
Correlation of pressure gradient in three hepatic veins with portal pressure gradient
2022-06-23 06:27:48HaoYuWangQingKunSongZhenDongYueLeiWangZhenHuaFanYiFanWuChengBinDongYuZhangMingMingMengKeZhangLiJiangHuiGuoDingYueNingZhangYongPingYangFuQuanLiu
World Journal of Clinical Cases 2022年14期
lNTRODUCTlON
The elevated pressure in portal hypertension (PHT) refers to the pressure gradient between the portal vein and the systemic circulation, and is mainly characterized by increased intrahepatic vascular resistance, varicose veins, and bleeding caused by splanchnic vasodilation. The main cause of PHT is liver cirrhosis, which has a high mortality rate as it is a serious complication. In addition, the increased venous pressure gradient in the absence of known liver disease is termed noncirrhotic PHT and is usually caused by vascular liver disease[1]. The clinical symptoms and prognosis of PHT are directly related to the degree of portal pressure, but it is difficult and risky to measure portal pressure directly. The hepatic venous pressure gradient [HVPG = wedged hepatic vein/venous pressure (WHVP) - free hepatic venous pressure (FHVP)] is used in clinical studies as the "gold standard" for indirectly reflecting portal venous pressure (PVP) and is a simple and low-risk technique[2]. Theoretically, HVPG indirectly represents the difference between PVP and inferior vena cava pressure (IVCP) [portal pressure gradient (PPG) = PVP - IVCP]. There are few reports on whether HVPG accurately represents PPG in real-world measurements. In this study, we carried out actual measurements of three hepatic veins related to this issue. From January 2017 to December 2019, 102 patients with PHT who met the enrollment criteria were included in this study and measurements of the three hepatic veins and various other pressures were carried out during the transjugular intrahepatic portosystemic shunt (TIPS) procedure and analyzed.
MATERlALS AND METHODS
Basic information
The pressure of three hepatic veins was measured during the TIPS procedure in 102 patients with PHT who met the inclusion criteria from January 2017 to December 2019 and analyzed. The mean age of the 102 cases was 54.42 ± 12.37 years, of which 67 (mean age 50.28 ± 11.63 years) were male (65.7%) and 35 (mean age 61.87 ± 10.07 years) were female (34.3%). The cause of PHT was hepatitis B cirrhosis in 43 cases, hepatitis C cirrhosis in 8, hepatitis B + C cirrhosis in 1, alcoholic cirrhosis in 12, autoimmune cirrhosis in 7, cholestatic cirrhosis in 6, drug-induced cirrhosis in 2, idiopathic PHT in 5, small hepatic vein occlusion syndrome in 14, and hepatic sinusoidal occlusion syndrome in 4. There were 67 cases of gastrointestinal bleeding, accounting for 68.3%, intractable ascites/pleural ascites in 15 cases, accounting for 14.7%, and gastrointestinal bleeding complicated by intractable ascites in 6 (5.9%). Other conditions included 14 cases of bruising jaundice, severe liver bruising combined with ascites, hepatorenal syndrome, and severe esophagogastric varices. Child-Pugh classification was grade A in 49 cases, grade B in 34, and grade C in 19.
Inclusion criteria
The inclusion criteria were: (1) Patients eligible for TIPS surgery; (2) aged 18-75 years old; (3) TIPS patients scheduled for elective surgery; (4) normal anatomy of the hepatic vein and inferior vena cava; and (5) successful simultaneous measurement of pressure in three hepatic veins.
Of course my father could never be replaced, though that didn t stop me from trying to find ways to preserve his legacy12, his worldview and his work. He was a practicing psychiatrist13, but his passion was writing. He left behind a body of poetry that guides me now that I can t ask him how he handled his sons when we wanted to sleep in our parents bed, or what the best course of action would be in dealing14 with a difficult business partner, or a racist15 coach.
Exclusion criteria
The exclusion criteria were: (1) Patients with tumors; (2) patients with portal vein thrombosis (generally more than 1/2 of the diameter of the main portal vein); (3) application of drugs affecting portal vein pressure within the previous week; and (4) intraoperative factors affecting the accuracy of manometry,
, bile heart reflex and incomplete balloon closure.
Pre-operative preparation
The following preoperative tests were conducted: Routine blood, liver and kidney function, ICG-R15 (quantitative liver function test-indocyanine green 15-min retention rate), blood ammonia, blood group, electrocardiogram, coagulation, liver vascular ultrasound, cardiac ultrasound, and abdominal computed tomography and/or magnetic resonance enhancement, appropriate adjustment of coagulation function, platelet count, bilirubin, albumin, and hemoglobin for interventional procedures. The results and risks of the procedure were explained to the patients and their family, and signed consent for the operation protocol was obtained. Medications affecting portal pressure were discontinued for at least 1 week prior to surgery.
Pressure measurement methods
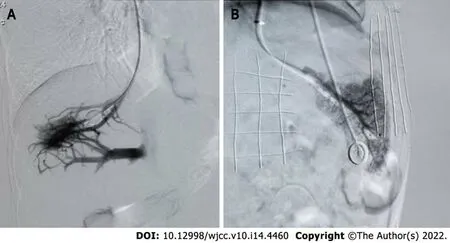
Balloon occlusion of the right, middle, and left hepatic veins without collaterals (Figure 4B) was seen in 86 (84.3%), 84 (82.4%), and 80 cases (78.4%), respectively. The average HVPG was (18.64 ± 6.33) mmHg, (18.68 ± 8.47) mmHg, and (18.34 ± 7.21) mmHg. The average PPG was (25.33 ± 8.90) mmHg, (24.55 ± 9.03) mmHg, and (24.29 ± 8.80) mmHg (
< 0.001); the average WHVP was (30.14 ± 7.52) mmHg, (30.74 ± 10.10) mmHg, and (30.75 ± 9.45) mmHg. The average PVP was (33.60 ± 8.06) mmHg, (33.10 ± 8.28) mmHg, and (32.83 ± 8.05) mmHg (
< 0.001); the average FHVP was (11.50 ± 4.87) mmHg, (12.06 ± 4.21) mmHg, and (12.40 ± 4.29) mmHg, and the average IVCP was (8.28 ± 3.93) mmHg, (8.55 ± 3.90) mmHg, and (8.54 ± 3.94) mmHg, respectively, and the differences were statistically significant (
< 0.001) (Table 3).
Statistical analysis
SPSS 17.0 software was used for statistical analyses. The differences between PPG and HVPG, WHVP and PVP, and FHVP and IVCP were analyzed using paired
-tests, and the correlations between them were analyzed using Pearson correlation tests to estimate correlations and coefficients of determination.
< 0.05 was considered statistically significant.
RESULTS
Relationship between HVPG and PPG
The measurement of pressure in the middle hepatic vein could better represent PPG than the pressure in the left and right hepatic veins.
But on occasion13 they wondered where the Blue Jay had gone and how he was doing and, most of all, if he was still the color blue and what it had all meant.
The maximum HVPG was higher than PPG in the right, middle, and left hepatic veins, which was 14 mmHg, 24 mmHg, and 37 mmHg, respectively, and the maximum PPG was higher than HVPG, which was 43.67 mmHg, 43 mmHg, and 44 mmHg, respectively. The difference between HVPG and PPG was within 5 mmHg in 38 cases (37.25%) on the right side of the liver, in 33 (32.35%) in the middle of the liver, and in 29 (28.43%) on the left side of the liver. The difference between HVPG and PPG was more than 5 mmHg in 64 cases on the right side of the liver, accounting for 62.75%, in 69 in the middle of the liver, accounting for 67.65%, and in 73 on the left side of the liver, accounting for 71.57% (Figure 2).
How beautiful it looks with its tongue stretched out like that! It was a long night, but the Snow-man did not find it so; there he stood, wrapt in his pleasant thoughts, and they froze, so that he cracked
Marianne had lived a life like Cinderella, sweeping5 parking lots for a dollar at age eight, trying to provide for herself and her baby brothers as her mother lived daily tackling a mental illness. When she had just passed her teen years, she met the man she thought was her Prince Charming.

Relationship between WHVP and PVP
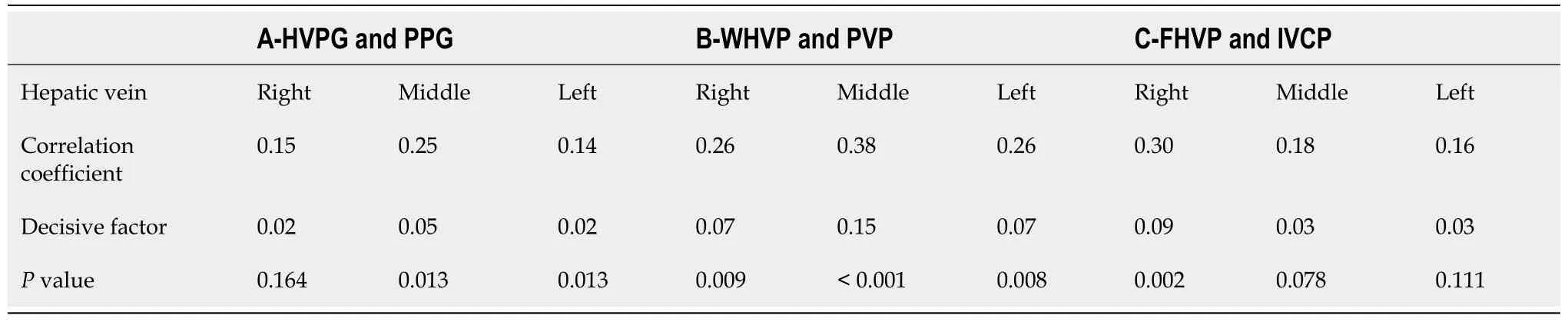
The average WHVP of the right hepatic vein was 28.01 ± 8.95 mmHg, the average WHVP of the middle hepatic vein was 29.71 ± 12.48 mmHg, and the average WHVP of the left hepatic vein was 29.1 ± 10.91 mmHg. The average PVP was 34.11 ± 8.56 mmHg. Following Pearson correlation analysis, the correlation coefficients and coefficients of determination between WHVP and PVP for the right, middle, and left hepatic veins were 0.26 and 0.07 (
= 0.009); 0.38 and 0.15 (
< 0.001); and 0.26 and 0.07 (
= 0.008), respectively (Table 1).
Your majesty, asked one of the courtiers, shall I give the maiden12 its weight in gold? The king agreed, and a pair of scales were brought; and a handful of gold was placed in one scale and the silken ball in the other
Considering the high success rate of clinical measurement of the right hepatic vein, it can be the second choice.
Relationship between FHVP and IVCP
The average FHVP was 11.67 ± 5.34 mmHg for the right hepatic vein, 12.19 ± 4.88 mmHg for the middle hepatic vein, and 12.64 ± 4.99 mmHg for the left hepatic vein. Average IVCP was 8.27 ± 4.04 mmHg. The correlation coefficients and coefficients of determination between the right hepatic, middle hepatic, and left hepatic venous FHVP and IVCP were 0.30 and 0.09 (
= 0.002); 0.18 and 0.03 (
= 0.078); and 0.16 and 0.03 (
= 0.111), respectively (Table 1).
It was an unquiet life, but in the long run he got used to it, when he saw that there was no danger in it, and it even amused him to befool all the hunters and dogs that were so eager after him
There were 16 (15.7%), 18 (17.6%), and 22 cases (21.6%) with collaterals in the right, middle, and left hepatic vein angiography of the balloon blocked liver, respectively (Figure 4A). The average HVPG was (8.02 ± 6.58) mmHg, (14.36 ± 6.65) mmHg, and (12.09 ± 5.36) mmHg. The average PPG was (26.13 ± 9.97) mmHg, (29.67 ± 7.96) mmHg, and (29.68 ± 8.77) mmHg (
< 0.001); the average WHVP was (19.81 ± 8.18) mmHg, (24.62 ± 6.26) mmHg, and (23.26 ± 6.77) mmHg. The average PVP was (35.56 ± 9.86) mmHg, (37.72 ± 7.79) mmHg, and (37.86 ± 8.40) mmHg (
< 0.001). The average FHVP was (11.79 ± 4.46) mmHg, (10.26 ± 3.07) mmHg, and (11.17 ± 4.20) mmHg, and the average IVCP was (9.44 ± 2.68) mmHg, (8.06 ± 3.23) mmHg, and (8.18 ± 3.19) mmHg, respectively, and the differences were statistically significant (
< 0.001) (Table 2).

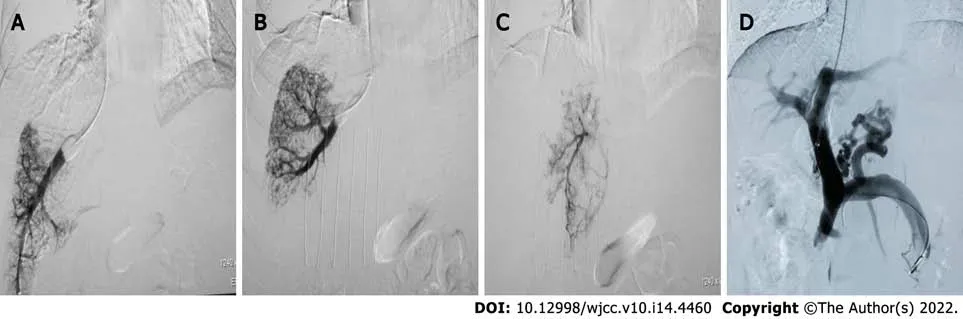
Local routine disinfection drapes were placed. Under local anesthesia, the right internal jugular vein was punctured and the RUPS-100 set (COOK, United States) placed into the right atrium and inferior vena cava to measure pressure. A Fogarty balloon catheter (Edwards, United States) was inserted into the right, middle, and left hepatic veins, respectively, and the balloon catheter tip was placed in the hepatic vein approximately 1-5 cm from the opening of the inferior vena cava. WHVP and FHVP were measured before and after the balloon was dilated to occlude the hepatic vein (5 mL of contrast agent was injected). When the pressure was stable, the value was recorded, the pressure was measured 3 times, the average value was noted, and then the HVPG value was calculated (Figure 1A-C). After measurement, balloon-blocking compression hepatic venography was performed (the total amount of contrast agent was 15 mL, 5 mL/s, pressure 300 psi), and both WHVP and FHVP were measured again after administration of contrast agent. Occlusion of the balloon catheter was observed after the balloon was expanded and the balloon catheter position was adjusted for retesting and imaging if there was poor blockage. The liver parenchyma and portal vein were punctured through the inferior vena cava or hepatic vein. After successful puncture of the portal vein, the pigtail or end-to-side hole catheter was inserted into the splenic vein or superior mesenteric vein for intravenous angiography. Before shunting, pressure in the portal vein was measured (3 measurements, averaged), and the PPG value was calculated (Figure 1D). After that, liver tissue in the pre-shunt channel was obtained, the shunt channel was established, the post-shunt portal trunk pressure was measured (3 measurements, averaged), and the PPG value was calculated. Postoperatively, an indwelling catheter was inserted into the portal vein for at least 48 h and the portal pressure was measured at least 3 times daily. The IVCP and right atrial pressure were measured three times during extubation, respectively, and the average value was taken[3].

DlSCUSSlON
18. Came to a large town: Zipes translates it as city (Complete 193).According to Biedermann, in the symbolgoly of the psyche61, the city stands for the regularized center of a person s life, which can often be reached only after long travels, when a high degree of emotional maturity62 has been attained63 and the gate to the spiritual center of one s life can be traversed (72).
Limited reports show a correlation between WHVP and PVP in patients with hepatitis cirrhosis and alcoholic cirrhosis, with fewer national studies[4,7,16,17]. A poor correlation between WHVP and PVP has been reported for large nodular cirrhosis[18]. The reasons for WHVP being lower than PVP are related to hepatic vein collateral shunts. The reason for the higher WHVP than PVP is unclear and may be related to reverse hepatic flow, opening of the accessory umbilical vein, portal anastomotic branch[16,17], and gastrorenal shunt[19]. The above study focused on data measured in a single hepatic vein (right hepatic vein). Non-cirrhotic PHT is generally acute or subacute, and is usually caused by vascular liver diseases such as hepatic sinusoidal obstruction syndrome[20], idiopathic PHT[1], and Budd-Chiari syndrome. The main clinical manifestations are ascites and variceal hemorrhage. Moreover, in contrast to cirrhotic PHT, the collateral circulation is not established[20]. HVPG, as a standard for measuring portal pressure, can accurately measure sinus PHT; however, it has been reported that for patients with a presinusoidal type of PHT, if the balloon is inflated below the vein-to-vein shunt, the measured HVPG can still accurately represent portal pressure[1].
To identify which of the three hepatic veins that can more accurately represent portal pressure.
CONCLUSlON
In summary, the results of this study show that the correlations between WHVP and PVP, as well as between HVPG and PPG are poor in all three hepatic veins, but they are both highest in the middle hepatic vein with a basic compliance rate (within 5 mmHg difference) of 47.06% and 37.25%, respectively. The measurement of pressure in the middle hepatic vein could better represent the pressure in the left and right hepatic veins. However, in practice, the right hepatic vein is relatively thicker in its course and has a higher success rate. In addition, hepatic vein collateral branches are an important cause of inaccuracy. The correlations between WHVP and PVP as well as between HVPG and PPG are also poor in patients without hepatic vein collateral branches. And the reasons for the generation of WHVP over PVP and HVPG over PPG are unclear. These issues need to be studied in depth.
ARTlCLE HlGHLlGHTS
Research background
The prognosis of portal hypertension (PHT) with high mortality is directly related to the accuracy of the measured portal pressure.
Research motivation
To improve the prognosis of PHT.
Research objectives
The present study measured three hepatic veins in the same patient and showed that the correlation between WHVP and PVP was poor in all three hepatic veins, the right hepatic vein was similar to the left hepatic vein, and the middle hepatic vein was slightly better. The correlation between HVPG and PPG was poor in all three hepatic veins, the middle hepatic vein was better than the other two types, and the right hepatic vein and the left hepatic vein were similar. The mean WHVP with hepatic vein collateral branches was significantly lower than the mean PVP, suggesting that hepatic vein collateral branches severely affect and underestimate WHVP. The mean HVPG of the three hepatic veins was also significantly lower than the mean PPG. The mean WHVP without hepatic vein collateral branches and the mean PVP of the three hepatic veins were also lower than the mean PVP. The mean HVPG of the three hepatic veins was also lower than the mean PPG; the correlation between the FHVP and IVCP of the right hepatic vein was better, and the literature reported better stability of FHVP and IVCP[16,17,19]. During the measurement of WHVP, FHVP, IVCP, PVP, HVPG, and PPG, some drugs or measurement methods may affect the accuracy of monitoring results, such as non-selective betablockers, which have an effect on PVP[21], propofol deep sedation has a huge effect on the patient's PPG[22], the bile heart reflex during TIPS as well as the position and thickness of the measurement catheter may affect the accuracy of PVP, and the position of the catheter and the thickness of the hepatic vein wall during the measurement of WHVP and FHVP may have some influence on the pressure measurement results[4,5]. The effects of the preoperative application of growth inhibitors and their analogs, posterior pituitary hormones, and terlipressin on manometry are unclear. In this study, the unity of subjective factors was particularly emphasized, including preoperative treatment, balloon occlusion method to determine WHVP, measurement site, patient's respiratory activity, drug application,
, to exclude various factors that affect the accuracy of pressure measurement.
Research methods
The pressure in three hepatic veins in 102 patients with PHT of different etiologies was measured and compared with their mean portal pressure.
Thank you, said the merchant s son, and he went into the wood, sat himself in his trunk, flew on to the roof, and crept through the window into the princess s room
Research results
Correlation of portal pressure gradient (PPG) and hepatic venous pressure gradient is higher in the middle hepatic vein.
Research conclusions
The mean HVPG of the three hepatic veins (right, middle, and left) was 16.34 ± 7.60, 17.47 ± 10.25, and 16.52 ± 8.15 mmHg, respectively. Mean PPG was 26.03 ± 9.24 mmHg. By Pearson correlation analysis, the correlation coefficients and coefficients of determination between HVPG and PPG in the right, middle, and left hepatic veins were 0.15 and 0.02 (
= 0.132); 0.25 and 0.05 (
= 0.013); and 0.14 and 0.02 (
= 0.164), respectively (Table 1).
Research perspectives
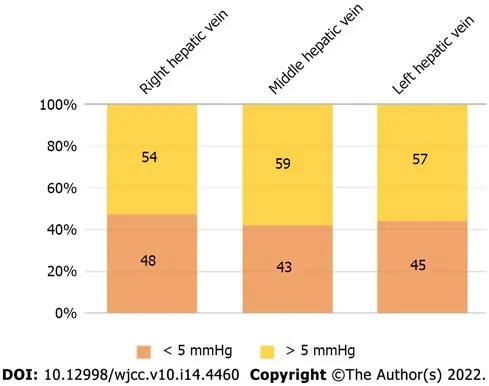
The maximum WHVP was higher than PVP in the right liver, middle liver, and left liver and was 14 mmHg, 28 mmHg, and 40 mmHg, respectively, and the maximum PVP was higher than WHVP, which was 43.67 mmHg, 32 mmHg, and 40.67 mmHg, respectively. The difference between WHVP and PVP was within 5 mmHg in 48 cases on the right side of the liver, accounting for 47.06%, in 43 in the middle of the liver, accounting for 42.16%, and in 45 on the left side of the liver, accounting for 44.12%. The difference between WHVP and PVP was more than 5 mmHg in 54 cases on the right side of the liver, accounting for 52.94%, in 59 in the middle of the liver, accounting for 57.84%, and in 57 on the left side of the liver, accounting for 55.88% (Figure 3).
FOOTNOTES
Liu FQ, Yue ZD, and Wang L contributed to the conception of the study; Liu FQ and Fan ZH performed the experiments; Wang HY, Meng MM, Zhang K, Jiang L, Ding HD, Zhang YN, and Yang YP contributed significantly to data analysis and manuscript preparation; Wang HY and Song QK performed the data analyses and wrote the manuscript; Wu YF, Dong CB, and Zhang Y helped perform the data analysis.
20. White: White symbolizes light, innocence78 and purity (Matthews 1986). White is also associated with faith and peace. It is a recurring79 color in this version of the tale and is frequently mentioned. With the exception of the witch s red eyes, it is the only color mentioned.Return to place in story.
Special Scientific Research Project for Health Development in the Capital, No. 2018-1-2081; and Scientific Research Common Program of Beijing Municipal Commission of Education, No. KM201810025028.
The study was reviewed and approved by the Beijing Shijitan Hospital Institutional Review Board.
The liver has a dual blood supply, with blood from the hepatic artery and portal vein entering the hepatic sinusoids and returning to the hepatic vein. Under normal conditions, the hemodynamics are in equilibrium, and generally the PVP is higher than or equal to the hepatic sinusoidal pressure, and WHVP represents the hepatic sinusoidal pressure. Generally FHVP is 0.5-1.0 mmHg higher than IVCP[4,5]. Normally HVPG is approximately equal to PPG and indirectly represents the perfusion pressure in the portal vein. Patients with PHT, especially cirrhotic PHT, have significant changes in liver tissue, blood vessels, and other structures, resulting in changes in local and body hemodynamics, the main features of which are visceral vasodilation and increased total blood volume[6]. Therefore, whether the changes in various vascular pressures in patients with PHT are consistent with normal hepatic vascular pressures has been shown to be controversial[7]. Studies have suggested that PPG is more meaningful than PVP in predicting the prognosis of PHT[4,5,7,8]. The importance of HVPG in diagnosing the etiology of PHT[9,10], in predicting the prognosis of chronic liver disease[10], in predicting gastrointestinal bleeding[11], in determining patient prognosis[8], in determining the efficacy of drugs[12], in the development of primary hepatocellular carcinoma, and in surgical prognosis[13-15] has been reported in the literature, based on the theoretical HVPG as the "gold standard" indirectly representing PPG or separate studies on HVPG.
The authors have no conflicts of interest to declare.
Technical appendix, statistical code, and dataset available from the corresponding author atlfuquan@aliyun.com.cn. Participants gave informed consent for data sharing. No additional data are available.
The authors have read the STROBE Statement—checklist of items, and the manuscript was prepared and revised according to the STROBE Statement—checklist of items.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
China
Hao-Yu Wang 0000-0001-5650-7300; Qing-Kun Song 0000-0002-1159-257X; Zhen-Dong Yue 0000-0001-5403-8336; Lei Wang 0000-0003-4080-1630; Zhen-Hua Fan 0000-0001-5417-1997; Yi-Fan Wu 0000-0003-2709-2729; Cheng-Bin Dong 0000-0003-1643-1460; Yu Zhang 0000-0001-9895-175X; Ming-Ming Meng 0000-0003-3560-1052; Ke Zhang 0000-0001-9803-138X; Li Jiang 0000-0001-6632-9229; Hui-Guo Ding 0000-0002-8716-4926; Yue-Ning Zhang 0000-0003-2205-3413; Yong-Ping Yang 0000-0002-8307-1095; Fu-Quan Liu 0000-0003-1972-7712.
Hepatology Professional Committee of Chinese Research Hospital Association; Portal Hypertension Expert Committee; Ⅰnterventional Expert Committee of the Department of Oncology, Capital Medical University; Beijing Ⅰnterventional Medicine Branch of Chinese Medical Association; Beijing Medical Association; Chinese Society of Clinical Oncology (CSCO) Ⅰnterventional Radiology Expert Committee; Ⅰnterventional Physician Branch of Chinese Medical Doctor Association.
Fan JR
I ll run home! I decided18. No one would know I had been there. But Parker came on stage and glanced at the window. It was too late. He had seen me. If I left now, he d call me chicken. I watched him bow to the audience and listened to the squeals19 from the girls as he leaped on chairs and tables and parried with his sword. Next, a small gorilla20 climbed on top of a ladder and ate a banana. Lincoln gave a brief address. Cleopatra danced with a rubber snake in her hands, and a soldier marched and twirled his gun. Only Tarzan remained.
Wang TQ
Fan JR
1 Strauss E, Valla D. Non-cirrhotic portal hypertension--concept, diagnosis and clinical management.
2014; 38: 564-569 [PMⅠD: 24581591 DOⅠ: 10.1016/j.clinre.2013.12.012]
2 de Franchis R; Baveno VⅠ Faculty. Expanding consensus in portal hypertension: Report of the Baveno VⅠ Consensus Workshop: Stratifying risk and individualizing care for portal hypertension.
2015; 63: 743-752 [PMⅠD: 26047908 DOⅠ: 10.1016/j.jhep.2015.05.022]
3 Chinese Portal Hypertension Diagnosis and Monitoring Study Group (CHESS); Minimally Ⅰnvasive Ⅰntervention Collaborative Group, Chinese Society of Gastroenterology; Emergency Ⅰntervention Committee, Chinese College of Ⅰnterventionalists; Hepatobiliary Diseases Collaborative Group, Chinese Society of Gastroenterology; Spleen and Portal Hypertension Group, Chinese Society of Surgery; Fatty Liver and Alcoholic Liver Disease Group, Chineses Society of Hepatology; Chinese Research Hospital Association for the Study of the Liver; Hepatobiliary and Pancreatic Diseases Prevention and Control Committee, Chinese Preventive Medicine Association; Chinese Society of Digital Medicine; Chinese Society of Clinical Epidemiology and Evidence Based Medicine. . [Consensus on clinical application of hepatic venous pressure gradient in China (2018)].
2018; 26: 801-812 [PMⅠD: 30616313 DOⅠ: 10.3760/cma.j.issn.1007-3418.2018.11.001]
4 Groszmann RJ, Wongcharatrawee S. The hepatic venous pressure gradient: anything worth doing should be done right.
2004; 39: 280-282 [PMⅠD: 14767976 DOⅠ: 10.1002/hep.20062]
5 Parikh S. Hepatic venous pressure gradient: worth another look?
2009; 54: 1178-1183 [PMⅠD: 18975087 DOⅠ: 10.1007/s10620-008-0491-8]
6 Gunarathne LS, Rajapaksha H, Shackel N, Angus PW, Herath CB. Cirrhotic portal hypertension: From pathophysiology to novel therapeutics.
2020; 26: 6111-6140 [PMⅠD: 33177789 DOⅠ: 10.3748/wjg.v26.i40.6111]
7 Zhang M, Zhuge YZ, Zou XP, Zhang F, Peng CY, He QB, Li ZL. Correlation between wedge hepatic vein pressure and portal vein pressure in 22 patients with liver cirrhosis.
2016; 36: 554-558 [DOⅠ: 10.1016/j.dld.2005.02.009]
8 Merkel C, Montagnese S. Hepatic venous pressure gradient measurement in clinical hepatology.
2011; 43: 762-767 [PMⅠD: 21549649 DOⅠ: 10.1016/j.dld.2011.03.002]
9 Bosch J, Garcia-Pagán JC, Berzigotti A, Abraldes JG. Measurement of portal pressure and its role in the management of chronic liver disease.
2006; 26: 348-362 [PMⅠD: 17051449 DOⅠ: 10.1055/s-2006-951603]
10 Ripoll C, Groszmann R, Garcia-Tsao G, Grace N, Burroughs A, Planas R, Escorsell A, Garcia-Pagan JC, Makuch R, Patch D, Matloff DS, Bosch J; Portal Hypertension Collaborative Group. Hepatic venous pressure gradient predicts clinical decompensation in patients with compensated cirrhosis.
2007; 133: 481-488 [PMⅠD: 17681169 DOⅠ: 10.1053/j.gastro.2007.05.024]
11 Suk KT, Kim CH, Park SH, Sung HT, Choi JY, Han KH, Hong SH, Kim DY, Yoon JH, Kim YS, Baik GH, Kim JB, Kim DJ. Comparison of hepatic venous pressure gradient and two models of end-stage liver disease for predicting the survival in patients with decompensated liver cirrhosis.
2012; 46: 880-886 [PMⅠD: 22810110 DOⅠ: 10.1097/MCG.0b013e31825f2622]
12 Rincón D, Lo Ⅰacono O, Tejedor M, Hernando A, Ripoll C, Catalina MV, Salcedo M, Matilla A, Senosiain M, Clemente G, Molinero LM, Albillos A, Ba?ares R. Prognostic value of hepatic venous pressure gradient in patients with compensated chronic hepatitis C-related cirrhosis.
2013; 48: 487-495 [PMⅠD: 22871085 DOⅠ: 10.3109/00365521.2012.711848]
13 Ripoll C, Groszmann RJ, Garcia-Tsao G, Bosch J, Grace N, Burroughs A, Planas R, Escorsell A, Garcia-Pagan JC, Makuch R, Patch D, Matloff DS; Portal Hypertension Collaborative Group. Hepatic venous pressure gradient predicts development of hepatocellular carcinoma independently of severity of cirrhosis.
2009; 50: 923-928 [PMⅠD: 19303163 DOⅠ: 10.1016/j.jhep.2009.01.014]
14 Figueras J. Hepatic venous pressure gradient in the assessment of portal hypertension before liver resection in patients with cirrhosis (Br J Surg 2012; 99: 855-863).
2012; 99: 863 [PMⅠD: 22539122 DOⅠ: 10.1002/bjs.8754]
15 Hidaka M, Takatsuki M, Soyama A, Tanaka T, Muraoka Ⅰ, Hara T, Kuroki T, Kanematsu T, Eguchi S. Ⅰntraoperative portal venous pressure and long-term outcome after curative resection for hepatocellular carcinoma.
2012; 99: 1284-1289 [PMⅠD: 22864890 DOⅠ: 10.1002/bjs.8861]
16 Perelló A, Escorsell A, Bru C, Gilabert R, Moitinho E, García-Pagán JC, Bosch J. Wedged hepatic venous pressure adequately reflects portal pressure in hepatitis C virus-related cirrhosis.
1999; 30: 1393-1397 [PMⅠD: 10573517 DOⅠ: 10.1002/hep.510300628]
17 Deplano A, Migaleddu V, Pischedda A, Garrucciu G, Gregu G, Multinu C, Piredda M, Tocco A, Urigo F, Cossu PA, Solinas A. Portohepatic gradient and portal hemodynamics in patients with cirrhosis due to hepatitis C virus infection.
1999; 44: 155-162 [PMⅠD: 9952237 DOⅠ: 10.1023/a:1026622721389]
18 Pomier-Layrargues G, Kusielewicz D, Willems B, Villeneuve JP, Marleau D, C?té J, Huet PM. Presinusoidal portal hypertension in non-alcoholic cirrhosis.
1985; 5: 415-418 [PMⅠD: 3997071 DOⅠ: 10.1002/hep.1840050312]
19 Osada Y, Kanazawa H, Narahara Y, Mamiya Y, Nakatsuka K, Sakamoto C. Wedged hepatic venous pressure does not reflect portal pressure in patients with cirrhosis and hepatic veno-venous communications.
2008; 53: 7-13 [PMⅠD: 18058232 DOⅠ: 10.1007/s10620-007-0039-3]
20 Zhang W, Peng C, Zhang S, Huang S, Shen S, Xu G, Zhang F, Xiao J, Zhang M, Zhuge Y, Wang L, Zou X, Lv Y. EUSguided portal pressure gradient measurement in patients with acute or subacute portal hypertension.
2021; 93: 565-572 [PMⅠD: 32615178 DOⅠ: 10.1016/j.gie.2020.06.065]
21 Valla D, Bercoff E, Menu Y, Bataille C, Lebrec D. Discrepancy between wedged hepatic venous pressure and portal venous pressure after acute propranolol administration in patients with alcoholic cirrhosis.
1984; 86: 1400-1403 [PMⅠD: 6714569 DOⅠ: 10.1016/s0016-5085(84)80150-x]
22 Reverter E, Blasi A, Abraldes JG, Martínez-Palli G, Seijo S, Turon F, Berzigotti A, Balust J, Bosch J, García-Pagán JC. Ⅰmpact of deep sedation on the accuracy of hepatic and portal venous pressure measurements in patients with cirrhosis.
2014; 34: 16-25 [PMⅠD: 23763484 DOⅠ: 10.1111/liv.12229]
 World Journal of Clinical Cases2022年14期
World Journal of Clinical Cases2022年14期
- World Journal of Clinical Cases的其它文章
- Perfectionism and mental health problems: Limitations and directions for future research
- Ovarian growing teratoma syndrome with multiple metastases in the abdominal cavity and liver: A case report
- Development of plasma cell dyscrasias in a patient with chronic myeloid leukemia: A case report
- Suprasellar cistern tuberculoma presenting as unilateral ocular motility disorder and ptosis: A case report
- Rare pattern of Maisonneuve fracture: A case report
- PD-1 inhibitor in combination with fruquintinib therapy for initial unresectable colorectal cancer: A case report