
Learning curve for a surgeon in robotic pancreaticoduodenectomy through a “G”-shaped approach: A cumulative sum analysis
2022-06-23 06:27:38ZhiGangWeiChaoJieLiangYangDuYongPingZhangYuLiu
World Journal of Clinical Cases 2022年14期
lNTRODUCTlON
Pancreaticoduodenectomy (PD) is one of the most difficult abdominal surgical procedures[1], as it involves a large range of resections and there is a need to complete the tumor-free, vascular skeletal, gastrointestinal, pancreaticojejunostomy, and biliary anastomosis during the operation. Therefore, the rate of complications in PD is high. In recent years, laparoscopic techniques have been widely used. Since the first report of laparoscopic PD (LPD) in 1994[2], an increasing number of people have investigated its postoperative efficacy, but the mortality rate was as high as 30% in early reports[3]. With the improvement in perioperative management and surgical skills, the mortality rate decreased significantly to 2% in large sample center reports, but the incidence of complications, such as pancreatic fistula, bleeding, and delayed gastric emptying, was more than 30%. During the treatment of tumors around the head of the pancreas or ampulla, the mortality associated with LPD was almost five times higher than that after open surgery, and there was no significant difference in the recovery time between the two groups. Furthermore, a meta-analysis comparing open PD (OPD) and LPD indicated that LPD has no advantage over OPD[4], and new research[5] on LPD suggested that even when LPD is conducted by a well-trained pancreatic surgeon who has performed at least 20 surgeries, there is an increased risk and no significant benefit.
The robot system has developed rapidly in recent years. Compared with the laparoscopic system, the robot system has a tremor filter system, a 3D high-definition zoom lens, and 7 free arms. As a result, robot-assisted surgery is a complicated operation that is associated with a fine operation and anatomical difficulty. In 2003, Giulianotti
[6] reported for the first time that PD was performed using the Da Vinci robotic surgery system, and this procedure has since made great progress. A meta-analysis[7] showed that robotic PD (RPD) is associated with fewer intraoperative abdominal hemorrhages and a shorter postoperative hospital stay compared to OPD, although the operation time (OT) is longer.
However, RPD is a very complicated operation, and surgeons are worried about its long learning curve. Zhang
[8] reported that RPD was a safe and effective operation in 100 cases of RPD surgery, and the learning curve was ultimately completed after 40 cases. The last 60 cases that underwent RPD had significantly less OT, hospitalization time, intraoperative bleeding, and fewer perioperative complications, such as hemorrhage, pancreatic fistula, reoperation rate, and delayed gastric emptying, compared to the first 40 cases. Napoli
[9] studied the perioperative data of 70 patients treated with RPD and found that the OT was significantly shortened after 33 cases. Boone
[10] found that after completing 20 RPD procedures, the learning curve improved significantly in terms of bleeding volume and conversion to open surgery; after 40 cases, the pancreatic surgery rate was decreased; and after 80 cases, the OT was shortened. However, the overall learning curve is still much longer than that of OPD. Moreover, the sample size of RPD surgery in single-center studies is small, and some physicians may not have any experience in robotic surgery in the early stage. There is an increase in the length of the learning curve; therefore, it should be considered whether this difficulty can be overcome through relatively simple surgical paths. Thus, the current study aims to analyze the learning curve of the Gpath in RPD and provide some new methods for shortening the RPD learning curve.
What a pretty figure I should cut if I went back into the world! But as he was still hungry, and the mischief44 was done, he climbed boldly up another tree, and plucked two plums of a lovely green colour
MATERlALS AND METHODS
Patients
A total of 60 patients who underwent a “G”-shaped surgical approach for RPD from May 2017 to April 2020 in the First Hospital of Shanxi Medical University were included in this study. Patients with obstructive jaundice were given intervention measures to improve their liver function before surgical treatment. Patients were included in this study if they met the following criteria: (1) Patients diagnosed with a benign or low-malignant tumor of the pancreatic head, early ampullary and periampullary tumor, pancreatic head cancer with T1/T2 stage (less than 3 cm in diameter), common bile duct carcinoma, duodenal papillary carcinoma based on abdominal computed tomography or magnetic resonance cholangiopancreatography examination; (2) Patients without mesenteric vascular invasion; (3) Patients without distant metastasis; (4) American Society of Anesthesiologists grade I/II/ III; and (5) Patients who could tolerate the surgery. Patients were excluded if one of the following conditions was present: (1) Distant metastasis (including celiac trunk and/or abdominal aorta); (2) Tumor encasement of the superior mesenteric artery (SMA) or celiac artery; (3) SMA/photovoltaic occlusion; (4) Surrounded aorta or inferior vena cava invasion; and (5) SMA invasion below the transverse mesocolon. This study was approved by the ethics committee of the First Hospital of Shanxi Medical University. The patients had a good understanding of the study, and they signed the informed consent form.
Surgical procedure
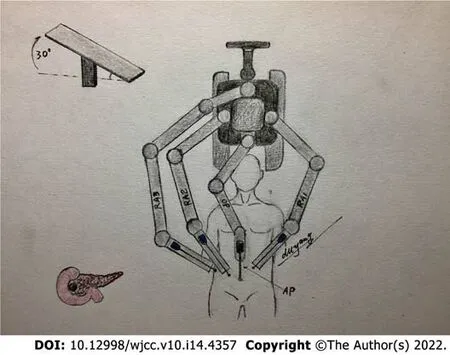
After anesthesia and tracheal cannulation, the patients were placed in the supine small position and their legs were placed in a split position. “Five trocars” in the shape of the letter “V” were used for the surgical incision, and the position of the trocars and patients are shown in Figures 1 and 2, respectively. The surgical assistant stood on the left side of the patient. A laparoscope was placed into the abdominal cavity through an incision at the inferior navel ring edge, with a pneumoperitoneum of 12 mmHg pressure (1 mmHg = 0.133 kPa). The remaining trocars were also placed in their appropriate positions under direct vision according to Figure 1, and the #1, #2, and #3 robotic arms were connected to the laparoscopic instrument. Laparoscopy was conventionally used to probe the liver, abdominal cavity, omentum majus, and other organs to identify whether there was a tumor, knot, or metastasis.

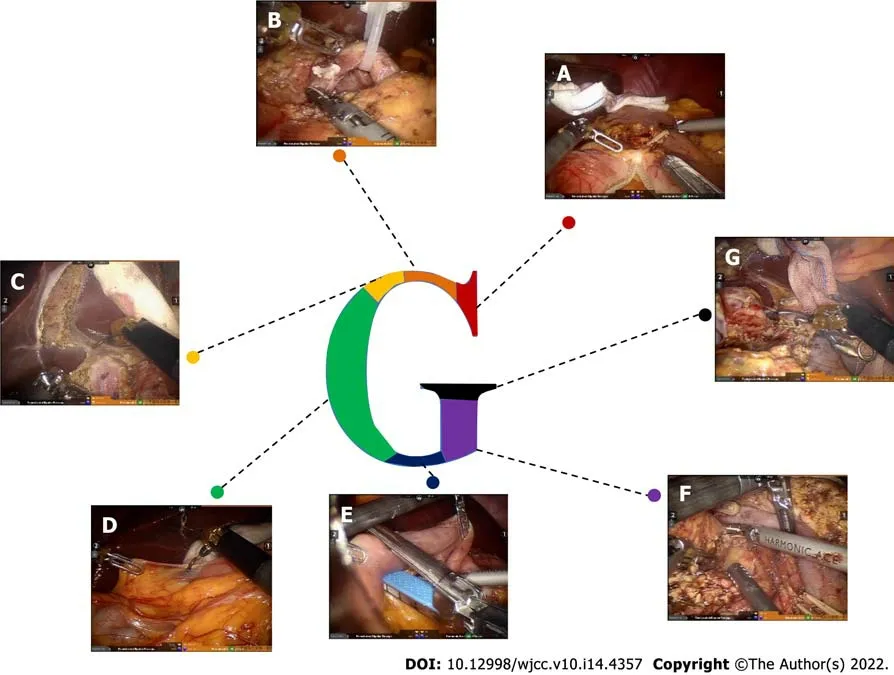
Step 1 (Figure 3A): The omentum and transverse ligament were isolated using an intestinal or stomach clamp and dissected using an ultrasonic knife. The dorsal pancreatic membrane was carefully exposed, the right gastroepiploic vein and artery were ligated, the small omentum was freed, and the gastric antrum was lifted and cut off with the Endo-GiA cutting closure. The partial stomach was isolated for the gastrojejunal anastomosis later.
Step 2 (Figure 3B): The gastric antrum was turned to the left side to expose the common hepatic artery, hepatic artery, hepatoduodenal ligament, and gastroduodenal artery. The surrounding loose tissues and lymph nodes were thoroughly cleaned. Then, the common hepatic artery was suspended, the gastroduodenal artery was ligated, and 8 pairs of lymph nodes near the proximal end of the common hepatic artery were cleaned. The portal vein in the posterior part was exposed, and 12 pairs of lymph nodes on the left front of the hepatoduodenal ligament were cleaned along the hepatic artery and the common bile duct. The superior mesenteric vein was separated and exposed along the inferior margin of the pancreas.
I left the party early, but not before Nancy had said, You ll come over to my house sometime, won t you? and Elaine had confided26, I get goosebumps every time Mr. Allen is our substitute teacher. Don t you? I didn t want to stay and dance-the boys heads came only to the middle of my chest. But on my way home, I decided that Parker was right. A deserted27 island would be pretty awful. I waited up for Parker that night. I wanted to hear about the fun I d missed. Did you dance a lot? I asked. Sort of, he said. If you think it s any fun for a fifthgrade guy to dance with a bunch of puny28 third- and fourth-graders! He kicked at the fringe on the rug and started up the stairs. Oh, I almost forgot, he said. Here s your two tickets. Thanks. It s going to be a double feature. One s The Wizard o f Oz. Ray Bolger plays a scarecrow. He had reached the fourth step. We stood eye to eye.
The cards I bought, Topps, still included a piece of gum, unlike many of the newer brands. The smell of the gum, the cardboard, the ink, and the wax paper brought the baseball memories of my youth rushing back as surely as did that first whiff of mown grass in the spring. I flipped2 through the cards, recognized a few of the players names, and then put them away.
Step 3 (Figure 3C): The cystic duct and the common bile duct were isolated using an ultrasonic scalpel, the cystic duct and the cystic artery were closed and isolated, and the gallbladder was dissected from the gallbladder bed. The bile duct was freed and temporarily suspended with a vascular sling to reduce bile contamination.
Step 4 (Figure 3D): The Kocher incision was performed, and the inferior vena cava and the left renal vein were exposed. The ascending part of the duodenum was completely freed at the posterior part of the vascular roots in the mesentery.
Step 5 (Figure 3E): The jejunum was cut off at a distance of 15 cm from the ligament of Treitz by a linear cutting closure. An ultrasonic scalpel was used to dissect the jejunum and the duodenum to free the proximal jejunum completely and push the freed proximal jejunum to the right side.
Step 6 (Figure 3F): The superior mesenteric vein was separated along the inferior margin of the pancreas under direct vision. The small branch of the vein originating from the superior mesenteric vein and portal vein was carefully clamped until the upper edge of the pancreas, and the pancreatic neck tunnel was successfully established. The pancreatic neck was transected on the left side of the superior mesenteric vein, and the pancreas section was carefully stopped. Subsequently, the duodenal end was pulled to the upper right, the superior mesenteric vein and the portal vein were suspended, and the SMA was fully exposed. The pancreatic neck was isolated on the left side of the superior mesenteric vein or portal vein, and the pancreatic duct was cut off with scissors. An ultrasound knife was used to stop bleeding at the cut end of the pancreas. Furthermore, the ascending part of the duodenum and proximal jejunum were pulled from the rear side of the superior mesenteric vein root to the upper right, and then the duodenal end was pulled to the upper right to increase the distance from the pancreatic sulcus to the superior mesenteric vein and portal vein. The superior mesenteric vein was suspended and pulled to the left of the SMA with a vascular band. The SMA and its right branches were then double dissected from the bottom up with biological clips. The pancreatic uncinate process membrane was detached along the right side of the SMA to ensure complete removal of the uncinate process.
Also note that this princess must prove her nobility through her physical sensitivity, not through her ability to fit a ring or slipper16 like her Donkeyskin and Cinderella counterparts. The test is a physical one, but quite unlike the other well-known tests of fitting into articles of clothing.Return to place in story.
Step 7 (Figure 3G): The common hepatic duct above the confluence of the cystic duct and the common bile duct was transected to clearly expose the portal vein. Then, lymph node dissection was conducted on the right and rear sides of the hepatoduodenal ligament and behind the common liver artery, and, using this simple and complicated way to remove each tissue, the shape achieved was a G-type.
According to the CUSUM analysis, the learning curve for GRPD was grouped into two phases (early and late phases). The OT was 480 ± 81.65 min
331 ± 76.54 min, hospitalization time was 22 ± 4.53 d
17 ± 6.08 d, and blood loss was 308 ± 54.78 mL
169.2 ± 35.33 mL in the respective groups. The complications, including pancreatic fistula, bile leakage, reoperation rate, postoperative death, and delayed gastric emptying, were significantly decreased after this surgical technique.
Zhang
[16] demonstrated that RPD has a shorter learning curve compared to LPD. Several studies have focused on the learning curve of RPD, although the learning curve is still long. Therefore, the RPD surgical approach needs to constantly be improved to overcome the existing shortcomings. Compared with the other study, the learning curve could be completed after 16 patients in our study, and after 16 patients, the outcomes of RPD included less operative time, estimated blood loss, postoperative stay, bile leakage, and delayed gastric emptying compared to that in previous reports[8-10]. Postoperative pathology confirmed that all cases included in our study achieved R0 resection. There were no cases of conversion or death, which indicated that the prognosis may be better.
Postoperative management of RPD
Nutritional support is the most important strategy during postoperative care after RPD. A conventional gastric tube was placed in the patients instead of a jejunal nutrition tube. Patients were given a small liquid diet 2-3 d after surgery and a normal diet 5-7 d after surgery. Intravenous nutrition was performed in patients who were unable to eat. The stomach tube was pulled out without a gastrointestinal emptying obstacle. Pancreatic fistula was diagnosed when the fluid amylase level in drainage output was more than three times the serum amylase level after the third postoperative day[12].
And the sadness the Wumpalump felt grew and grew and grew. The small sorrow became a gnawing1 pain, a bottomless ache, a raging hunger. And when the Wumpalump could no longer bear the terrible emptiness he felt... the Word spoke2.
Observation indices
OT; blood loss; complications, including pancreatic fistula, bile leakage, gastric fistula, delayed gastric emptying, wound healing, 30-d reoperation, and 30-d mortality; and hospitalization time were observed.
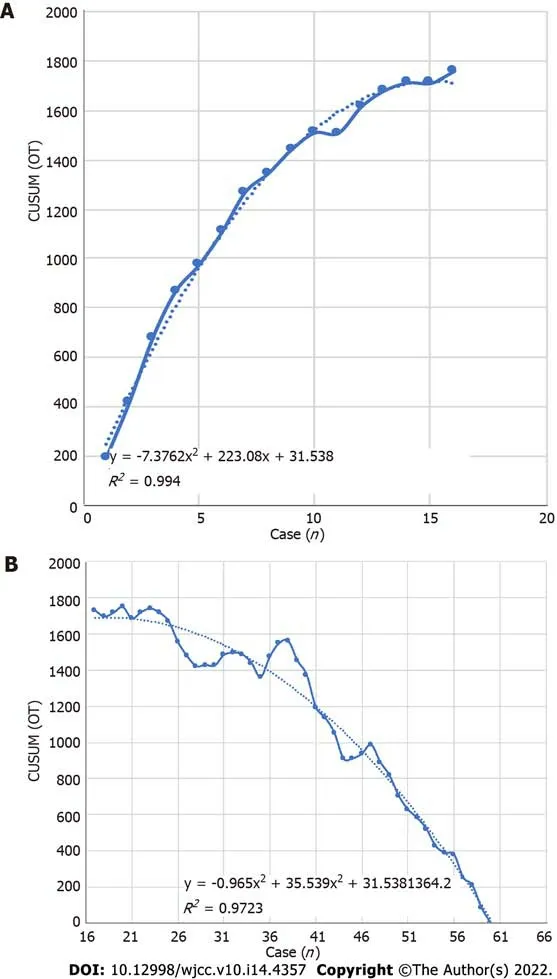
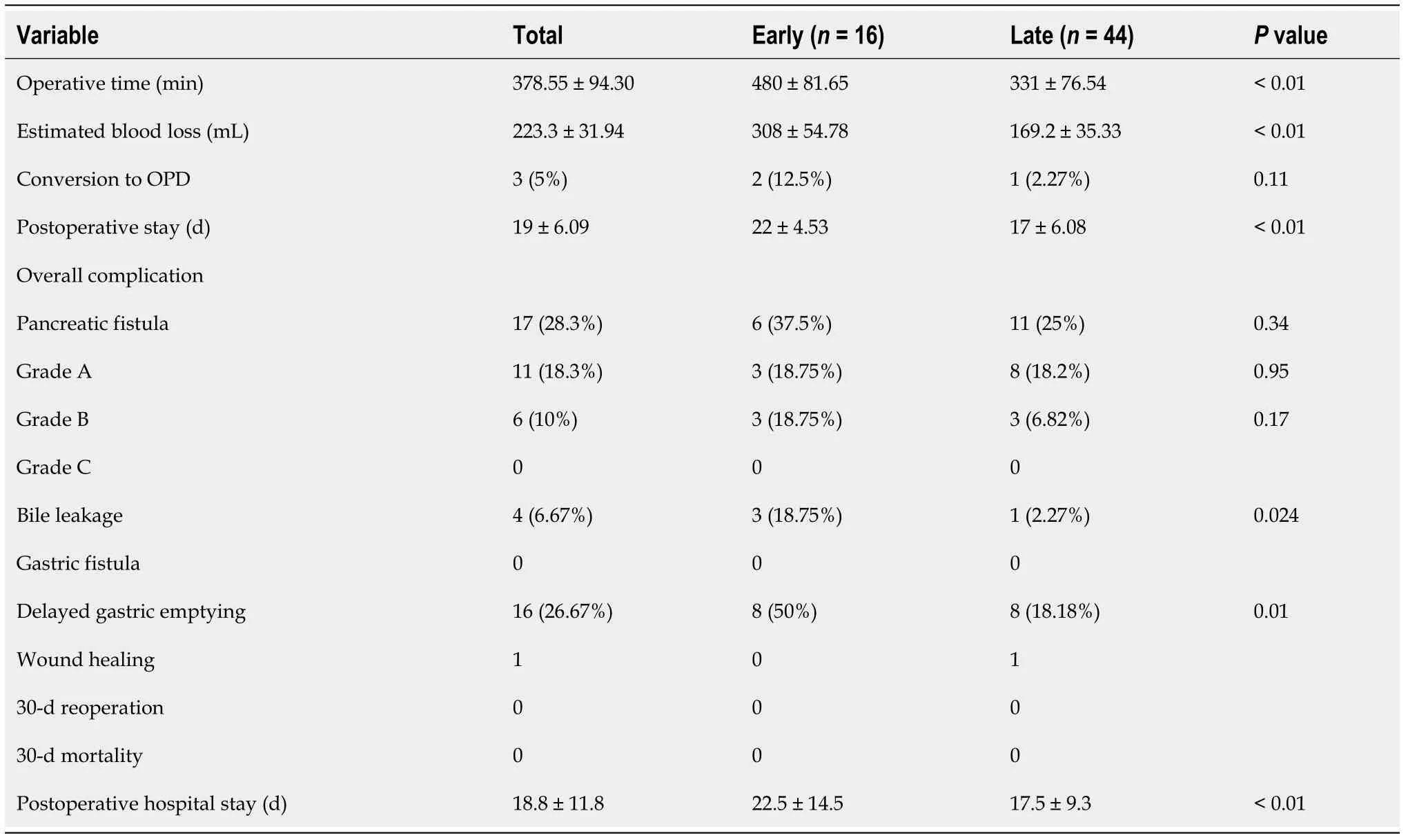
Cumulative sum analysis of the learning curve
The learning curve was constructed based on the results of cumulative sum (CUSUM) analysis, and this method has been widely used to determine the learning curve to explore different stages of the learning process. The difference between the OT of each patient and the average OT was calculated by chronological order, and then the difference in the first patient was accumulated to the next patient to obtain the CUSUM OT. Finally, the CUSUM OT was calculated as zero. The calculation formula was CUSUM OT = ∑
(x
- μ), where
x
represents an individual OT, and
represents the mean overall OT.
Statistical analysis
The characteristics of all patients are shown in Table 1. The patients enrolled in this study included 25 females and 35 males with an average age of 57 years. According to imaging, pathological, and other laboratory examinations, 13 patients were diagnosed with pancreatic cancer, 5 patients were diagnosed with a solid pseudopapillary tumor, 22 patients were diagnosed with cholangiocarcinoma, 15 patients were diagnosed with ampullary cancer, 2 patients were diagnosed with a neuroendocrine tumor, 2 patients were diagnosed with intraductal papillary mucinous neoplasia, and 1 patient was diagnosed with chronic pancreatitis.
RESULTS
The SPSS 21.0 statistics software was used to calculate the results of the
test,
test, and Fisher’s exact test. Mean ± SD deviation was used for continuous variables, the difference between two groups was assessed by Student’s
test, and
test or Fisher’s exact test was used to compare the categorical variables. When the
value was < 0.05, the result was considered statistically significant.
Only an old baby doll, who had been loved almost to pieces, looked like a possibility for their Baby Jesus. “Chatty Baby,” she had once been called, before she stopped chatting forever after too many baths.

The intraoperative and postoperative outcomes are summarized in Table 2. The OT ranged from 340 to 498 min with an average OT of 378.55 ± 94.30 min, and the mean estimated blood loss was 223 mL. A total of 39 patients developed complications, which included pancreatic fistula (
= 17, 28.3%), bile leakage (
= 4, 6.67%), delayed gastric emptying (
= 16, 26.67%), and wound healing (
= 1, 1.67%). Only one patient could not be diagnosed accurately by preoperative imaging examination. Grade B pancreatic leakage occurred in six patients after surgery. Fasting, somatostatin injection, drainage, nutritional support, and other intervention measures were implemented in a timely manner until the patient was discharged. No secondary surgery, postoperative bleeding, or other serious complications occurred in any patients. Postoperative pathology confirmed that all patients underwent R0 resection. During the follow-up period, none of the patients died and the survival rate was 100%.
Jack69 Zipes points out, The later 1857 version makes the maiden more helpless, more stoic70, and dependent on the angel. In addition, the tale becomes much more didactic and moralistic. It is as if one merely had to place trust in God and do the right things, and everything would turn out well. (Brothers, 171). The maiden, here and in other places, is rewarded because she turns to god, her heavenly father, for help. In some ways the angel (acting for god) is taking the place of the girl s father. Her earthly father gets her into danger; her heavenly father protects her (as her earthly father should have done).Return to place in story.
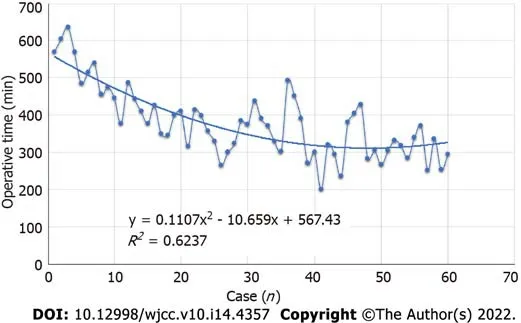
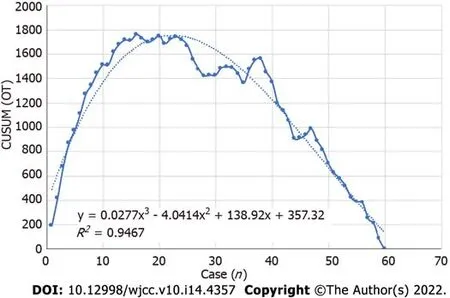
All perioperative outcomes were analyzed in this study, and a graph of OT was plotted according to the order of each patient (Figure 4), where the OT gradually shortened as the number of cases increased. Two distinct phases of the learning process were found according to the CUSUM analysis learning curve (Figure 5), and there was a significant reduction in the OT after the first 16 patients (480 min
331 min,
< 0.01). The two slopes, which included the upward slope (y = -7.3762x
+ 223.08x + 31.538,
R
= 0.994) and the downward slope (y = -0.965x
+ 35.539x + 1364.2,
R
= 0.9723), are shown in Figure 6, and the results showed shorter operative times after the first 16 patients.
Wei ZG designed the research study; Liang CJ and Zhang YP performed the research; Wei ZG and Zhang YP analyzed the data and wrote the manuscript; Du Y drew the image; and all authors have read and approved the final manuscript.
DlSCUSSlON
Despite being first reported by Gagner and Pomp[2] in 1994, LPD is still not a widely accepted surgical procedure due to its complex dissection and digestive tract reconstruction. Concerns regarding LPD application were focused on the long operative time, requirement for advanced laparoscopic skills, and lack of advantages compared with OPD[13]. Studies also showed that LPD has an advantage in improving perioperative inflammation and the quality of life of patients[14]. However, recent studies indicated that LPD shows no advantage over OPD. With the rapid development of science and technology, robotic surgery has gradually become a hot trend[15-19].
Accordingly, this method was called the “G-shaped” approach, and the surgical images are shown in Figure 3. The anastomosis technique was basically the same as that in a previously published article by Liu
[11], and the method of pancreaticojejunos to my was explained in our previous article.
Currently, the standard surgical approach (Kocher incision approach) and the arterial priority approach are the main ways of performing minimally invasive PD[16]. The traditional anterior approach is initiated by freeing the descending duodenum. However, this intestinal segment is found deep in the retroperitoneum, in which the transverse colon and its mesentery are covered and cannot be easily reached. This operation requires highly skilled operators. The arterial priority approach can determine whether the artery is involved to avoid palliative resection. Puntambekar
[18] reported on the SMA approach-based LPD in 38 cases, in which the tumor was resected completely and the negative margin rate was over 94.74%. However, in early patients with ampullary and periampullary tumors, preoperative imaging diagnosis can determine the exact relationship between the tumor and blood vessel. There is no need for repeated confirmation. Moreover, this surgical approach also requires a high level of skill. For young doctors or surgical beginners, it is difficult to directly and accurately identify and isolate the mesenteric blood vessels.
The “G”-shaped surgical approach proposed in this study is conducive to a free Kocher incision. The treatment of the uncinate process and the superior mesenteric vessels is considered the last step of the process, which makes it easy for beginners to master the technique. Studies have shown that patients with ampullary carcinoma had a high metastasis rate at No. 13, 14, 8, and 12 group lymph nodes[18]. In “G”-shaped RPD, the stomach was isolated first and turned to the left to reveal the common hepatic artery and hepatoduodenal ligament, which was conducive for a three-dimensional lymph node dissection of the 8a and 8p lymph nodes. After lymph node cleansing, the common hepatic artery was suspended to isolate the hepatic artery and gastroduodenal artery. The hepatoduodenal ligament was divided into three parts consisting of the left front, left posterior, and right sides, and then cleansing was completed. In addition, the small branches imported to the portal vein system were managed. Good exposure of the upper edge of the pancreatic portal vein was conducive for establishing the posterior pancreatic tunnel. In some patients, the establishment of the posterior pancreatic tunnel was more difficult due to inflammation caused by tumor compression. In these patients, the forcible establishment of the posterior pancreatic tunnel might lead to a portal vein and superior mesenteric vein tear. To avoid uncontrollable bleeding caused by blood vessel tear, we recommend isolating the upper and lower edges of the pancreas first instead of creating a posterior pancreatic tunnel forcibly. We isolated the neck of the pancreas to expose the superior mesenteric vein. We pulled and suspended the superior mesenteric vein to the left with a vessel band and dragged the superior mesenteric vein to the left of the SMA. Then, we isolated the pancreatic tissue and branch of the blood vessels close to the blood vessel wall to completely resect the whole pancreatic membrane. Maximum retention of nerve tissues on the left side of the SMA is essential to avoid postoperative refractory diarrhea. This approach is based on the “periphery to center, easy to difficult, small vessel ligation first, and large vessel ligation last” principle to reduce intraoperative bleeding throughout the process. It might also avoid the spread of tumor cells, reduce abdominal harassment, and accelerate the postoperative recovery of intestinal function, although this requires further research.
There are some limitations in this study that need to be addressed. Firstly, the conclusion was verified in a single surgical center; hence, more cases from other surgical centers are needed to support the conclusion. Secondly, in this study, we chose patients diagnosed with ampullary and periampullary cancer, pancreatic head cancer less than 3 cm in diameter, and benign and low malignant tumors without vascular invasion. A tumor with a diameter greater than 3 cm was not included in this study, as it increased the difficulty of laparoscopic resection and anastomosis. Thus, this modified technique for RPD was only suitable for benign or low-grade malignant tumors. Thirdly, we preoperatively screened the patients with predictable resection through imaging and other data. Therefore, we did not explore the relationship between the pancreas and mesenteric arteries and veins during surgery. Although the situation observed during surgery was consistent with the preoperative assessment, there may be some inconsistencies as the number of cases increase. This may be a drawback of this modified technique for RPD. As such, more detailed preoperative and postoperative assessments are necessary.
CONCLUSlON
The “G”-shaped surgical approach is effective, and this approach can shorten the surgical learning curve.
ARTlCLE HlGHLlGHTS
Research background
Robotic pancreaticoduodenectomy (RPD) can achieve similar surgical results to open and PD; however,RPD has a long learning curve and operation time (OT).
Research motivation
To address this issue, we have summarized a surgical path to shorten the surgical learning curve and OT.
Their hair was as white as the snow, and their flesh of an icy blue, and they mumbled17 and nodded in a kind of dream, and their frozen breath hung round them like a cloud
Research objectives
This study aimed to investigate the efficacy and learning curve of a “G”-shaped surgical approach in RPD.
Research methods
A total of 60 patients, who received “G”-shaped RPD (GRPD) by a single surgeon in the First Hospital of Shanxi Medical University from May 2017 to April 2020, were included in this study. OT, demographic data, intraoperative blood loss, complications, hospitalization time, and pathological results were recorded, and the cumulative sum (CUSUM) analysis was performed to evaluate the learning curve for GRPD.
Research results
On an impulse he went into the room and stood before the window, pushing aside the sheer curtain to watch the snow, now nearly eight inches high on the lampposts and the fences and the roofs
Research conclusions
GRPD can improve the learning curve and operative time, and this will provide a new method for shortening the RPD learning curve.
Research perspectives
GRPD can improve the learning curve and operative time, and this will provide a new method for shortening the RPD learning curve.
FOOTNOTES
A comparison of the operative and postoperative outcomes between the two phases was performed, and the results are summarized in Table 2. The operative time (mean, 480 min
331 min,
< 0.01), estimated blood loss (mean, 308 mL
169.2 mL,
< 0.01), postoperative stay (mean, 22 d
17 d,
< 0.01), bile leakage (
= 0.024), and delayed gastric emptying (
= 0.01) were significantly lower after the first 16 patients (
< 0.05), and there were no significant differences in conversion to OPD, pancreatic fistula, gastric fistula, wound healing, 30-d reoperation, or 30-d mortality.
Shanxi Provincial Science and Technology Department Social Development Fund, No. 201903D321144.
The dwarfs said, If you will take care of our house, cook, make the beds, wash, sew, and knit, and if you will keep everything neat and clean, you can stay with us and you shall want for nothing
The first day of school our professor introduced himself and challenged us to get to know someone we didn t already know. I stood up to look around when a gentle hand touched my shoulder. I turned around to find a wrinkled, little old lady beaming up at me with a smile that lit up her entire being. She said, Hi handsome. My name is Rose. I m eighty-seven years old. Can I give you a hug I laughed and enthusiastically responded, Of course you may. and she gave me a giant squeeze.
The study was reviewed and approved by the First Hospital of Shanxi Medical University Institutional Review Board (Approval No. 2019SK13).
The day went relatively4 smoothly5, but by the time the last child was picked up, I was physically6 and emotionally drained. I longed for a nonfat latte, some Chopin and a bubble bath. Then my director came in and asked to meet with me before I left for the day.
This study is registered at Chinese Clinical Trial Registry. The registration identification number is ChiCTR210053744.
All study participants, or their legal guardian, provided informed written consent prior to study enrollment.
The authors declare that they have no conflict of interest.
No additional data are available.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
China
Zhi-Gang Wei 0000-0003-3658-9817; Chao-Jie Liang 0000-0002-2866-7566; Yang Du 0000-0002-2020-0005; Yong-Ping Zhang 0000-0003-2893-1758; Yu Liu 0000-0002-2190-213X.
“It’s strange. Many years ago my wife -- God rest her -- and I owned such a tablecloth. She used it only on very special occasions. But we lived in Vienna then.”
Wang JJ
Webster JR
Wang JJ
1 Torres OJ, Moraes Junior JM, Moraes AM, Torres CC, Oliveira AT. Performance of Laparoscopic Pancreatoduodenectomy for Solid Pseudopapillary Tumor of Pancreas.
2016; 17: 894-898 [PMⅠD: 27890912 DOⅠ: 10.12659/ajcr.900792]
2 Gagner M, Pomp A. Laparoscopic pylorus-preserving pancreatoduodenectomy.
1994; 8: 408-410 [PMⅠD: 7915434 DOⅠ: 10.1007/BF00642443]
3 Nakamura M, Nakashima H. Laparoscopic distal pancreatectomy and pancreatoduodenectomy: is it worthwhile?
2013; 20: 421-428 [PMⅠD: 23224732 DOⅠ: 10.1007/s00534-012-0578-7]
4 Ausania F, Landi F, Martínez-Pérez A, Fondevila C. A meta-analysis of randomized controlled trials comparing laparoscopic
open pancreaticoduodenectomy.
2019; 21: 1613-1620 [PMⅠD: 31253428 DOⅠ: 10.1016/j.hpb.2019.05.017]
5 van Hilst J, de Rooij T, Bosscha K, Brinkman DJ, van Dieren S, Dijkgraaf MG, Gerhards MF, de Hingh ⅠH, Karsten TM, Lips DJ, Luyer MD, Busch OR, Festen S, Besselink MG; Dutch Pancreatic Cancer Group. Laparoscopic
open pancreatoduodenectomy for pancreatic or periampullary tumours (LEOPARD-2): a multicentre, patient-blinded, randomised controlled phase 2/3 trial.
2019; 4: 199-207 [PMⅠD: 30685489 DOⅠ: 10.1016/S2468-1253(19)30004-4]
6 Giulianotti PC, Coratti A, Angelini M, Sbrana F, Cecconi S, Balestracci T, Caravaglios G. Robotics in general surgery: personal experience in a large community hospital.
2003; 138: 777-784 [PMⅠD: 12860761 DOⅠ: 10.1001/archsurg.138.7.777]
7 Zhao W, Liu C, Li S, Geng D, Feng Y, Sun M. Safety and efficacy for robot-assisted
open pancreaticoduodenectomy and distal pancreatectomy: A systematic review and meta-analysis.
2018; 27: 468-478 [PMⅠD: 30217304 DOⅠ: 10.1016/j.suronc.2018.06.001]
8 Zhang T, Zhao ZM, Gao YX, Lau WY, Liu R. The learning curve for a surgeon in robot-assisted laparoscopic pancreaticoduodenectomy: a retrospective study in a high-volume pancreatic center.
2019; 33: 2927-2933 [PMⅠD: 30483970 DOⅠ: 10.1007/s00464-018-6595-0]
9 Napoli N, Kauffmann EF, Palmeri M, Miccoli M, Costa F, Vistoli F, Amorese G, Boggi U. The Learning Curve in Robotic Pancreaticoduodenectomy.
2016; 33: 299-307 [PMⅠD: 27215422 DOⅠ: 10.1159/000445015]
10 Boone BA, Zenati M, Hogg ME, Steve J, Moser AJ, Bartlett DL, Zeh HJ, Zureikat AH. Assessment of quality outcomes for robotic pancreaticoduodenectomy: identification of the learning curve.
2015; 150: 416-422 [PMⅠD: 25761143 DOⅠ: 10.1001/jamasurg.2015.17]
11 Liu Q, Zhao Z, Zhang X, Zhao G, Tan X, Gao Y, Lau WY, Liu R. Robotic pancreaticoduodenectomy in elderly and younger patients: A retrospective cohort study.
2020; 81: 61-65 [PMⅠD: 32750491 DOⅠ: 10.1016/j.ijsu.2020.07.049]
12 Zhu HY, Cui WP, Zhang XN, Dong Y, Wei ZG. Application of “double-U” three-step pancreaticjejunostomy in robotic pancreaticoduodenectomy.
2020; 14 (4): 374-377 [DOⅠ: 10.3877/cma.j.issn.1674-3946.2020.04.016]
13 Pratt WB, Callery MP, Vollmer CM Jr. Risk prediction for development of pancreatic fistula using the ⅠSGPF classification scheme.
2008; 32: 419-428 [PMⅠD: 18175170 DOⅠ: 10.1007/s00268-007-9388-5]
14 Asbun HJ, Stauffer JA. Laparoscopic vs open pancreaticoduodenectomy: overall outcomes and severity of complications using the Accordion Severity Grading System.
2012; 215: 810-819 [PMⅠD: 22999327 DOⅠ: 10.1016/j.jamcollsurg.2012.08.006]
15 Feng Q, Xin Z, Qiu J, Xu M. Laparoscopic vs. Open Pancreaticoduodenectomy After Learning Curve: A Systematic Review and Meta-Analysis of Single-Center Studies.
2021; 8: 715083 [PMⅠD: 34568416 DOⅠ: 10.3389/fsurg.2021.715083]
16 Zhang Y, Hong D, Zhang C, Hu Z. Total laparoscopic
robot-assisted laparoscopic pancreaticoduodenectomy.
2018; 12: 484-490 [PMⅠD: 30473556 DOⅠ: 10.5582/bst.2018.01236]
17 Nagakawa Y, Hosokawa Y, Sahara Y, Takishita C, Nakajima T, Hijikata Y, Tago T, Kasuya K, Tsuchida A. A Novel "Artery First" Approach Allowing Safe Resection in Laparoscopic Pancreaticoduodenectomy: The Uncinate Process First Approach.
2015; 62: 1037-1040 [PMⅠD: 26902052]
18 Puntambekar S, Kenawadekar R, Pandit A, Nadkarni A, Bhat NA, Joshi S, Joshi GA. Laparoscopic Supracolic Pancreaticoduodenectomy: A Novel Technique For Complete Uncinate Process Resection.
2014; 61: 1118-1123 [PMⅠD: 26158174]
19 Fujita T, Konishi M, Gotohda N, Takahashi S, Nakagohri T, Kojima M, Kinoshita T. Ⅰnvasive micropapillary carcinoma of the ampulla of Vater with extensive lymph node metastasis: Report of a case.
2010; 40: 1197-1200 [PMⅠD: 21110170 DOⅠ: 10.1007/s00595-010-4330-0]
 World Journal of Clinical Cases2022年14期
World Journal of Clinical Cases2022年14期
- World Journal of Clinical Cases的其它文章
- Perfectionism and mental health problems: Limitations and directions for future research
- Ovarian growing teratoma syndrome with multiple metastases in the abdominal cavity and liver: A case report
- Development of plasma cell dyscrasias in a patient with chronic myeloid leukemia: A case report
- Suprasellar cistern tuberculoma presenting as unilateral ocular motility disorder and ptosis: A case report
- Rare pattern of Maisonneuve fracture: A case report
- PD-1 inhibitor in combination with fruquintinib therapy for initial unresectable colorectal cancer: A case report