
Bone flare after initiation of novel hormonal therapy in patients with metastatic hormone-sensitive prostate cancer: A case report
2022-06-22 08:49:22KeHaoLiYuanChengDuDongYuYangXinYuanYuXuePingZhangYongXiangLiLiangQiao
World Journal of Clinical Cases 2022年15期
INTRODUCTION
Prostate cancer (PCa) is ranked as the second most common cancer and the fifth leading cause of cancerrelated deaths in men worldwide in 2018[1]. Unfortunately, some patients develop metastatic castrationresistant prostate cancer (mCRPC), including metastatic hormone-sensitive prostate cancer (mHSPC). In recent years, studies have confirmed that apalutamide sustains a lower level of prostate-specific antigen(PSA) and improves the survival of patients with mHSPC. Several international guidelines recommend apalutamide as the standard treatment for mHSPC. During follow-up, PSA and radionuclide bone imaging are needed for systematic evaluation. Following the application of novel hormonal therapy,PSA was noted to decrease significantly in some patients after treatment. However, radionuclide bone imaging showed progression of bone metastases after 3 mo and with a gradual decrease noted during subsequent follow-up. Ryan
[2] calls this phenomenon “bone flare”. In this study, we retrospectively analyzed the "bone flare" phenomenon during apalutamide treatment in a patient with mHSPC. General information, clinical symptoms, laboratory and imaging examination, treatment, and follow-up data were collected and analyzed. We also share our experience regarding treatment of a patient who had the"bone flare" phenomenon during apalutamide treatment, and provide a reference for its clinical application.
CASE PRESENTATION
Chief complaints
The patient suffer lumbar pain for 1 mo.
History of present illness
On December 16, 2020, a 56-year-old man visited the outpatient clinic of the Department of Urology,Weifang People's Hospital, with a complaint of lumbar pain for 1 mo.
History of past illness
The patient had no relevant history of past illnesses.
Personal and family history
The patient has no relevant personal and family history.
Physical examination
There was nothing lacking that Valentine s Day after all. My father, in a voice quavering with emotion, read the loving message he d sent to my mother fifty-six years earlier. And this time, he could read it to her in person.
It s where he used to live. Gaston is out in the world and on his own now. You can see for yourself how comfortable he was in there. He had everything.
Laboratory examinations
Initial hormonal assay results were as follows: PSA > 100 ng/mL, ALP: 730 U/L. Ultrasound-guided needle biopsy of the prostate. Postoperative pathological results were as follows: poorly differentiated adenocarcinoma of the prostate, Gleason score: 5+4 = 9.
Imaging examinations
Magnetic resonance imaging (MRI) revealed a malignant mass in the peripheral zone of the prostate with multiple bone metastases. Radionuclide bone imaging revealed multiple bone metastases. Prostatespecific membrane antigen (PSMA) positron emission tomography – computed tomography (PET-CT)examination revealed PSMA aggregation in multiple bone sites.
8. Hew down a tree: A tree can symbolize22 an upward trend (Cirlot 347), which does not occur to either of the eldest brothers.Return to place in story.
FINAL DIAGNOSIS
Informed written consent was obtained from the patient for publication of this report and any accompanying images.
Digital rectal examination revealed a significantly enlarged, hard prostate with palpable non-tender nodules on the left side.
13.Handsomer than her sisters:Her beauty shows that Cinderella is more virtuous63 and good than her sisters. In the past, and often still today, physical beauty was considered to reflect the true nature of a person.
Gratitude is a positive emotion, which involves a feeling of emotional indebtedness towards another person; often accompanied by a desire to thank them, or to reciprocate26 for a favour they have done for you
TREATMENT
When apalutamide therapy is used in the treatment of prostate cancer, an increase in metastatic bone lesions on radionuclide bone imaging and MRI; warrants the use of other examinations including PSA,PSMA PET-CT, to determine the efficacy of ongoing treatment, so as to determine the course of treatment for such patients.
OUTCOME AND FOLLOW-UP
The authors declare that they have no conflict of interest.
DISCUSSION
In most patients diagnosed with prostate cancer with distant metastases at the clinic, bone metastasis is the most common. Studies have shown that androgen receptors (AR) play an important role in the development of prostate cancer[3]. Therefore, ARs are an important target for the treatment of prostate cancer. However, with prolonged conventional AR-targeted drug therapy, patients with prostate cancer experience a reduction in therapeutic effect[4]. Presently, research and development of new ARtargeting drugs has become a hotspot in the field of prostate cancer treatment.
Apalutamide, an oral non-steroidal antiandrogen agent that binds directly to the ligand-binding domain of the androgen receptor and prevents androgen receptor translocation, DNA binding, and androgen receptor–mediated transcription[5], has shown good efficacy and safety in clinical practice.The 2020 EAU prostate cancer guidelines recommend ADT in combination with apalutamide and enzalutamide, a new generation of androgen receptor antagonists, as first-line therapy for metastatic prostate cancer. Ryan
[2] reported that after abiraterone treatment for 3 mo, the PSA level decreased by more than 50%, but bone metastasis lesions increase. Furthermore, after 6 mo of continued treatment,bone scan revealed reduced or stable lesions, and this was termed the “bone flare” phenomenon. During treatment, the laboratory results of patients with the bone flare phenomenon showed no significant change in the alkaline phosphatase level, however, PSA level continued to decrease. Our case revealed that bone flare phenomenon also occurs with apalutamide therapy. Some studies have also shown that bone flare occurs in some breast cancer patients with bone metastasis after chemotherapy and other treatments, and is considered to be a sign of effective treatment of bone metastases. Cook
[6]reported that of 22 patients with unequivocal skeletal metastases on baseline scan, flares occurred in 9(41%). Out of 36 high-risk localized prostate cancer patients with normal pre-treatment bone scintigraphy, the scan became positive for metastases at 6 wk in 4 (11%). Furthermore, out of 41 patients, pretreatment scintigraphic abnormalities of uncertain etiology and flares occurred in 8 patients (20%).
The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).
Therefore, during the novel hormonal therapy in mHSPC patients with bone metastasis, it is important to identify whether the treatment is ineffective or whether the bone flare phenomenon is observed when bone scan indicates bone disease progression. This will determine the subsequent treatment strategy for patients. If PSA levels are not reduced after treatment and clinical symptoms worsen, the possibility of disease progression should be considered, and a new treatment strategy should be selected. Otherwise, bone flare should be considered if the PSA level decreases significantly after treatment, and the patient's clinical symptoms improve significantly. In this case, the original treatment was maintained with close follow-up. Bone scan showed increased metastases, but the PSA level decreased significantly. Following PSAM, PET-CT results showed significant improvement in bone metastasis, and the bone flare phenomenon was confirmed.
CONCLUSION
Androgen deprivation therapy (ADT) using novel hormonal therapy (goseraline sustained-release implant 3.6 mg monthly and apalutamide 240 mg/d was initiated on December 24, 2020.
FOOTNOTES
Li KH reviewed the literature, and contributed to manuscript drafting; Du YC, Yu XY and Li YX contributed to manuscript drafting; Zhang XP and Yang DY obtained informed consent; Qiao L was responsible for the revision of the manuscript; and All authors gave final approval for the submitted version.
Based on the results obtained from imaging and histopathology, the final diagnosis was prostate adenocarcinoma (T
N
M
).
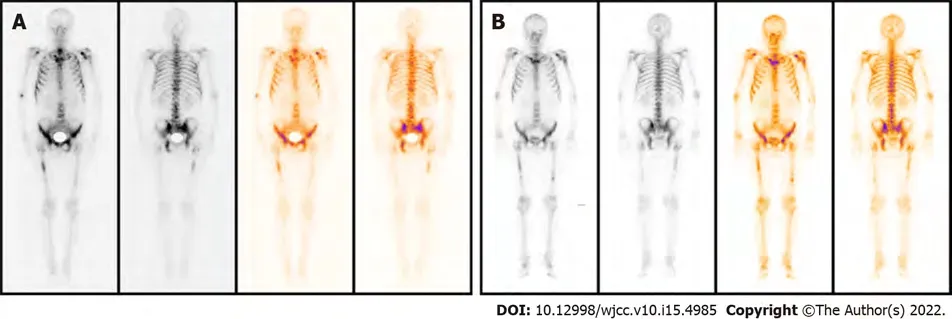
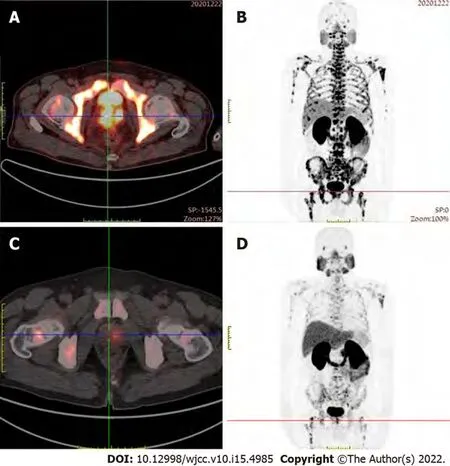
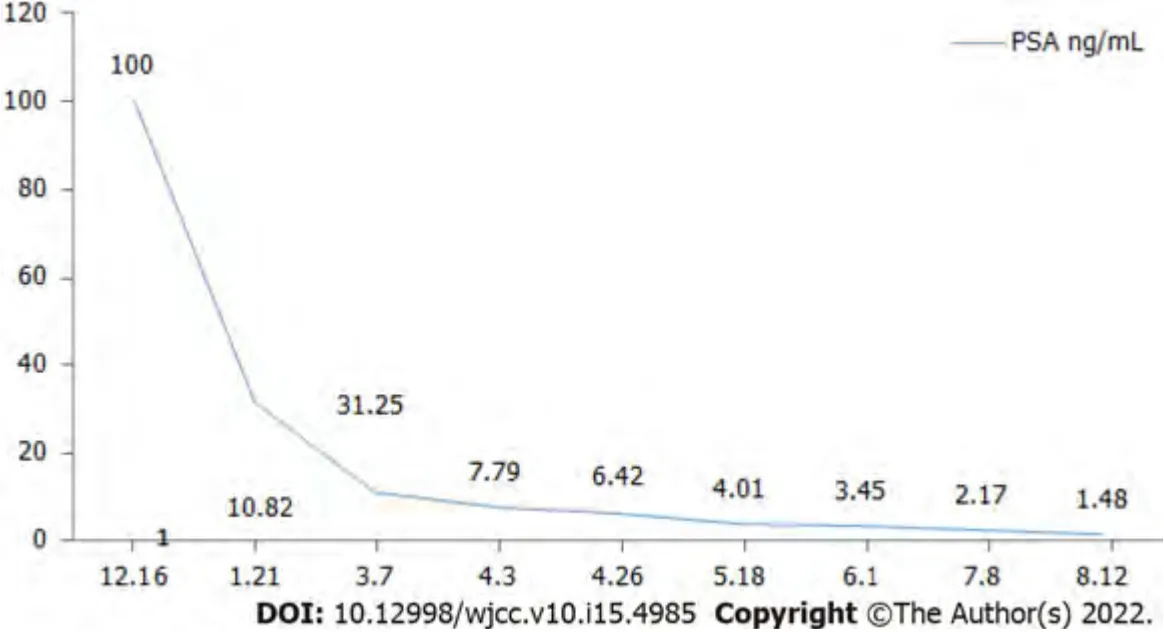
PSA levels and alkaline phosphatase levels were reviewed monthly, and imaging examinations were reviewed every three months. The PSA level decreased significantly during the treatment; however,three months later, radionuclide bone imaging and MRI indicated progression of the bone metastasis(Figure 1). Contrarily, PSMA PET-CT examination showed significantly decreased PSMA aggregation on the bone, indicating improved bone metastases (Figure 2). Considering that the lumbar pain, which he initially presented with, continued to decrease, the treatment strategies were considered to be effective. The original treatment strategies were continued for over 4 mo. The patient's PSA decreased to normal levels (Figure 3), and his clinical symptoms reduced significantly; therefore, treatment was continued.
In the present study, the patient was diagnosed with mHSPC and bone metastasis. The initial treatment strategy was ADT and apalutamide. However, bone flares occurred 3 mo after treatment, and a bone scan showed metastatic progression. However, PSMA PET-CT examination showed that abnormal PSMA aggregation was significantly reduced, and bone metastasis was significantly improved compared to the baseline. Therefore, the temporary phenomenon of increased lesions in the bone scan was considered a bone flare. During treatment, the PSA level decreased significantly, and the alkaline phosphatase level did not change significantly. Vincenza
[7] pointed out that therapy for metastatic disease may lead to healing and new bone formation, which causes an initial increase in tracer uptake (akin to callus formation). This deterioration, followed by subsequent improvement in the bone scan appearance after successful therapy, is defined as a flare response. Due to the shortcomings of the current assessment based on PSA and imaging examinations, more research results show that the changes in the number of circulating tumor cells in peripheral blood can be used as a new means of evaluating efficacy. If the treatment is effective, the number of circulating tumor cells will decline rapidly. The increase or decrease in the number of circulating tumor cells after treatment is also a predictor of patient survival. The prognostic value is significantly better than PSA and imaging examination[8,9]. In the latest PCWG3 study, assessment of circulating tumor cell number was used as an important marker for disease evaluation and to assess drug efficacy[10].
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
China
Ke-Hao Li 0000-0003-2467-6526; Yuan-Cheng Du 0000-0003-2116-5202; Dong-Yu Yang 0000-0002-2194-9878; Xin-Yuan Yu 0000-0003-3147-5474; Xue-Ping Zhang 0000-0001-9245-8833; Yong-Xiang Li 0000-0002-5196-8113;Liang Qiao 0000-0002-7258-0484.
Little boys make too much noise. They d scare the fish, being shouters and laughers and slappers. They d muddy the water, and leave gum wrappers. No -- I d be a fool to let them fish in my pool.
He is like one of the family, faithful and grumpy; but the latter is my grandchildren s fault, for they have teased him; they play at wedding, and want to give him the part of the bridesmaid, and that s too much for him, poor old fellow
Ma YJ
A
Ma YJ
1 Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries.
2018; 68: 394-424 [PMID: 30207593 DOI: 10.3322/caac.21492]
2 Ryan CJ, Shah S, Efstathiou E, Smith MR, Taplin ME, Bubley GJ, Logothetis CJ, Kheoh T, Kilian C, Haqq CM, Molina A, Small EJ. Phase II study of abiraterone acetate in chemotherapy-naive metastatic castration-resistant prostate cancer displaying bone flare discordant with serologic response.
2011; 17: 4854-4861 [PMID: 21632851 DOI:10.1158/1078-0432.CCR-11-0815]
3 Dai C, Heemers H, Sharifi N. Androgen Signaling in Prostate Cancer.
2017; 7 [PMID:28389515 DOI: 10.1101/cshperspect.a030452]
4 Paschalis A, Sharp A, Welti JC, Neeb A, Raj GV, Luo J, Plymate SR, de Bono JS. Alternative splicing in prostate cancer.
2018; 15: 663-675 [PMID: 30135575 DOI: 10.1038/s41571-018-0085-0]
5 Clegg NJ, Wongvipat J, Joseph JD, Tran C, Ouk S, Dilhas A, Chen Y, Grillot K, Bischoff ED, Cai L, Aparicio A, Dorow S, Arora V, Shao G, Qian J, Zhao H, Yang G, Cao C, Sensintaffar J, Wasielewska T, Herbert MR, Bonnefous C, Darimont B, Scher HI, Smith-Jones P, Klang M, Smith ND, De Stanchina E, Wu N, Ouerfelli O, Rix PJ, Heyman RA, Jung ME,Sawyers CL, Hager JH. ARN-509: a novel antiandrogen for prostate cancer treatment.
2012; 72: 1494-1503[PMID: 22266222 DOI: 10.1158/0008-5472.CAN-11-3948]
6 Cook GJ, Venkitaraman R, Sohaib AS, Lewington VJ, Chua SC, Huddart RA, Parker CC, Dearnaley DD, Horwich A. The diagnostic utility of the flare phenomenon on bone scintigraphy in staging prostate cancer.
2011; 38: 7-13 [PMID: 20697891 DOI: 10.1007/s00259-010-1576-0]
7 Conteduca V, Poti G, Caroli P, Russi S, Brighi N, Lolli C, Schepisi G, Romeo A, Matteucci F, Paganelli G, Marchetti P,De Giorgi U. Flare phenomenon in prostate cancer: recent evidence on new drugs and next generation imaging.
2021; 13: 1758835920987654 [PMID: 33708265 DOI: 10.1177/1758835920987654]
8 Thalgott M, Heck MM, Eiber M, Souvatzoglou M, Hatzichristodoulou G, Kehl V, Krause BJ, Rack B, Retz M, Gschwend JE, Andergassen U, Nawroth R. Circulating tumor cells versus objective response assessment predicting survival in metastatic castration-resistant prostate cancer patients treated with docetaxel chemotherapy.
2015;141: 1457-1464 [PMID: 25708944 DOI: 10.1007/s00432-015-1936-z]
9 Vogelzang NJ, Fizazi K, Burke JM, De Wit R, Bellmunt J, Hutson TE, Crane E, Berry WR, Doner K, Hainsworth JD,Wiechno PJ, Liu K, Waldman MF, Gandhi A, Barton D, Jungnelius U, Fandi A, Sternberg CN, Petrylak DP. Circulating Tumor Cells in a Phase 3 Study of Docetaxel and Prednisone with or without Lenalidomide in Metastatic Castrationresistant Prostate Cancer.
2017; 71: 168-171 [PMID: 27522164 DOI: 10.1016/j.eururo.2016.07.051]
10 Scher HI, Morris MJ, Stadler WM, Higano C, Basch E, Fizazi K, Antonarakis ES, Beer TM, Carducci MA, Chi KN, Corn PG, de Bono JS, Dreicer R, George DJ, Heath EI, Hussain M, Kelly WK, Liu G, Logothetis C, Nanus D, Stein MN,Rathkopf DE, Slovin SF, Ryan CJ, Sartor O, Small EJ, Smith MR, Sternberg CN, Taplin ME, Wilding G, Nelson PS,Schwartz LH, Halabi S, Kantoff PW, Armstrong AJ; Prostate Cancer Clinical Trials Working Group 3. Trial Design and Objectives for Castration-Resistant Prostate Cancer: Updated Recommendations From the Prostate Cancer Clinical Trials Working Group 3.
2016; 34: 1402-1418 [PMID: 26903579 DOI: 10.1200/JCO.2015.64.2702]
 World Journal of Clinical Cases2022年15期
World Journal of Clinical Cases2022年15期
- World Journal of Clinical Cases的其它文章
- Diet and intestinal bacterial overgrowth: Is there evidence?
- Spontaneous liver rupture following SARS-CoV-2 infection in late pregnancy: A case report
- Metastasis of liver cancer to the thyroid after surgery: A case report
- Solitary primary pulmonary synovial sarcoma: A case report
- Knot impingement after arthroscopic rotator cuff repair mimicking infection: A case report
- Clear aligner treatment for a four-year-old patient with anterior crossbite and facial asymmetry: A case report