
Neurocutaneous melanosis with an intracranial cystic-solid meningeal melanoma in an adult: A case report and review of literature
2022-06-22 08:49:24BoChuanLiuYuBoWangZhuangLiuYanJiaoXianFengZhang
World Journal of Clinical Cases 2022年15期
INTRODUCTION
Neurocutaneous melanosis (NCM) is a rare congenital, nonhereditary neurocutaneous syndrome that mainly occurs in children; adult NCM is very rare. Specifically, NCM is a rare combined abnormality of the skin and central nervous system (CNS)[1], mainly presenting as congenital melanocytic nevi with benign or malignant melanoma of the central nervous system[2]. NCM is a neuroectodermal dysplasia believed to arise from an embryological defect in the migration of melanoblasts from the neural crest to the leptomeninges and skin[3]; it was first described by Rokitanki in 1861[4]. Patients with NCM usually have neurological symptoms at an early age. Most patients have a poor prognosis once symptoms occur,regardless of whether the CNS tumors are benign or malignant; in most cases, the disease is fatal within 3 years of onset[5]. Primary malignant melanoma in the central nervous system is usually a single solid mass, and melanoma with large cystic changes is extremely rare. Here, we describe a rare adult NCM complicated with intracranial cystic-solid malignant melanoma and review the relevant literature to discuss the clinical features, diagnosis, treatment and prognosis.
CASE PRESENTATION
Chief complaints
The patient was admitted to our department with intermittent headache for 1 mo.
History of present illness
A 41-year-old woman was admitted to the hospital with intermittent headache for 1 mo. The headache could not be relieved by rest. There were no obvious symptoms of nausea, vomiting and epilepsy.
History of past illness
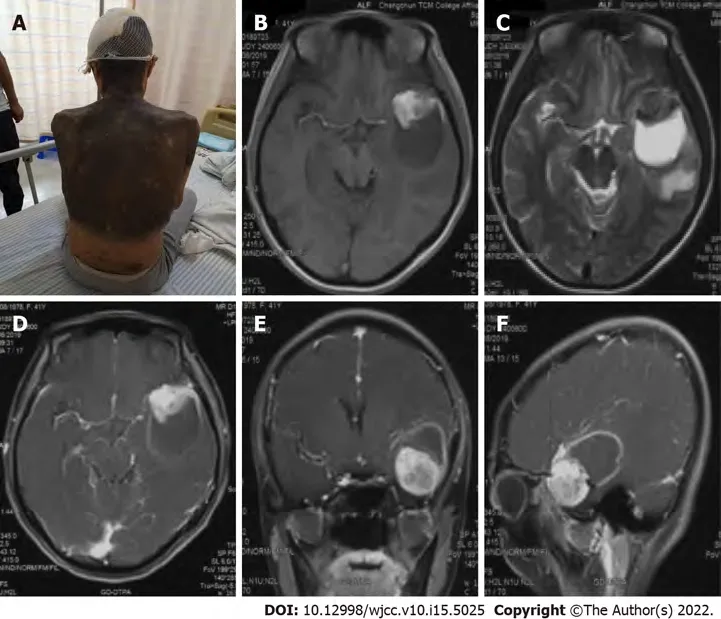
The patient was born with diffuse melanosis of the skin, mainly covering the back of the trunk,shoulders and neck, with multiple satellite nevi on the limbs and a few hairs on the surface of the nevi in the first few years after birth (Figure 1A). The lesion was considered to be a birthmark and had not been treated. No malignant clinical signs, such as enlargement, ulcers, bleeding or itching, were observed in the pigmented area as the patient aged.
Once upon a time there lived a King and Queen, who were the best creatures in the world, and so kind-hearted that they could not bear to see their subjects want for anything
Personal and family history
There was no past history of skin or CNS disease or malignant tumor. The patient had no history of surgery, and her parents and children had no history of congenital nevi or melanoma.
Physical examination
The patient has diffuse melanosis of the skin, mainly covering the back of the trunk, shoulders and neck,with multiple satellite nevi on the limbs and a few hairs on the surface of the nevi. Examination of her nervous system revealed no obvious abnormalities.
Laboratory examinations
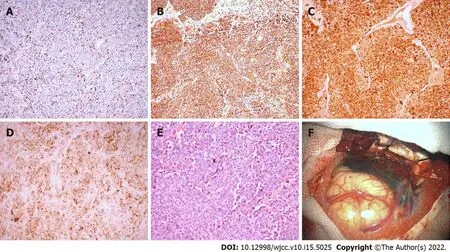
Laboratory examinations such as routine blood tests, routine urine tests and blood biochemistry were normal. The pathological results showed malignant melanoma. Immunohistochemistry results were as follows: Ki-67 (+30%), S-100 (+), HMB45 (+), Vimentin (+); all other markers were negative (Figure 2).
Imaging examinations
Some literature reports have shown that when intracranial lesions of NCM manifest as solid melanoma foci, they are usually asymptomatic[20]. When solid lesions involve the amygdala, pons, and cerebellum, most have a stable or benign course until they develop into malignant melanoma[21]. This may be one reason why NCM does not develop in some patients until adulthood.
FINAL DIAGNOSIS
We ultimately diagnosed this patient with NCM with meningeal melanoma.
If the elves work and results follow the same pattern already described, the number of shoes increases greatly each night starting with 1 and following a sequence of:2, 4, 8, 16, 32, 64, 128, 256, 512, etc
TREATMENT
The patient underwent surgery to remove the intracranial mass after admission. During the operation,the tumor appeared blackish brown (the peripheral leptomeninges were also stained black), with lightyellow sac fluid inside, and the blood supply to the tumor was extremely rich. First, the cystic fluid was drawn out, and the lesion was then gradually separated along its periphery until it was completely removed. The pathological results showed malignant melanoma. Immunohistochemistry results were as follows: Ki-67 (+30%), S-100 (+), HMB45 (+), Vimentin (+); all other markers were negative (Figure 2).
OUTCOME AND FOLLOW-UP
The patient was in good condition after the operation; she refused further radiotherapy and chemotherapy and was discharged on the tenth day after the operation. Five months after the operation,the patient went to a local hospital due to unconsciousness after severe headache and died of ineffective treatment. Her death was considered to be due to obstructive hydrocephalus from tumor progression.
Informed written consent has been obtained from the patient for publication of this report and any accompanying images.
DISCUSSION
We report an adult female patient with a congenital melanocytic nevus (CMN) on her neck, shoulder and back. A space-occupying lesion in the left temporal lobe was found during a magnetic resonance imaging (MRI) scan of her head. The tumor was resected en bloc under microscopy, and subsequent histopathology and immunohistochemistry analyses revealed malignant melanoma. Adult NCM and cystic-solid malignant melanomas are very rare. Our present case report may provide an additional reference that can serve as a potential guide for clinicians and radiologists.
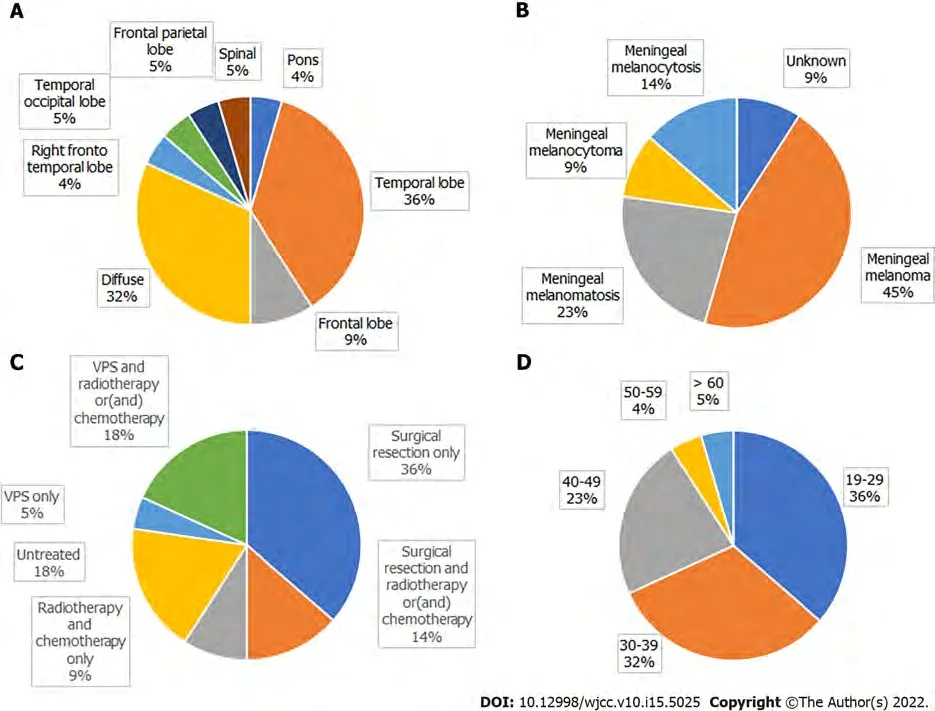
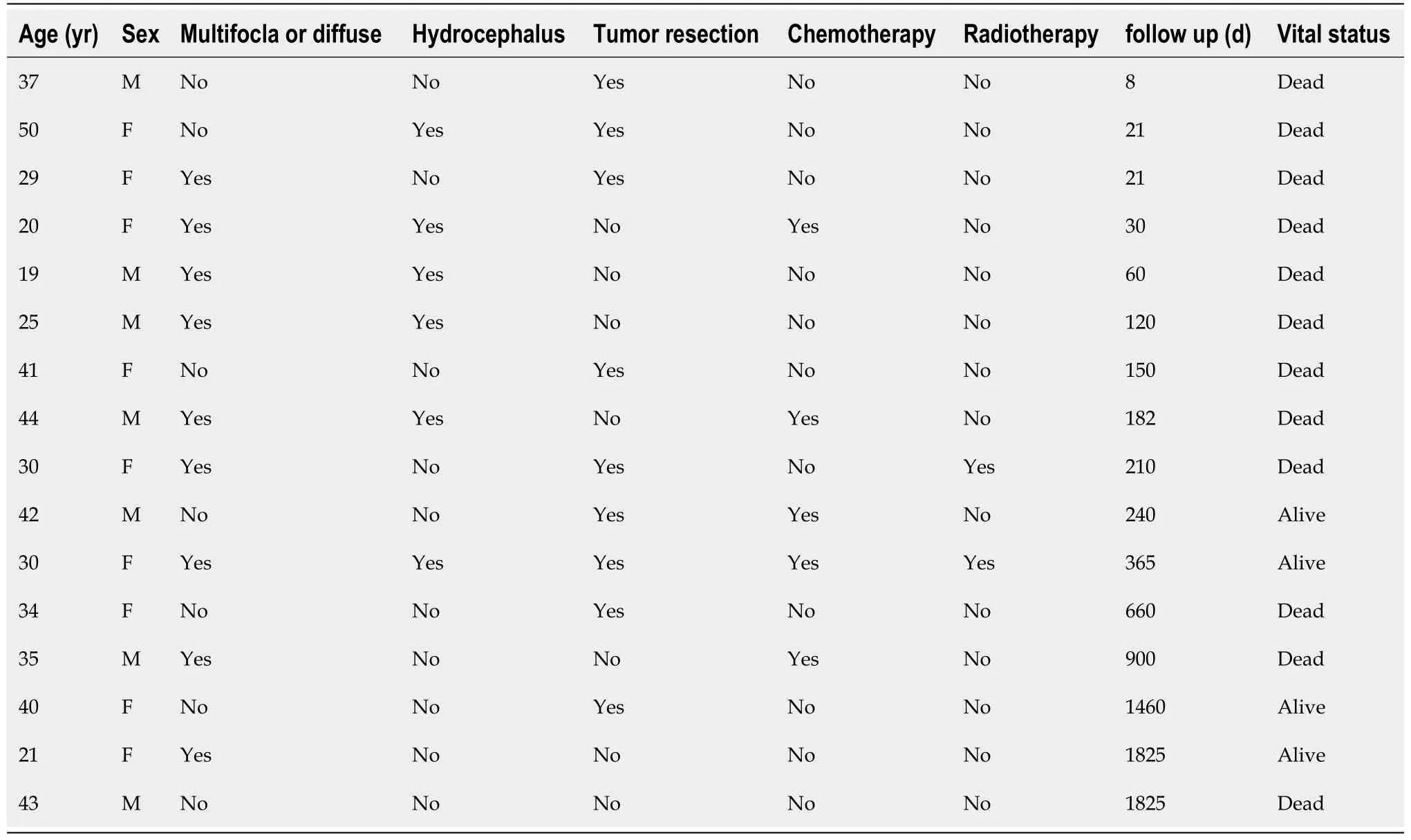
A search of the literature revealed 22 adult NCM cases, including our patient (Table 1); there were 13 males and 9 females, with a male to female ratio of 1.444:1. The mean patient age was 34.13 ± 11.41 years(range: 19-67 years). Congenital melanocytic nevus was most commonly located in the trunk (71.4%),followed by multiple congenital nevi (18.1%). Intracranial hypertension (45%) and epileptic seizures(40%) were the most common first clinical symptoms; others included disturbances of consciousness,movement disorders, and paresthesia. Imaging showed that the lesions were mainly located in the temporal lobe, frontal lobe, and pons. Cystic changes in intracranial melanoma tumors occurred in two patients.
In PubMed, we searched for adult NCM cases published between 1990 and 2020. “Neurocutaneous melanosis” was used as the key word and “Adult: 19 + years” as the qualification, and reports without detailed clinical data were excluded. In addition, references cited in selected articles were manually searched and reviewed to identify other potentially eligible studies. Patient data were extracted, and the clinical data were described and analyzed.
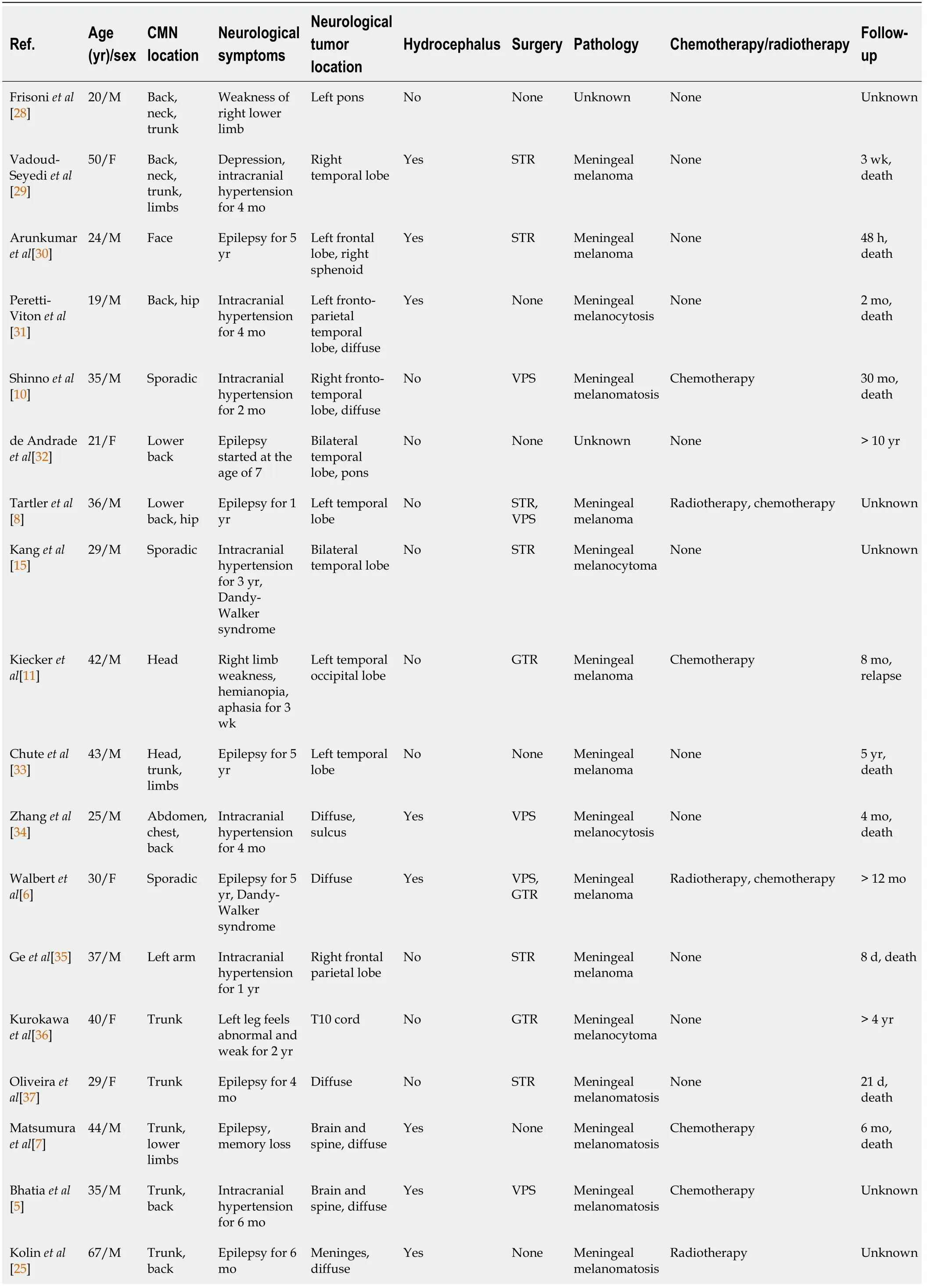

Subtotal resection of tumors occurred in 6 cases, gross total resection in 5 cases, ventriculoperitoneal shunt in 4 cases, gross total tumor resection plus ventriculoperitoneal shunt in 1 case, and subtotal tumor resection plus ventriculoperitoneal shunt in 1 case. Three patients received postoperative chemotherapy, 2 received postoperative radiotherapy plus chemotherapy, and 2 received chemotherapy without surgery; 4 did not receive treatment. Among those receiving chemotherapy, 5 patients were treated with temozolomide[5-9], 1 patient received combined immunochemotherapy[10], and 1 patient received adjuvant chemotherapy with fotemustine[11]. According to the pathological results, 9 cases of meningeal melanoma, 5 cases of meningeal melanomatosis, 2 cases of meningeal melanocytoma, 3 cases of meningeal melanocytosis, and 3 cases of unknown pathology were diagnosed (Figure 3).
The survival time of 3 patients was not mentioned. There was one special case of a patient who had seizures at the age of 7 and was still alive at the age of 21. The survival period of patients after the appearance of symptoms was 4.75 mo to more than 6 years, and 14 patients (82%) died within 3 years.
According to previous reports, patients with NCM generally develop neurological symptoms at an early age, and most of them die within 3 years after the onset of symptoms. Adult NCM is very rare[5].The vast majority of patients with NCM are sporadic cases, with few familial cases being reported.Approximately 2/3 of patients with NCM have a giant CMN, and the remaining 1/3 have multiple small lesions[12]. Patients with a giant CMN located on the posterior axis of the trunk and multiple satellite nevi are at higher risk for NCM[13]. The current diagnostic criteria for NCM were revised by Kadonaga
[14] in 1991 as follows: (1) Large or multiple congenital nevi are observed in association with meningeal melanosis or melanoma. Large refers to a lesion size equal to or greater than 20 cm in diameter in an adult; in neonates and infants, large is defined as a size of 9 cm in the head or 6 cm in the body. Multiple signifies three or more lesions; (2) There is no evidence of cutaneous melanoma, except in patients in whom the examined areas of the meningeal lesions were histologically benign; and (3)There is no evidence of meningeal melanoma, except in patients in whom the cutaneous lesions were histologically benign. According to the above criteria, our patient was diagnosed with NCM. As NCM is very rare, there is no specific incidence. Men seem to be more susceptible to the disease than women, or it is possible that male patients have a greater chance of surviving to adulthood than female patients.
What a sad man, Diana thought when she first saw him. The future Princess was intrigued3 to finally meet the most eligible4 bachelor in England, thought she was not impressed with his five-foot-ten-inch height, thinking to herself that she would tower over him in high heels. But Diana would later say that she admired his beautiful blue eyes.
Last year I was put into a lower-level math class at school. The reason I was in this class had nothing to do with my intellect or math skills. I am blind. The school decided1 that it would be better for me to learn at a lower level because it takes me a great deal longer to complete assignments and grasp visual concepts.
Most intracranial meningeal melanomas are solid masses, and some tumors may have small necrotic cysts inside; cystic-solid malignant melanoma is very rare. In the literature, there were 2 patients with similar lesions. Kang
[15] reported a patient with NCM who had a cystic-solid meningeal melanocytoma in the left temporal lobe, a dermoid cyst in the right temporal lobe, and Dandy-Walker syndrome. Ma
[16] reported a patient with NCM who had cystic-solid malignant melanoma in the left temporal lobe and survived for 22 mo after partial resection of the tumor. Combined with our patient, melanoma with large cystic degeneration occurred only in adult patients, and whether tumors were benign or malignant did not seem to have an absolute relationship with cystic degeneration. Due to limited data, it is impossible to clarify the impact of cystic changes in NCM intracranial tumors on the prognosis of patients.
In general, when a cystic mass develops in the central nervous system, the cystic component is caused by tumor necrosis or degeneration. The tumor cyst of our patient was mainly filled with a light-yellow liquid. In the literature, we found that the cysts of some tumors may constitute a nutrient reservoir for brain tumors to ensure that tumor metabolism and tumor cell synthesis can be carried out. Through a component analysis, serum was reported as one of the possible sources of nutrients in most cystic fluids,which may be due to the destruction of the blood–brain barrier by the tumor[17].
Clinical presentations of NCM are nonspecific and vary depending on the tumor site, size and invasion site; these mainly include epilepsy, intracranial hypertension, dyskinesia, and hydrocephalus[9]. Hydrocephalus has been reported in approximately two-thirds of cases and occurs as a result of the obstruction of cerebrospinal fluid (CSF) flow due to melanotic infiltration of arachnoid villi and leptomeninges[12]. Based on our data, the incidence of hydrocephalus in adults was 42.8%. According to this set of data, the peak of neurological symptoms in adult patients is in the third 10 years of life. In addition, the association between Dandy-Walker syndrome and NCM is rare and complex. It has been reported that approximately 8%-10% of cases of Dandy-Walker syndrome are related to NCM[18]. There are currently two theories describing the connection between NCM and Dandy-Walker syndrome. It is thought that melanotic infiltration interferes with the capacity of primitive meningeal cells to induce the normal migration of neurons, deposition of extracellular matrix, and development of normal CSF pathways, leading to posterior fossa cyst formation and vermian dysgenesis. Alternatively, Omar
[19] suggested that melanosis interferes with the ectodermal-mesodermal interaction, causing an abnormal formation of the fourth ventricle and cerebellum.
MRI examination of the head revealed a mass with intramural cysts located on the left temporal lobe.The solid part of the tumor was hyperintense on T1-weighted images and hypointense on T2-weighted images, and the cystic components showed the opposite. The lesion had a clear boundary of approximately 4.7 cm x 3.6 cm and was surrounded by peritumoral edema (Figure 1B and C). After the injection of a contrast agent (Gd-DTPA), obvious heterogeneous enhancement was observed in the solid part, while the cystic part showed abnormal ring-shaped enhancement (Figure 1D-F).
At present, MRI is the first-choice imaging approach for diagnosing central nervous system diseases in NCM patients, although it cannot distinguish benign and malignant intracranial tumors. In fact, as melanin pigment is inherently paramagnetic, typical NCM lesions usually exhibit high intensity on T1-weighted images and low intensity to isointensity on T2-weighted images[22]. Due to differences in the melanin content, intracranial melanomas are divided into the melanin type, nonmelanin type, mixed type (melanin type plus nonmelanin type) and blood type according to MRI characteristics[23]. Because NCM does not have a unique clinical manifestation, patients with a giant CMN without neurological symptoms should be examined regularly to rule out the disease. It has been reported that the most common melanin deposits occur in the temporal lobe (especially the amygdala), cerebellum and pons[24]. However, lesions were found in the frontal lobe of some patients, as revealed by our analysis.
There are reports in the literature indicating that CSF can also be used to diagnose NCM. Kolin
[25] reported on a patient they diagnosed with CSF, which they claimed was the first case report of a diagnosis of primary leptomeningeal melanomatosis (PLM) with an NRAS mutation using a CSF sample for both confirmatory immunocytochemistry and molecular testing. However, in regard to the diagnosis of NCM, we believe that imaging examinations have the advantages of convenience and noninvasiveness. As a result, diagnostic imaging is still the first choice, and CSF examination can be used to further determine whether the lesion is benign or malignant.
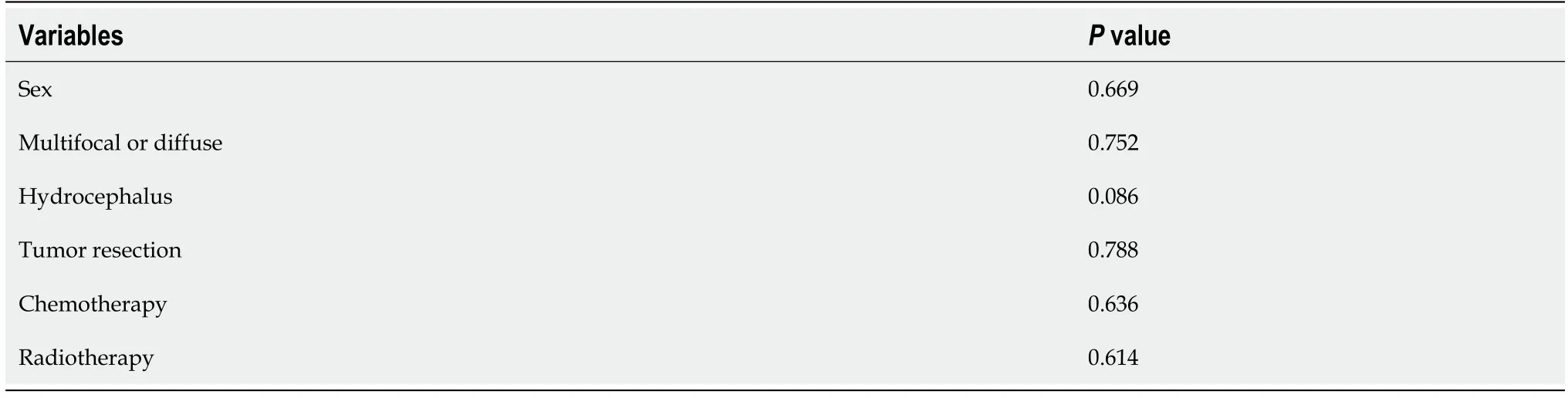
We have tried to analyze the survival data. We excluded the patients without follow-up and the patients died within 3 d after the surgery, 16 patients were included in the survival analysis. Then we divided the patients into different groups (Table 2) and use Kaplan-Meier graph to estimate the overall survival in different groups. The differences between the curves were analyzed by log-rank test,statistical significance was defined as
< 0.05. Unfortunately, we have not found any independent prognostic factors associated with overall survival (Table 3).
Neurocutaneous melanosis usually has a very poor prognosis. The 2016 classification by the World Health Organization categorizes central nervous system melanocyte lesions into meningeal melanocytosis, meningeal melanomatosis, meningeal melanocytoma and meningeal melanoma, where meningeal melanocytosis is considered benign and meningeal melanocytoma is considered relatively benign. The prognosis of meningeal melanoma is very poor. Moreover, the prognosis of patients with NCM is poor, even if the intracranial lesion is diagnosed as benign melanocytosis[16]. According to the literature, most patients die of benign melanocyte overgrowth or malignant transformation within 3 years after symptom onset[27]. In the literature, 15 patients died during follow-up (71%), the survival status of 3 patients was unknown, and 3 patients survived for a long time.
Due to the rarity of NCM, a standard treatment approach for this disease has not yet been established. The current treatment options are mainly microsurgery, chemotherapy, immunotherapy,gene therapy, ventricular-peritoneal shunt and comprehensive treatment. However, melanoma in some patients is diffuse and cannot be removed surgically, and it seems that the effects of radiotherapy and chemotherapy cannot effectively extend the life of patients. In the current study, mutations in codon 61 of the NRAS gene were found in most cases. However, there are currently no established targeted therapies for patients with NRAS-mutated melanomas; BRAF inhibitors and MEK inhibitors may be used for treatment, but their effects and safety remain to be determined[26].
The plane? Dana asked. Who cares about the plane? How could you be so cold? That was an old man; he could have been your grandfather! How would you like it if everyone just stepped over your grandfather and went on their way?
CONCLUSION
In summary, we report an adult NCM patient and summarize 21 known cases. NCM is relatively rare,especially in adult patients. Among adult patients, the proportion of male patients is higher, and most patients are found to have CMN in the trunk of the body. Therefore, patients with CMN should remain vigilant and undergo regular imaging examinations. At present, MRI is the first-choice imaging approach for diagnosing central nervous system diseases in NCM patients. Most patients develop symptoms when they are young. Although some patients may not have central nervous system symptoms until adulthood, once symptoms appear, the prognosis is poor, regardless of whether the intracranial lesions are benign or malignant. Currently, effective treatments are still lacking. Thus, more case reports describing NCM, as well as long-term follow-up studies, are warranted to fully understand NCM in the adult population. To address these limitations, our present case report provides an additional reference among the few available that can serve as a potential guide for clinicians and radiologists.
FOOTNOTES
Liu BC and Wang YB contributed equally to this work; Liu BC and Zhang XF diagnosed the patient; Liu BC analyzed the literature data; and All authors wrote and revised the manuscript and issued the final approval for the version to be submitted.
Fortunately one of the King s servants had become very partial to the young huntsmen, and hearing of the trial they were to be put to, he went to them and said: The Lion wants to persuade the King that you are only girls ; and then told them all the plot
Then the young tailor stepped boldly to the front and said, The Princess has one silver and one golden hair on her head, and those are the two colours
The books travelled all over the world, and some of them came into the hands of the emperor; and he sat in his golden chair, and, as he read, he nodded his approval every moment, for it pleased him to find such a beautiful description of his city, his palace, and his gardens
All authors declare that there are no any conflicts of interest.
The authors have read the CARE Checklist(2016), and the manuscript was prepared and revised according to the CARE Checklist(2016).
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Simon had got the better of them, and done them out of fifty gold pieces, they flew into such a rage that they made up their minds to kill him, and, seizing their weapons for this purpose, went to his house
China
An Italian version of the tale, The Most Sensitive Woman, offers three highly sensitive women, but the prince chooses the one with the highest sensitivity. The first has suffered agonies from the pulling of one single hair from her head while brushing it. The second is in pain from sleeping on a wrinkle in her sheets. The third and final woman, the most sensitive, has a serious injury from a jasmine petal9 falling onto her foot.Return to place in story. #p#
Bo-Chuan Liu 0000-0003-4933-2295; Yu-Bo Wang 0000-0002-3404-0225; Zhuang Liu 0000-0003-4065-6920; Yan Jiao 0000-0002-2471-6260; Xian-Feng Zhang 0000-0001-8958-2585.
Ma YJ
A
Ma YJ
1 G?nül M, Soylu S, Gül U, Aslan E, Unal T, Ergül G. Giant congenital melanocytic naevus associated with Dandy-Walker malformation, lipomatosis and hemihypertrophy of the leg.
2009; 34: e106-e109 [PMID: 19438567 DOI: 10.1111/j.1365-2230.2008.03191.x]
2 Agero AL, Benvenuto-Andrade C, Dusza SW, Halpern AC, Marghoob AA. Asymptomatic neurocutaneous melanocytosis in patients with large congenital melanocytic nevi: a study of cases from an Internet-based registry.
2005; 53: 959-965 [PMID: 16310055 DOI: 10.1016/j.jaad.2005.07.046]
3 Scattolin MA, Lin J, Peruchi MM, Rocha AJ, Masruha MR, Vilanova LC. Neurocutaneous melanosis: follow-up and literature review.
2011; 38: 313-318 [PMID: 21489630 DOI: 10.1016/j.neurad.2011.02.007]
4 Taboada-Suárez A, Brea-García B, Suárez-Pe?aranda JM, Couto-González I. Neurocutaneous melanosis in association with proliferative skin nodules.
2011; 28: 681-684 [PMID: 21995739 DOI:10.1111/j.1525-1470.2011.01383.x]
5 Bhatia R, Kataria V, Vibha D, Kakkar A, Prasad K, Mathur S, Garg A, Bakhshi S. Mystery Case: Neurocutaneous melanosis with diffuse leptomeningeal malignant melanoma in an adult.
2016; 86: e75-e79 [PMID: 26903493 DOI: 10.1212/WNL.0000000000002396]
6 Walbert T, Sloan AE, Cohen ML, Koubeissi MZ. Symptomatic neurocutaneous melanosis and Dandy-Walker malformation in an adult.
2009; 27: 2886-2887 [PMID: 19398571 DOI: 10.1200/JCO.2008.21.5830]
7 Matsumura M, Okudela K, Tateishi Y, Umeda S, Mitsui H, Suzuki T, Nakayama T, Inayama Y, Ohashi K.Leptomeningeal melanomatosis associated with neurocutaneous melanosis: an autopsy case report.
2015; 65:100-105 [PMID: 25521302 DOI: 10.1111/pin.12238]
8 Tartler U, Mang R, Schulte KW, Hengge U, Megahed M, Reifenberger J. [Neurocutaneous melanosis and malignant melanoma].
2004; 55: 971-974 [PMID: 15365641 DOI: 10.1007/s00105-004-0807-3]
9 Alessandro L, Blaquier JB, Bártoli J, Diez B. Diagnostic and therapeutic approach for neurocutaneous melanosis in a young adult.
2019; 34: 336-338 [PMID: 27939117 DOI: 10.1016/j.nrl.2016.09.008]
10 Shinno K, Nagahiro S, Uno M, Kannuki S, Nakaiso M, Sano N, Horiguchi H. Neurocutaneous melanosis associated with malignant leptomeningeal melanoma in an adult: clinical significance of 5-S-cysteinyldopa in the cerebrospinal fluid---case report.
2003; 43: 619-625 [PMID: 14723271 DOI: 10.2176/nmc.43.619]
11 Kiecker F, Hofmann MA, Audring H, Brenner A, Labitzke C, Sterry W, Trefzer U. Large primary meningeal melanoma in an adult patient with neurocutaneous melanosis.
2007; 109: 448-451 [PMID: 17382464 DOI:10.1016/j.clineuro.2007.02.004]
12 Sharouf F, Zaben M, Lammie A, Leach P, Bhatti MI. Neurocutaneous melanosis presenting with hydrocephalus and malignant transformation: case-based update.
2018; 34: 1471-1477 [PMID: 29948137 DOI:10.1007/s00381-018-3851-5]
13 Jakchairoongruang K, Khakoo Y, Beckwith M, Barkovich AJ. New insights into neurocutaneous melanosis.
2018; 48: 1786-1796 [PMID: 30074086 DOI: 10.1007/s00247-018-4205-x]
14 Kadonaga JN, Frieden IJ. Neurocutaneous melanosis: definition and review of the literature.
1991;24: 747-755 [PMID: 1869648 DOI: 10.1016/0190-9622(91)70115-i]
15 Kang SG, Yoo DS, Cho KS, Kim DS, Chang ED, Huh PW, Kim MC. Coexisting intracranial meningeal melanocytoma,dermoid tumor, and Dandy-Walker cyst in a patient with neurocutaneous melanosis. Case report.
2006; 104:444-447 [PMID: 16572661 DOI: 10.3171/jns.2006.104.3.444]
16 Ma M, Ding ZL, Cheng ZQ, Wu G, Tang XY, Deng P, Wu JD. Neurocutaneous Melanosis in an Adult Patient with Intracranial Primary Malignant Melanoma: Case Report and Review of the Literature.
2018; 114: 76-83[PMID: 29530698 DOI: 10.1016/j.wneu.2018.02.007]
17 Dahlberg D, Struys EA, Jansen EE, M?rkrid L, Midttun ?, Hassel B. Cyst Fluid From Cystic, Malignant Brain Tumors: A Reservoir of Nutrients, Including Growth Factor-Like Nutrients, for Tumor Cells.
2017; 80: 917-924 [PMID:28327992 DOI: 10.1093/neuros/nyw101]
18 Danial-Mamlouk C, Mamlouk MD, Handwerker J, Hasso AN. Case 220: Neurocutaneous Melanosis.
2015;276: 609-613 [PMID: 26203712 DOI: 10.1148/radiol.2015131288]
19 Omar AT, Bagnas MAC, Del Rosario-Blasco KAR, Diestro JDB, Khu KJO. Shunt Surgery for Neurocutaneous Melanosis with Hydrocephalus: Case Report and Review of the Literature.
2018; 120: 583-589.e3 [PMID:30205217 DOI: 10.1016/j.wneu.2018.09.002]
20 Bekiesińska-Figatowska M, Sawicka E, ?ak K, Szczygielski O. Age related changes in brain MR appearance in the course of neurocutaneous melanosis.
2016; 85: 1427-1431 [PMID: 27423683 DOI: 10.1016/j.ejrad.2016.05.014]
21 Kim SJ, Kim JH, Son B, Yoo C. A giant congenital melanocytic nevus associated with neurocutaneous melanosis.
2014; 24: 177-184 [PMID: 24173435 DOI: 10.1007/s00062-013-0217-y]
22 Striano P, Consales A, Severino M, Prato G, Occella C, Rossi A, Cama A, Nozza P, Baglietto MG. A 3-year-old boy with drug-resistant complex partial seizures.
2012; 22: 725-728 [PMID: 22925082 DOI:10.1111/j.1750-3639.2012.00619.x]
23 Isiklar I, Leeds NE, Fuller GN, Kumar AJ. Intracranial metastatic melanoma: correlation between MR imaging characteristics and melanin content.
1995; 165: 1503-1512 [PMID: 7484597 DOI:10.2214/ajr.165.6.7484597]
24 Taylor DR, Wait SD, Wheless JW, Boop FA. Amygdalar neuromelanosis intractable epilepsy without leptomeningeal involvement.
2013; 12: 21-24 [PMID: 23641959 DOI: 10.3171/2013.3.PEDS12502]
25 Kolin DL, Geddie WR, Ko HM. CSF cytology diagnosis of NRAS-mutated primary leptomeningeal melanomatosis with neurocutaneous melanosis.
2017; 28: 235-238 [PMID: 27696542 DOI: 10.1111/cyt.12366]
26 Küsters-Vandevelde HV, Willemsen AE, Groenen PJ, Küsters B, Lammens M, Wesseling P, Djafarihamedani M, Rijntjes J, Delye H, Willemsen MA, van Herpen CM, Blokx WA. Experimental treatment of NRAS-mutated neurocutaneous melanocytosis with MEK162, a MEK-inhibitor.
2014; 2: 41 [PMID: 24713450 DOI:10.1186/2051-5960-2-41]
27 Furtado S, Furtado SV, Ghosal N, Hegde AS. Fatal leptomeningeal melanoma in neurocutaneous melanosis.
2012; 29: 358-361 [PMID: 21906139 DOI: 10.1111/j.1525-1470.2011.01424.x]
28 Frisoni GB, Gasparotti R, Di Monda V. Giant congenital nevus and chronic progressive ascending hemiparesis (Mills syndrome). Report of a case.
1992; 13: 259-263 [PMID: 1624284 DOI: 10.1007/BF02224400]
29 Vadoud-Seyedi R, Heenen M. Neurocutaneous melanosis.
1994; 188: 62-65 [PMID: 8305762 DOI:10.1159/000247089]
30 Arunkumar MJ, Ranjan A, Jacob M, Rajshekhar V. Neurocutaneous melanosis: a case of primary intracranial melanoma with metastasis.
2001; 13: 52-54 [PMID: 11292138 DOI: 10.1053/clon.2001.9215]
31 Peretti-Viton P, Gorincour G, Feuillet L, Lambot K, Brunel H, Raybaud C, Pellissier JF, Chérif AA. Neurocutaneous melanosis: radiological-pathological correlation.
2002; 12: 1349-1353 [PMID: 12042938 DOI:10.1007/s00330-001-1195-z]
32 de Andrade DO, Dravet C, Raybaud C, Broglin D, Laguitton V, Girard N. An unusual case of neurocutaneous melanosis.
2004; 6: 145-152 [PMID: 15504713]
33 Chute DJ, Reiber K. Three unusual neuropathologic-related causes of sudden death.
2008; 53: 734-738[PMID: 18471225 DOI: 10.1111/j.1556-4029.2008.00696.x]
34 Zhang W, Miao J, Li Q, Liu R, Li Z. Neurocutaneous melanosis in an adult patient with diffuse leptomeningeal melanosis and a rapidly deteriorating course: case report and review of the literature.
2008; 110: 609-613[PMID: 18407407 DOI: 10.1016/j.clineuro.2008.02.022]
35 Ge P, Wang H, Zhong Y, Chen B, Ling F, Luo Y. Rare presentation in an adult patient with neurocutaneous melanosis.
2010; 49: 1311-1313 [PMID: 20964655 DOI: 10.1111/j.1365-4632.2009.04347.x]
36 Kurokawa R, Kim P, Kawamoto T, Matsuda H, Hayashi S, Yamazaki S, Hatamochi A, Mori S, Shimoda M, Kubota K.Intramedullary and retroperitoneal melanocytic tumor associated with congenital blue nevus and nevus flammeus: an uncommon combination of neurocutaneous melanosis and phacomatosis pigmentovascularis--case report.
2013; 53: 730-734 [PMID: 24077274 DOI: 10.2176/nmc.cr2012-0241]
37 Oliveira RS, Carvalho AP, Noro F, Melo AS, Monteiro R, Guimar?es R, Landeiro JA. Neurocutaneous melanosis.
2013; 71: 130-131 [PMID: 23392328 DOI: 10.1590/s0004-282x2013000200016]
38 Araújo C, Resende C, Pardal F, Brito C. Giant congenital melanocytic nevi and neurocutaneous melanosis.
2015; 2015: 545603 [PMID: 25722729 DOI: 10.1155/2015/545603]
 World Journal of Clinical Cases2022年15期
World Journal of Clinical Cases2022年15期
- World Journal of Clinical Cases的其它文章
- Diet and intestinal bacterial overgrowth: Is there evidence?
- Spontaneous liver rupture following SARS-CoV-2 infection in late pregnancy: A case report
- Metastasis of liver cancer to the thyroid after surgery: A case report
- Solitary primary pulmonary synovial sarcoma: A case report
- Knot impingement after arthroscopic rotator cuff repair mimicking infection: A case report
- Clear aligner treatment for a four-year-old patient with anterior crossbite and facial asymmetry: A case report