
Knot impingement after arthroscopic rotator cuff repair mimicking infection: A case report
2022-06-22 08:49:26DuHanKimJongHyukJeonByungChanChoiChulHyunCho
World Journal of Clinical Cases 2022年15期
INTRODUCTION
Determining the cause of acute joint pain in patients with no history of trauma can be challenging for the orthopedic clinician[1]. Because the destruction of the involved joint can occur rapidly, a septic condition should be considered when making a diagnosis. However, making a differential diagnosis of infection from other problems that can induce acute joint pain is not always easy. Acute onset of shoulder pain is a relatively common symptom observed in the clinical setting. The most common causes of acute shoulder pain include calcific tendinitis, subacromial bursitis, and septic arthritis[1].
Arthroscopic rotator cuff repair (ARCR) is a procedure that is widely performed with satisfactory outcomes[2-5]. Development of knot impingement as a complication after ARCR has been suggested as a cause of persistent pain with limited motion[6,7]. To date, only 13 cases involving knot impingement after ARCR have been reported and most of the patients complained of insidious onset of pain during shoulder motion[6-8]. Previous studies have focused on the pathogenesis of bone erosion on the acromial undersurface caused by suture knots[6-8]. Because of its rarity, information regarding the clinical features in patients with knot impingement after ARCR is limited.
We report on a case involving a patient who developed knot impingement after ARCR who complained of acute onset of pain with limited motion, which was confused with infection. This report describes our experience with a rare case mimicking infection; successful management was achieved by arthroscopic removal of the knot.
CASE PRESENTATION
Chief complaints
A 55-year-old female who complained of severe pain with limited motion of the right shoulder visited our emergency room.
History of present illness
Development of pain had occurred two days ago; the pain was dull and continuous in nature regardless of shoulder motion.
History of past illness
According to the results of laboratory tests, the white blood cell count was 7920/μL (normal ranges,4000-10000/μL) with 66.9% neutrophils. C-reactive protein (CRP) and erythrocyte sedimentation rate(ESR) were elevated at 8.4 mg/dL (normal ranges, 0.0-0.5 mg/dL) and 50 mm/hr (normal ranges, 0-25 mm/hr), respectively. Because a septic condition was suspected, aspiration was performed through the subacromial space and 2 cc of yellowish fluid with mucoid nature was obtained. Results of the fluid analysis showed that the WBC count was 3960 with 90% neutrophils.
Knot impingement has recently been described as a complication occurring after ARCR resulting in pain during motion; additional surgery may be necessary for removal of the suture knots[6,7]. To date, only 13 cases involving knot impingement after ARCR have been reported[6-8]. In 2010, Hotta and Yamashita[6] first reported that acromial erosion was observed in nine of 434 (2.1%) patients who had undergone ARCR. They found an association between the knot position and the portion of osteolysis on the undersurface of the acromion; the patients no longer had symptoms after removal of the knots[6].They concluded that this complication might have been caused by knot impingement resulting from the knots of the suture thread[6]. Park
[8] also reported that acromial erosion was observed in three of 221 (1.4%) patients with ARCR. Uchida
[7] recently reported two cases involving symptomatic knot impingement resulting in subacromial bone erosion.
I, of course, kept shoving peas down my throat. The glares made me nervous, and every single pea made me want to throw up, but the magical image of that five dollars floated before me, and I finally gagged down every last one of them. My grandmother handed me the five dollars with a flourish. My mother continued to glare in silence. And the episode ended. Or so I thought.
Personal and family history
National Research Foundation of Korea, No. 2021R1F1A1047546.
Physical examination
A review of the literature found that some shoulder problems such as calcific tendinitis, subacromial bursitis, chronic lymphocytic leukemia, small lymphocytic lymphoma, and deep vein thrombosis can mimic infection by presenting with acute onset of severe pain[1,9,10]. Although the incidence is rare, the possibility of knot impingement should be considered for patients with acute pain and limited motion of the shoulder who have a history of ARCR.
Laboratory examinations
The patient had undergone ARCR using a suture-bridge technique at a local clinic four months ago for treatment of a small supraspinatus tear of the right shoulder.
Imaging examinations
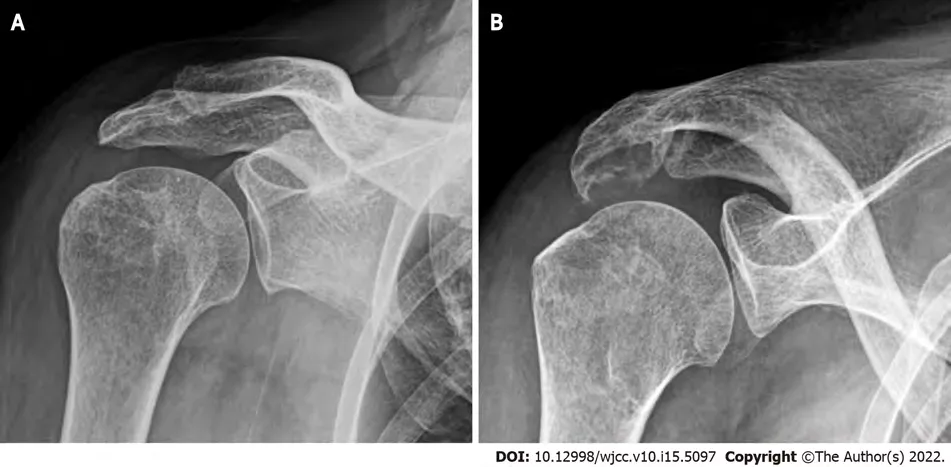
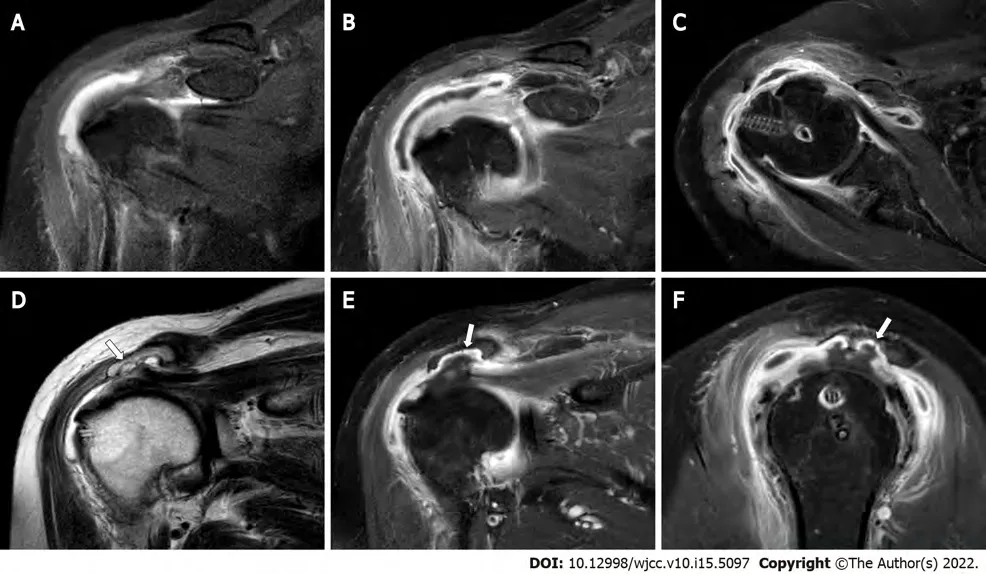
An erosive change of the undersurface of the acromion was observed on plain radiographs of the right shoulder at 30
caudal tilting view (Figure 1). A moderate amount of bursal fluid and synovial thickening with enhancement was observed by enhanced magnetic resonance imaging (MRI) (Figure 2).In addition, an irregular erosive change of the undersurface of the acromion was also observed.
FINAL DIAGNOSIS
Suggested causes of knot impingement after ARCR include the position of the knot, exposure of cancellous bone after acromioplasty, and stronger suture materials[6-8]. Hotta and Yamashita[6], who reported observing knots on the top of the greater tuberosity in all cases involving knot impingement,suggested that the use of a knotless or suture-bridge repair technique may be helpful in prevention of symptomatic knot impingement during ARCR. However, Park
[8] reported that there was no difference in acromial erosion in high-profile knots made using a single row technique compared with a double row suture-bridge technique. Acromial erosion due to knot impingement may be the result of exposure of weak cancellous bone after acromioplasty[6,8]. Anchor suture limbs have recently been replaced by strong braided nonabsorbable suture materials such as FiberWire (Arthrex, Naples, FL,United States), resulting in stronger knots without suture breakage during ARCR[8]. However, these characteristics may contribute to development of knot impingement after ARCR. In our case,acromioplasty and ARCR were performed using suture anchors with strong braided nonabsorbable suture threads. Even though a suture-bridge technique was used in performance of ARCR, an association of knot impingement with loose suture threads and knots was confirmed.
TREATMENT
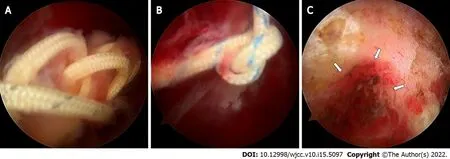
The arthroscopic view showed healing of the repaired supraspinatus tendon and loose suture threads and knots with severe subacromial bursitis were observed. Impingement of suture knots was observed at the undersurface of the acromion, resulting in erosion of subacromial bone (Figure 3). Debridement of inflammatory tissues of the glenohumeral joint and subacromial space was performed for removal of all suture materials.
OUTCOME AND FOLLOW-UP
The final culture from the aspirated bursal fluid showed no growth of organisms. The patient’s symptoms subsided immediately after this procedure. Completely restored range of motion without pain at rest or activity was observed at one-year follow-up after surgery.
DISCUSSION
I am sending you my last payment of three dollars to pay for the beds in full. I told my two sons that they could now go to the storage shed and put the beds together and sleep in them, for they are now paid for and rightfully ours. Thank you for your trust.
Although a definite diagnosis of infection was not indicated by these findings, because the possibility of infection could not be ruled out completely based on the clinical symptoms, the patient was scheduled to undergo emergency arthroscopic surgery.
Because of its rarity, there is a poor understanding of clinical features in patients with knot impingement. Although previous studies have not provided a detailed description, in most reported cases there was insidious development of symptoms, which were aggravated during shoulder motion such as overhead working and sports activities[6-8]. Different clinical features were observed in the current study compared to previously reported cases. The patient visited the emergency room with a complaint of acute onset of severe pain and limited motion. Due to the clinical features with elevated ESR and CRP on laboratory tests and fluid collection and synovial thickening with enhancement on MRI there was concern of an infectious condition. Therefore, emergency arthroscopic surgery was performed for diagnostic and therapeutic intention. Erosive change of the acromial undersurface was observed on plain radiographs prior to arthroscopic surgery. However, the clinical features were more like an infection; therefore symptomatic knot impingement was not detected. Using arthroscopic findings we determined that knot impingement with suture threads might have been the cause of the patient’s pain.Conduct of further studies, including large numbers of patients, is needed in order to clarify the pathogenesis and clinical features of knot impingement after ARCR.
Tenderness on the involved shoulder was observed and body temperature was 37.4
C. Her active range of motion was 45
of forward flexion, 30
of abduction, 25
of external rotation at the side, and buttock level of internal rotation at the back. Passive range of motion could not be evaluated because the patient was experiencing severe pain.
CONCLUSION
To the best of our knowledge, this is the first report of knot impingement after ARCR mimicking infection with successful management by arthroscopic removal of the knot. We suggest consideration of knot impingement after ARCR as a cause of acute shoulder pain.
10. I will lead you home again: Although he is the most maligned75 of the children, Little Thumb is the only one of the brothers who takes any action toward saving themselves.Return to place in story.
ACKNOWLEDGEMENTS
The authors thank Eun-Ji Jeon for her support.
FOOTNOTES
Cho CH and Kim DH performed the conceptualization; Choi BC contributed to the investigation; Choi BC and Kim DH contributed to the data curation; Jeon JH wrote the original draft preparation;Cho CH wrote the review and editing, performed the supervision; Kim DH wrote the project administration; all authors have read and agreed to the published version of the manuscript.
The patient had no personal or family history.
Informed written consent was obtained from the patient for publication of this report and any accompanying images.
The authors declare that they have no conflict of interest.
102. Have a good cry103. Make time for hobbies104. Limit work time105. Compromise/cooperate106. Don t procrastinate19107. Unplug your phone/TV108. Relax your standards109. Journal your thoughts110. Take a vacation111. Organize your desk112. Develop flexibility20113. Allow for imperfections114. Don t overschedule115. Expose your secrets116. Build a strong body117. Nurture your faith118. Open a savings21 account119. Take in the sun120. Love and be loved121. Get the facts122. Work as a team123. Smile - open your heart124. Validate22 yourself125. Daydream23126. Know God loves you!
The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
South Korea
So Aveline made her preparations accordingly, and began by arranging that the equerry should lose himself in the forest, after which she took away the king s sword and his horse while he lay asleep under a tree
Du-Han Kim 0000-0002-6636-9340; Jong-Hyuk Jeon 0000-0001-7815-8148; Byung-Chan Choi 0000-0002-0171-1862; Chul-Hyun Cho 0000-0003-0252-8741.
Fan JR
The miller was shocked and answered, How could I cut off my own child s hands? Then the Evil-one threatened him and said, If thou dost not do it thou art mine, and I will take thee thyself
One day a jackal who was prowling about in search of a dinner came by chance to the foot of the rock where the dove s nest was hidden away, and he suddenly bethought himself that if he could get nothing better he might manage to make a mouthful of one of the young doves
A
It was a fine September night, with a silver moon riding high. They washed up the supper dishes and then took their chairs out onto the porch. I ll get my fiddle1(), said the old man, and play you some of the old tunes3.
Fan JR
1 Ross G, Cooper J, Minos L, Steinmann SP. Acute calcific tendinitis of the shoulder mimicking infection: arthroscopic evaluation and treatment--a case report.
2006; 35: 572-574 [PMID: 17243407]
2 Oh SY, Jang YH, Chae IS, Kim SH. Prevalence and Clinical Impact of Acromial Cupping after Arthroscopic Rotator Cuff Repair: Does Acromioplasty Matter?
2021; 13: 520-528 [PMID: 34868502 DOI: 10.4055/cios21010]
3 Lee D, Lee KH, Jo YH, Joo IH, Lee HJ, Jeong SY, Lee BG. Correlation between Severity of Synovitis and Clinical Features in Rotator Cuff Tears.
2021; 13: 88-96 [PMID: 33747384 DOI: 10.4055/cios20002]
4 Kim H, Song HS, Kang SG, Han SB. Arthroscopic Capsular Repair without Relaying Sutures: 'Simple Sewing Technique'.
2019; 22: 146-148 [PMID: 33330211 DOI: 10.5397/cise.2019.22.3.146]
5 Park JY, Lee JH, Oh KS, Chung SW, Choi Y, Yoon WY, Kim DW. Rotator cuff retear after repair surgery: comparison between experienced and inexperienced surgeons.
2021; 24: 135-140 [PMID: 34488293 DOI:10.5397/cise.2021.00073]
6 Hotta T, Yamashita T. Osteolysis of the inferior surface of the acromion caused by knots of the suture thread after rotator cuff repair surgery: knot impingement after rotator cuff repair.
2010; 19: e17-e23 [PMID: 21070953 DOI: 10.1016/j.jse.2010.07.002]
7 Uchida A, Mihata T, Neo M. Subacromial bone erosion due to suture-knots in arthroscopic rotator cuff repair: A report of two cases.
2019; 16: 30-35 [PMID: 30984561 DOI:10.1016/j.asmart.2018.11.006]
8 Park YE, Shon MS, Lim TK, Koh KH, Jung SW, Yoo JC. Knot impingement after rotator cuff repair: is it real?
2014; 30: 1055-1060 [PMID: 24908257 DOI: 10.1016/j.arthro.2014.04.091]
9 Donovan A, Schweitzer ME, Garcia RA, Nomikos G. Chronic lymphocytic leukemia/small lymphocytic lymphoma presenting as septic arthritis of the shoulder.
2008; 37: 1035-1039 [PMID: 18521594 DOI:10.1007/s00256-008-0512-x]
10 Lisse JR, Thurmond-Anderle M, Davis CP. Deep venous thrombosis in intravenous cocaine abuse mimicking septic arthritis of the shoulder.
1991; 84: 278-279 [PMID: 1990471 DOI: 10.1097/00007611-199102000-00034]
 World Journal of Clinical Cases2022年15期
World Journal of Clinical Cases2022年15期
- World Journal of Clinical Cases的其它文章
- Diet and intestinal bacterial overgrowth: Is there evidence?
- Spontaneous liver rupture following SARS-CoV-2 infection in late pregnancy: A case report
- Metastasis of liver cancer to the thyroid after surgery: A case report
- Solitary primary pulmonary synovial sarcoma: A case report
- Clear aligner treatment for a four-year-old patient with anterior crossbite and facial asymmetry: A case report
- Catheter-related infections caused by Mycobacterium abscessus in a patient with motor neurone disease: A case report