
Outcomes of cervical degenerative disc disease treated by anterior cervical discectomy and fusion with self-locking fusion cage
2022-06-22 08:49:06BoZhangYuZhenJiangQingPengSongYanAn
World Journal of Clinical Cases 2022年15期
INTRODUCTION
The incidence of spondylosis has been increasing in recent years as people experience more stress in a rapidly developing society. In addition, spondylosis has become more common in younger populations.Cervical degenerative disc (CDD) disease is a common type of spondylosis. At present, anterior cervical discectomy and fusion (ACDF) is the preferred treatment for CDD disease and is widely accepted as the gold standard treatment. A titanium plate is generally used in ACDF for internal fixation[1,2]. Although ACDF is extensively performed, it has been noted that internal fixation with a titanium plate may cause various postoperative complications, such as pseudarthrosis, loosening of the internally fixed plates,and dysphagia. These disorders may seriously affect the life quality and prognosis of patients[3,4].
In recent years, we have witnessed a growing demand for healthcare. The conventional ACDF +internal fixation using a titanium plate is no longer adequate. Reducing postoperative complications and improving the therapeutic effect have long been topics of interest[5,6]. The invention of the ACDF with a self-locking fusion cage (ROI-C) has effectively decreased the incidence of postoperative complications and has drawn increasing attention[7,8]. In the present study, we further investigated the efficacy of ACDF using ROI-C for internal fixation in CDD disease. Patients with CDD disease treated at our hospital received the conventional ACDF using either a titanium plate or ROI-C for internal fixation.The effect of this technique on patient prognosis was analyzed. The findings offer theoretical clues for the treatment of CDD disease.
MATERIALS AND METHODS
Patients
Ninety patients with CDD disease treated at our hospital from March 2019 to March 2021 were retrospectively analyzed. The present study was approved by the hospital ethics committee. The patients were divided into two groups (control group and observation group,= 45 in each) using a random number table. The control group consisted of 25 males and 20 females aged 26-75 years(average 42.3 ± 5.2 years). With regard to the vertebrae affected, one segment was affected in 38 patients,and two affected in 7 patients. As to the type of spondylosis, 25 patients were affected at the nerve roots,12 patients in the spinal cord, and 8 patients were of mixed type. The observation group consisted of 26 males and 19 females aged 28-79 years (average 43.4 ± 5.3 years). With regard to the vertebrae affected,one segment was affected in 36 patients, and two affected in 9 patients. As to the type of spondylosis, 24 patients were affected at the nerve roots, 14 patients in the spinal cord, and 7 patients were of mixed type. There were no significant differences in terms of gender, age, number of segments affected, and type of spondylosis between the two groups (> 0.05).
Inclusion criteria were: (1) Conformed to the diagnostic criteria for CDD disease according to examinations and clinical signs[9]; (2) voluntarily engaged in the present study and signed an informed consent; (3) unresponsive to conservative treatment; and (4) indicated for cervical spine surgerythe anterior approach.
Exclusion criteria were: (1) Cervical deformity; (2) combined with osteoporosis; (3) history of cervical spine surgery; (4) combined with severe diseases that might influence the results of the present study,such as malignancies; and (5) participating in other studies during the same period.
Methods
The long-term efficacy of ROI-C still needs to be evaluated.
I arrived a couple of days later on a chilly5 autumn morning and spied a frost-covered paper bag on the back steps. With my trowel and bone meal in hand, I set off in search of just the right place to plant.
20.Are you afraid?: Once she has made her decision, the heroine faces her betrothed66 and her future without fear. She is asked several times throughout the tale if she is afraid, but she never is. Return to place in story.#p#
Observation indicators
The two groups of patients were compared in terms of the following surgical parameters: Surgical time,blood loss, drainage volume, and length of hospital stay, in addition to pain, cervical spine function,range of motion, and complications. The visual analogue scale (VAS) was used to assess pain, and the patients were scored on a 0-10 scale. The higher the VAS score, the more severe the pain[10]. Cervical spine function was assessed using the Japanese Orthopedic Association (JOA) score[11] and the neck disability index (NDI)[12]. The total JOA score ranged from 0 to 29. The lower the score, the more severe the dysfunction. NDI is a 10-item questionnaire, and each item is scored from 0 to 5. The total index =[total score/(number of items responded by patients × 5)] 100%. The higher the NDI, the more severe the dysfunction. The cervical range of motion covered cervical disc height and the range of motion of inferior and superior adjacent vertebrae.
Statistical analysis
Statistical analysis was performed using the SPSS 18.0 software (Chicago, IL, United States).Measurements were expressed as mean ± SD, andtest was used for intergroup comparison of measurement data. Counts were expressed as percentages (%), and theχtest was used for intergroup comparison of count data.< 0.05 indicated a significant difference.
1. A widow: A widow often inspires sympathy, perhaps even pity, in fairy tales, except for when she is a stepmother, too. Here the woman is not a stepmother, but she quickly loses the audience s sympathy with her abusive behavior.Return to place in story.
RESULTS
Comparison of surgical parameters between the two groups
There is a special relationship between fans-especially kids-and their heroes that can be almost mystical. Like that time my five college buddies14 and I traveled to Pittsburgh to see Roger. It s so real to me even today, yet back then it seemed like a dream.

Comparison of pain and cervical spine function between the two groups
No significant differences in the VAS, JOA, and NDI scores were observed between the two groups before surgery (> 0.05). The VAS and NDI scores in the observation group were considerably lower than those in the control group after surgery; however, the JOA scores in the observation group were significantly higher than those in the control group (< 0.05, Table 2).

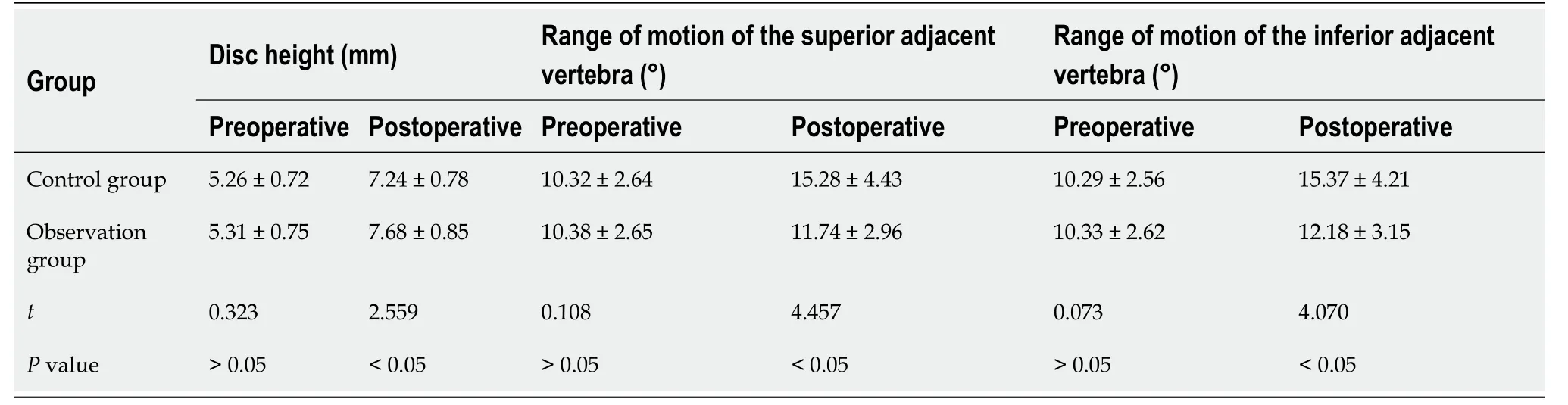
Comparison of the cervical range of motion between the two groups
No significant differences were observed in cervical disc height and the range of motion of the superior and inferior adjacent vertebrae between the two groups before surgery (> 0.05). The cervical disc height in the observation group was larger than that in the control group after surgery. The range of motion of both the superior and inferior adjacent vertebrae was significantly smaller in the observation group than in the control group (< 0.05, Table 3).
Comparison of complications between the two groups
Complications in the two groups included dysphagia, loosening of the internally fixed implant, and infection. The incidence of these complications was only 2.22% in the observation group compared to 15.56% in the control group, and the difference was statistically significant (< 0.05, Table 4).
The dolphins sported in the waves, and the great whales spouted29 water from their nostrils30 till it seemed as if a hundred fountains were playing in every direction
But the King was never able to enjoy his treasure, for he might watch and guard them as he liked, as soon as they began to get ripe they were always stolen
Patients in the observation group received ACDF + ROI-C placement for internal fixation. The first few steps were the same as those in the control group until the intervertebral disc was removed. Then trialing began to select an implant of the appropriate size. After filling with autologous bone, the implant was inserted into the intervertebral space. The implant position was confirmed by C-arm X-ray.Subsequently, two ROI-C VerteBRIDGE plates were tapped in for immobilization. A drainage tube was placed after surgery, and the incision was closed. The autologous bone from the resected osteophytes and decompression were used for intraoperative bone grafting in the two groups.

DISCUSSION
The pathogenesis of CDD disease has not yet been fully clarified. Some scholars attribute this disease to the natural degeneration of intervertebral discs[13,14]. Others propose that it is associated with biomechanical changes in the adjacent vertebrae after surgery[15,16]. ACDF is a common treatment for cervical disc disorders. Several procedures have been proposed for ACDF. For example, ACDF with autologous bone grafting, allogenic bone grafting, anterior steel plate placement, or an intervertebral fusion cage has been widely used. No significant difference in the fusion rate has been reported with different ACDF procedures. However, differences have been observed in the incidence of complications and postoperative recovery[17-19].
ACDF with internal fixation using a steel plate is one of the most common choices. Although the steel plate improves cervical stability and promotes bone fusion, the anterior placement of a steel plate requires a larger surgical field. Therefore, the esophagus, trachea, and nerves are more likely to be damaged, leading to postoperative complications[20]. In addition, screw insertion may damage the spinal cord and vertebral artery, leading to long-term complications, such as screw loosening and steel plate dislocation[21]. How to improve the therapeutic effect of ACDF and reduce complications has been a long-standing concern. In recent years, an increasing number of reports have emerged concerning the use of an intervertebral fusion cage in ACDF, and the outcome is generally good[22-24].
We recruited patients with CDD disease treated at our hospital by ACDF using either a conventional titanium plate or ROI-C for internal fixation. The results showed that surgical time, blood loss, drainage volume, and length of hospital stay were not significantly different between the two groups of patients.This was because the first few steps of the surgical procedures were similar between the two groups(Figure 1) and the steps following removal of the intervertebral disc were different. In the control group,the patients received internal fixation using a titanium plate after autologous bone grafting. In the observation group, autologous bone was first placed into the implant, which was then inserted into the intervertebral space. Both procedures were easy. There were no significant differences in surgical time,blood loss, postoperative drainage volume, and length of hospital stay between the two groups. Pain and cervical spine function were assessed in the two groups. The VAS scores and NDI were lower in the observation group than in the control group, while the JOA scores were higher in the former than in the latter. These results indicated that pain was relieved more after surgery in the observation group, hence the cervical spine function was better. The cervical range of motion in the two groups was examined,and it was found that the cervical disc height was larger in the observation group than in the control group. The range of motion of both the superior and inferior adjacent vertebrae was significantly smaller in the observation group than in the control group. These results indicated that the cervical discheight was improved considerably in the observation group after surgery, with the range of motion in adjacent vertebrae mildly affected.
Horror gripped the heart of the World War I soldier as he saw his lifelong friend fall in battle. Caught in a trench1 with continuous gunfire whizzing over his head, the soldier asked his lieutenant2 if he might go out into the No Man s Land between the trenches3 to bring his fallen comrade back.

In the present study, it was also found that the incidence of postoperative complications was significantly lower in the observation group than in the control group. This was because two VerteBRIDGE plates were used with ROI-C. These self-locking plates were inserted into the superior and inferior vertebrae, respectively, to immobilize the implant more effectively. As the implant is more firmly immobilized by the VerteBRIDGE plates, postoperative complications are generally reduced.
The intervertebral fusion cage can maintain lordosis and a normal range of motion and prevent kyphosis. Thus, the intervertebral fusion cage plays an important role in relieving postoperative pain and improving cervical spine functions[25,26]. The intervertebral fusion cage involves slight peeling of the anterior longitudinal ligament, with only exposure of the intervertebral space in the segment to be operated. The screws were inserted at an oblique angle into the endplate through the intervertebral space (Figure 2). In this way, the adverse influence on the adjacent vertebrae is minimized, especially the range of motion of adjacent vertebrae[27,28]. The vertebral bodies are separated using a distractor before inserting the intervertebral fusion cage, which is conducive to restoring the vertebral height. An intervertebral fusion cage insertion reduces height loss of the vertebral body, relieves nerve root compression, and avoids degeneration of adjacent vertebrae[29,30].
Late, late into this night, Allison and Clark gutted12 and carved the pumpkins together, at an old table set on the back porch, over newspaper after soggy newspaper, with paring knives and with spoons and with a Swiss Army knife Clark used for exact shaping of tooth and eye and nostril13. Clark had been a doctor, an internist, but also a Sunday watercolorist. His four pumpkins were expressive14 and artful. Their carved features were suited to the sizes and shapes of the pumpkins. Two looked ferocious15 and jagged. One registered surprise. The last was serene16 and beaming.

CONCLUSION
Taken together, ROI-C with internal fixation showed similar efficacy to conventional titanium plates in ACDF for CDD disease. However, cervical spine function restoration was better with the former than with the latter. The range of motion of the cervical spine was not increased significantly after using ROIC. Nevertheless, pain and complications were less common using ROI-C. Given the above advantages,the ROI-C featuring VerteBRIDGE plates is worthy of clinical popularization.
ARTICLE HIGHLIGHTS
Research background
To observe the outcomes of cervical degenerative disc (CDD) disease treated by ACDF with ROI-C.
Surgical time, blood loss, drainage volume, and length of hospital stay were not significantly different between the two groups of patients (> 0.05, Table 1).
Research motivation
To evaluate the efficacy of ROI-C.
Research objectives
The conventional anterior cervical discectomy and fusion (ACDF) + internal fixation using a titanium plate is no longer adequate. The invention of the ACDF with a self-locking fusion cage (ROI-C) has effectively decreased the incidence of postoperative complications after ACDF and has drawn increasing attention.
Research methods
Ninety patients with CDD disease treated at our hospital from March 2019 to March 2021 were included. They were divided into two groups (= 45 in each) using a random number table. Patients in the control group received ACDF plus internal fixation with a titanium plate. Those in the observation group received ACDF + ROI-C placement. The two groups of patients were compared in terms of surgical parameters, pain, cervical spine function, range of motion, and complications.
Research results
The two groups of patients showed no significant differences in surgical time, blood loss, drainage volume, and length of hospital stay (> 0.05). No significant differences in the visual analogue scale(VAS), Japanese Orthopaedic Association (JOA), and neck disability index (NDI) scores were observed between the two groups before surgery (> 0.05). The JOA scores in the observation group were significantly higher than those in the control group (< 0.05). No significant differences were observed in cervical disc height and the range of motion of the superior or inferior adjacent vertebrae between the two groups before surgery (> 0.05). The range of motion of both the superior and inferior adjacent vertebrae was significantly smaller in the observation group than in the control group (< 0.05). The incidence of complications was only 2.22% in the observation group compared to 15.56% in the control group, and the difference was statistically significant (< 0.05).
Research conclusions
The use of ROI-C with internal fixation in ACDF had similar efficacy to the use of conventional titanium plates in ACDF for CDD disease. However, cervical spine function restoration after using ROI-C was better than the control. The range of motion of the cervical spine was not increased significantly after using ROI-C, but pain and complications were less common. The ROI-C featuring the VerteBRIDGE plate is worthy of clinical popularization.
Research perspectives
Patients in the control group received ACDF plus a titanium plate for internal fixation. The patients were placed in the supine position. General anesthesia was performed after tracheal intubation. The head was immobilized in a neutral position, and the neck was slightly moved backward. A transverse incision of approximately 6 cm was made in the right anterior cervical region. The skin was cut open,and the platysma muscle was transected. The muscle flap was pulled down. Blunt dissection was performed at the intermuscular space between the sternocleidomastoid muscle and sternothyroid. The omohyoid muscle was exposed and then dissociated, ligated, and severed. The esophagus and trachea were pushed to the left. External traction was applied to the sternocleidomastoid muscle and carotid sheath to expose the prevertebral fascia. The relevant segment was located by a C-arm X-ray. A longitudinal incision was made in the prevertebral fascia to peel it up and down slowly. The range of peeling did not exceed the medial margin of the longus colli muscle by 3 mm. Two distraction screws were inserted into the middle of the superior and inferior vertebrae adjacent to the lesioned segment,respectively. The distractor was mounted on the screws to separate the vertebral bodies. The anterior longitudinal ligament was cut open and peeled off to the two sides. The fibrous ring was exposed and cut open using a long-handled scalpel. Blunt dissection was performed up and down to remove the intervertebral disc. Autologous bone was placed into the intervertebral space. A titanium anterior cervical plate of an appropriate length was inserted for internal fixation. The implant position was confirmed again by C-arm X-ray, and locking screws were inserted for internal fixation. A drainage tube was placed after surgery, and the incision was closed.
FOOTNOTES
Zhang B designed the research study; Jiang YZ, Song QP, and An Y performed the research;Jiang YZ and Song QP analyzed the data and wrote the manuscript; all authors have read and approve the final manuscript.
The study was conducted according to the Declaration of Helsinki and approved by the Ethics Committee of Beijing Jishuitan Hospital (202110-04).
All study participants, or their legal guardian, provided informed written consent prior to study enrollment.
There are no conflicts of interest to report.
Data can be acquired from the corresponding author.
The authors have read the STROBE Statement—checklist of items, and the manuscript was prepared and revised according to the STROBE Statement—checklist of items.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
China
I shut off the recorder and Rebekah sighed deeply. Thank you, Nan, she said with a weak smile. You ll give this one to them, won t you? she murmured as she slid into sleep.
Bo Zhang 0000-0002-6320-7258; Yu-Zhen Jiang 0000-0003-2248-7211; Qing-Peng Song 0000-0002-2146-6913; Yan An 0000-0003-4919-2106.
Chen YL
Filipodia
Chen YL
 World Journal of Clinical Cases2022年15期
World Journal of Clinical Cases2022年15期
- World Journal of Clinical Cases的其它文章
- Diet and intestinal bacterial overgrowth: Is there evidence?
- Spontaneous liver rupture following SARS-CoV-2 infection in late pregnancy: A case report
- Metastasis of liver cancer to the thyroid after surgery: A case report
- Solitary primary pulmonary synovial sarcoma: A case report
- Knot impingement after arthroscopic rotator cuff repair mimicking infection: A case report
- Clear aligner treatment for a four-year-old patient with anterior crossbite and facial asymmetry: A case report