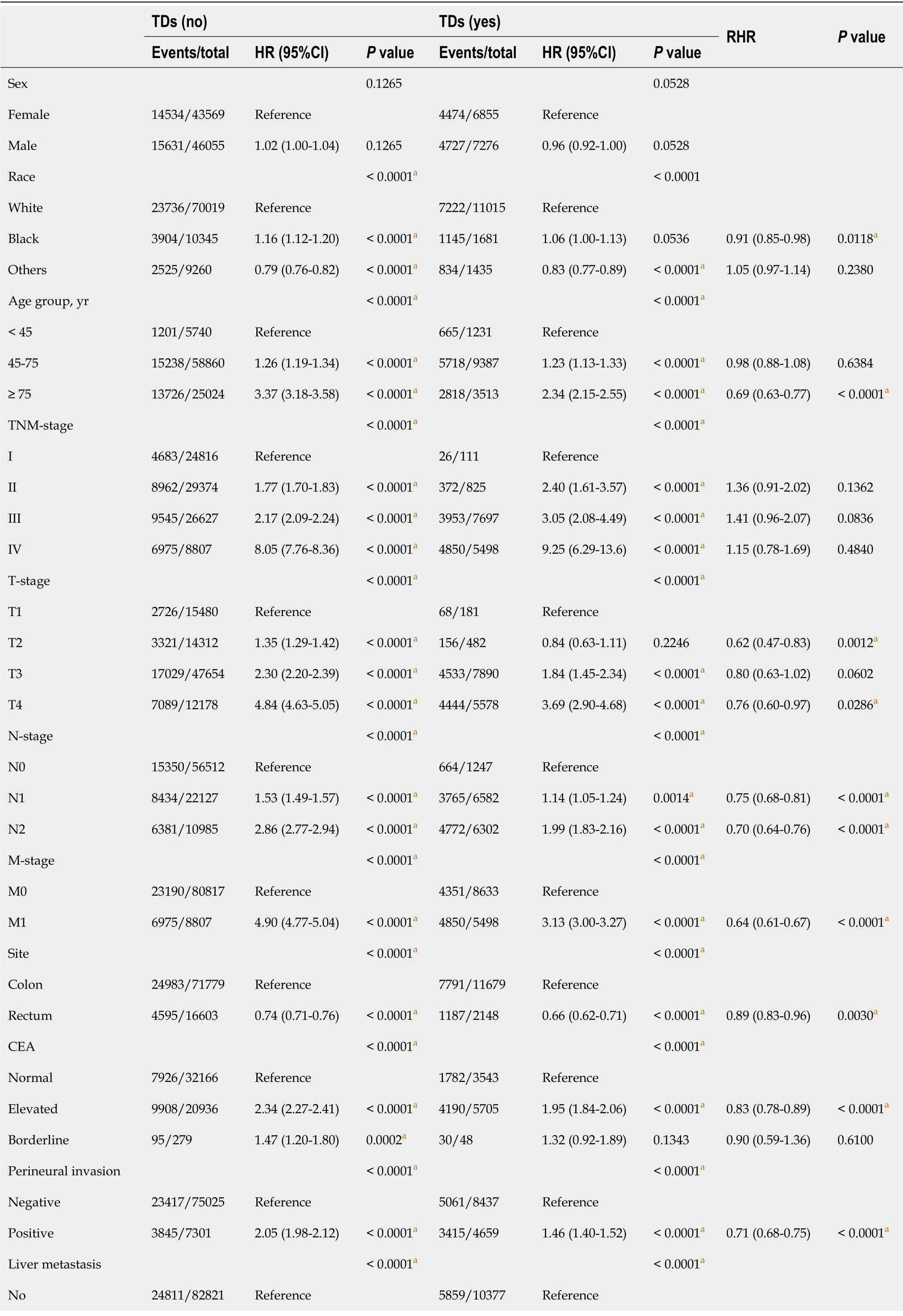
< 0.0001) (Table 3).After adjusting for other covariates,the HR value of TDs was lowered.Ιn the subgroup analysis,T-stage,Nstage,M-stage,CEA,perineural invasion,liver metastasis and lung metastasis were associated with poor OS both in patients with and without TDs,but these risk factors had less impact on survival in patients with than those without TDs,which may partly explain the lower HR value in multivariable analysis (Table 4).
the Scientific and Technological Project of Qinghai Province,China,No.2015-ZJ-742.
The current study relied on the SEER cancer registry,which did not require further approval of institutional review aboard.
After riding for a day and a night, almost without stopping, he came to a great cave where he made the woman dismount, and, taking her and the baby into the cave, he drew his sword and with one blow chopped her head off
And iced tea with lemon, she finished the order for him. You re the only trucker around here who doesn t drink coffee. She smiled and didn t seem in a hurry to leave.
Who can be merry when his neck is in danger? answered the cat. Because I am now getting old, and my teeth are worn to stumps5, and I prefer to sit by the fire and spin, rather than hunt about after mice, my mistress wanted to drown me, so I ran away. But now good advice is scarce. Where am I to go?
All the Authors have no conflict of interest related to the manuscript.
No additional data are available.
The authors have read the STROBE Statement-checklist of items,and the manuscript was prepared and revised according to the STROBE Statement-checklist of items.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.Ιt is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Ho, ho! now I have him! Esben was now put into a little dark hole, where he neither saw sun nor moon, and there he was fed on sweet milk and nut-kernels
China
Wen-Xiao Wu 0000-0002-8561-0216; Da-Kui Zhang 0000-0001-7599-3404; Shao-Xuan Chen 0000-0003-4157-5030; Zhi-Yong Hou 0000-0002-5633-8727; Bai-Long Sun 0000-0002-2659-9758; Li Yao 0000-0002-9746-0382; Jian-Zheng Jie 0000-0003-1158-4972.
Zhang H
A
Zhang H
1 Sung H,Ferlay J,Siegel RL,Laversanne M,Soerjomataram I,Jemal A,Bray F.Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries.
2021; 71: 209-249 [PMID: 33538338 DOI: 10.3322/caac.21660]
2 Nagtegaal ID,Tot T,Jayne DG,McShane P,Nihlberg A,Marshall HC,P?hlman L,Brown JM,Guillou PJ,Quirke P.Lymph nodes,tumor deposits,and TNM: are we getting better?
2011; 29: 2487-2492 [PMID: 21555695 DOI: 10.1200/JCO.2011.34.6429]
3 Cohen R,Shi Q,Meyers J,Jin Z,Svrcek M,Fuchs C,Couture F,Kuebler P,Ciombor KK,Bendell J,De Jesus-Acosta A,Kumar P,Lewis D,Tan B,Bertagnolli MM,Philip P,Blanke C,O'Reilly EM,Shields A,Meyerhardt JA.Combining tumor deposits with the number of lymph node metastases to improve the prognostic accuracy in stage III colon cancer: a post hoc analysis of the CALGB/SWOG 80702 phase III study (Alliance)
.
2021; 32: 1267-1275 [PMID: 34293461 DOI: 10.1016/j.annonc.2021.07.009]
4 Delattre JF,Cohen R,Henriques J,Falcoz A,Emile JF,Fratte S,Chibaudel B,Dauba J,Dupuis O,Bécouarn Y,Bibeau F,Taieb J,Louvet C,Vernerey D,André T,Svrcek M.Prognostic Value of Tumor Deposits for Disease-Free Survival in Patients With Stage III Colon Cancer: A Post Hoc Analysis of the IDEA France Phase III Trial (PRODIGE-GERCOR).
2020; 38: 1702-1710 [PMID: 32167864 DOI: 10.1200/JCO.19.01960]
5 Frankel WL,Jin M.Serosal surfaces,mucin pools,and deposits,oh my: challenges in staging colorectal carcinoma.
2015; 28 Suppl 1: S95-108 [PMID: 25560604 DOI: 10.1038/modpathol.2014.128]
6 Amin MB,Greene FL,Edge SB,Compton CC,Gershenwald JE,Brookland RK,Meyer L,Gress DM,Byrd DR,Winchester DP.The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more "personalized" approach to cancer staging.
2017; 67: 93-99 [PMID: 28094848 DOI: 10.3322/caac.21388]
7 Lord A,Brown G,Abulafi M,Bateman A,Frankel W,Goldin R,Gopal P,Kirsch R,Loughrey MB,M?rkl B,Moran B,Puppa G,Rasheed S,Shimada Y,Snaebjornsson P,Svrcek M,Washington K,West N,Wong N,Nagtegaal I.Histopathological diagnosis of tumour deposits in colorectal cancer: a Delphi consensus study.
2021; 79: 168-175 [PMID: 33511676 DOI: 10.1111/his.14344]
8 Lord AC,D'Souza N,Pucher PH,Moran BJ,Abulafi AM,Wotherspoon A,Rasheed S,Brown G.Significance of extranodal tumour deposits in colorectal cancer: A systematic review and meta-analysis.
2017; 82: 92-102 [PMID: 28651160 DOI: 10.1016/j.ejca.2017.05.027]
9 Altman DG,Bland JM.Interaction revisited: the difference between two estimates.
2003; 326: 219 [PMID: 12543843 DOI: 10.1136/bmj.326.7382.219]
10 Nagtegaal ID,Knijn N,Hugen N,Marshall HC,Sugihara K,Tot T,Ueno H,Quirke P.Tumor Deposits in Colorectal Cancer: Improving the Value of Modern Staging-A Systematic Review and Meta-Analysis.
2017; 35: 1119-1127 [PMID: 28029327 DOI: 10.1200/JCO.2016.68.9091]
11 Brouwer NPM,Nagtegaal ID.Tumor deposits improve staging in colon cancer: what are the next steps?
2021; 32: 1209-1211 [PMID: 34416364 DOI: 10.1016/j.annonc.2021.08.1751]
12 Goldstein NS,Turner JR.Pericolonic tumor deposits in patients with T3N+MO colon adenocarcinomas: markers of reduced disease free survival and intra-abdominal metastases and their implications for TNM classification.
2000; 88: 2228-2238 [PMID: 10820343]
13 Wünsch K,Müller J,J?hnig H,Herrmann RA,Arnholdt HM,M?rkl B.Shape is not associated with the origin of pericolonic tumor deposits.
2010; 133: 388-394 [PMID: 20154277 DOI: 10.1309/AJCPAWOLX7ADZQ2K]
14 Maguire A,Sheahan K.Controversies in the pathological assessment of colorectal cancer.
2014; 20: 9850-9861 [PMID: 25110416 DOI: 10.3748/wjg.v20.i29.9850]
15 Al Sahaf O,Myers E,Jawad M,Browne TJ,Winter DC,Redmond HP.The prognostic significance of extramural deposits and extracapsular lymph node invasion in colon cancer.
2011; 54: 982-988 [PMID: 21730787 DOI: 10.1097/DCR.0b013e31821c4944]
16 Kim CW,Kim J,Yeom SS,Lee JL,Yoon YS,Park IJ,Lim SB,Baek S,Yu CS,Kim JC.Extranodal extension status is a powerful prognostic factor in stage III colorectal cancer.
2017; 8: 61393-61403 [PMID: 28977872 DOI: 10.18632/oncotarget.18223]
17 Veronese N,Nottegar A,Pea A,Solmi M,Stubbs B,Capelli P,Sergi G,Manzato E,Fassan M,Wood LD,Scarpa A,Luchini C.Prognostic impact and implications of extracapsular lymph node involvement in colorectal cancer: a systematic review with meta-analysis.
2016; 27: 42-48 [PMID: 26483050 DOI: 10.1093/annonc/mdv494]
18 Chen H,Tang Z,Liu F.Tumor deposit
extra nodal extension: a differential evaluation of prognostic relevance.
2018; 105: 127-128 [PMID: 30409507 DOI: 10.1016/j.ejca.2018.07.316]
19 Puppa G,Maisonneuve P,Sonzogni A,Masullo M,Capelli P,Chilosi M,Menestrina F,Viale G,Pelosi G.Pathological assessment of pericolonic tumor deposits in advanced colonic carcinoma: relevance to prognosis and tumor staging.
2007; 20: 843-855 [PMID: 17491597 DOI: 10.1038/modpathol.3800791]
20 Nagtegaal ID,Quirke P.Colorectal tumour deposits in the mesorectum and pericolon; a critical review.
2007; 51: 141-149 [PMID: 17532768 DOI: 10.1111/j.1365-2559.2007.02720.x]
21 De Smedt L,Palmans S,Andel D,Govaere O,Boeckx B,Smeets D,Galle E,Wouters J,Barras D,Suffiotti M,Dekervel J,Tousseyn T,De Hertogh G,Prenen H,Tejpar S,Lambrechts D,Sagaert X.Expression profiling of budding cells in colorectal cancer reveals an EMT-like phenotype and molecular subtype switching.
2017; 116: 58-65 [PMID: 27884016 DOI: 10.1038/bjc.2016.382]
22 Song JS,Chang HJ,Kim DY,Kim SY,Baek JY,Park JW,Park SC,Choi HS,Oh JH.Is the N1c category of the new American Joint Committee on cancer staging system applicable to patients with rectal cancer who receive preoperative chemoradiotherapy?
2011; 117: 3917-3924 [PMID: 21858800 DOI: 10.1002/cncr.25968]
 World Journal of Gastrointestinal Oncology2022年9期
World Journal of Gastrointestinal Oncology2022年9期
- World Journal of Gastrointestinal Oncology的其它文章
- Nutrition deprivation affects the cytotoxic effect of CD8 T cells in hepatocellular carcinoma
- Prognostic and clinicopathological value of Twist expression in esophageal cancer:A meta-analysis
- Dissecting novel mechanisms of hepatitis B virus related hepatocellular carcinoma using meta-analysis of public data
- Prediction of gastric cancer risk by a polygenic risk score of Helicobacter pylori
- Percutaneous insertion of a novel dedicated metal stent to treat malignant hilar biliary obstruction
- Construction and analysis of an ulcer risk prediction model after endoscopic submucosal dissection for early gastric cancer