
A novel spherical-headed fascial dilator is feasible for second-stage ultrasound guided percutaneous nephrolithotomy:A pilot study
2021-12-31 01:35:28YiweiWngLihengGoMingxiXuWenfengLiYunshenMoFujunWngLuWngJunZhongWng
Asian Journal of Urology 2021年4期
Yiwei Wng ,Liheng Go ,Mingxi Xu ,Wenfeng Li ,Yunshen Mo ,Fujun Wng ,Lu Wng ,Jun D ,,Zhong Wng ,
a Department of Urology,Ninth People’s Hospital,School of Medicine,Shanghai Jiaotong University,Shanghai,China
b Key Laboratory of Textile Science and Technology,Ministry of Education,College of Textiles,Donghua University,Shanghai,China
KEYWORDS Percutaneous nephrolithotomy;Fascial dilator;Ultrasound guidance;Kidney stones without hydronephrosis
Abstract Objective:In second-stage percutaneous nephrolithotomy(PCNL),because the hydronephrosis has been decompressed,the dilated renal pelvis has resolved and the space is small.Consequently,introduction of the tip of the Amplatz dilator can cause injury to the opposite side of the renal-pelvic mucosa.In this study,we report the experimental and initial clinical performance of a spherical-headed fascial dilator developed specifically for second-stage PCNL.
1.Introduction
Percutaneous nephrolithotomy(PCNL)is the first-line option for patients with large or complex kidney stones and offers the best chance of complete stone clearance with a single procedure.However,a second-stage PCNL is commonly required for several reasons.Derived from an internet-based survey receiving 300 responses from Endourological Society members representing 47 countries,14.3%of urologists preferred a second-stage PCNL to manage≤1 cm stone residual following initial PCNL[1].At many centers,second-look PCNL is routinely undertaken following initial,large stone burden PCNL to assure a complete stone clearance[2,3].Additionally,staged PCNL may be planned or necessitated due to intraoperative circumstances,such as large stone burden,pyonephrosis,or abrupt procedure termination as a consequence of brisk hemorrhage[4,5].
In the above situations,a second-stage PCNL is performed for patients with indwelling nephrostomy tubes,simplifying the technique for the second-stage PCNL.Immediately following removal of the nephrostomy tube,the fascial dilator along with the working sheath can be passed down this established access tract without need for puncture or sequential dilation.Despite these apparent advantages for a second-stage PCNL,the associated complications,according to standard Clavien Scores,have been comparable to the initial PCNL[2].
Because of the feasibility and avoidance of radiation,ultrasound guided PCNL has gained increasing acceptance.This also applies to guidance of renal tract dilation[6].However,in the absence of hydronephrosis,dilation even with ultrasound guidance is associated with risks of hemorrhage and channel loss[7].Over time,an indwelling nephrostomy tube relieves the hydronephrosis,and an attempt to induce artificial hydronephrosis is difficult to establish and maintain due to leakage through nephrostomy channel.Inevitably,therefore,the intrapelvic space in second-stage PCNL is small.In this situation,the introduction of the sharp tip of the Amplatz dilator down the tract is not monitored clearly under ultrasound guidance,and the safety of this approach,therefore,depends on the experienced touch of the urologist.Unfortunately,over-insertion may result in damage to the opposite side of the renal-pelvic mucosa and even perforation.To solve this problem,we developed a spherical-headed fascial dilator specifically for patients who had undergone prior PCNL or nephrostomy.In this study,we report the experimental and initial clinical performance of this novel dilator.
2.Materials and methods
2.1.Design characteristics of dilators
Fig.1 shows three 16 Fr Teflon Amplatz dilators and working sheath.The design characteristics of the dilators are listed in Table 1.D1 and D2 have tapered heads with flat tips.The diameter and taper of D2 are greater than that of D1.D3 is the novel dilator having a spherical head.D1 was manufactured by Urovision,Bad Aibling,Germany.D2 and D3 were manufactured by Ruibang,Zhuzhou,China.

Table1 Morphological features of the dilators.
2.2.In vitro static puncture test
A static puncture test was performed using a universal testing machine(YG[B]026h-500,Darong Textile Instrument Co.,Ltd.,Wenzhou,China).A polyethylene(PE)film and a nitrile butadiene rubber(NBR)film were employed to simulate the human renal pelvis,with a test area set as 0.785 cm(10 mm diameter).Theexperimentaldilatorswereprogrammedtoadvance against the fixedmembranes at a rateof 200 mm/min.All tests were conducted under standard environmental conditions(20±1C,relative humidity[RH]65%±2%),and the test was repeated four times for each dilator.
2.3.Patients
The study enrolled eight patients with 16 Fr indwelling nephrostomy tubes who had undergone first-stage PCNL ornephrostomy,and were scheduled to undergo a secondstage PCNL between June 2019 and October 2019 at Shanghai Ninth People’s Hospital,Shanghai Jiaotong University School of Medicine.There were no specific exclusion criteria.This study was approved by the ethics committee of Ninth People’s Hospital,School of Medicine,Shanghai Jiaotong University(approved number:2016-47-C14)and was therefore performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.Informed consents were obtained from all study participants.
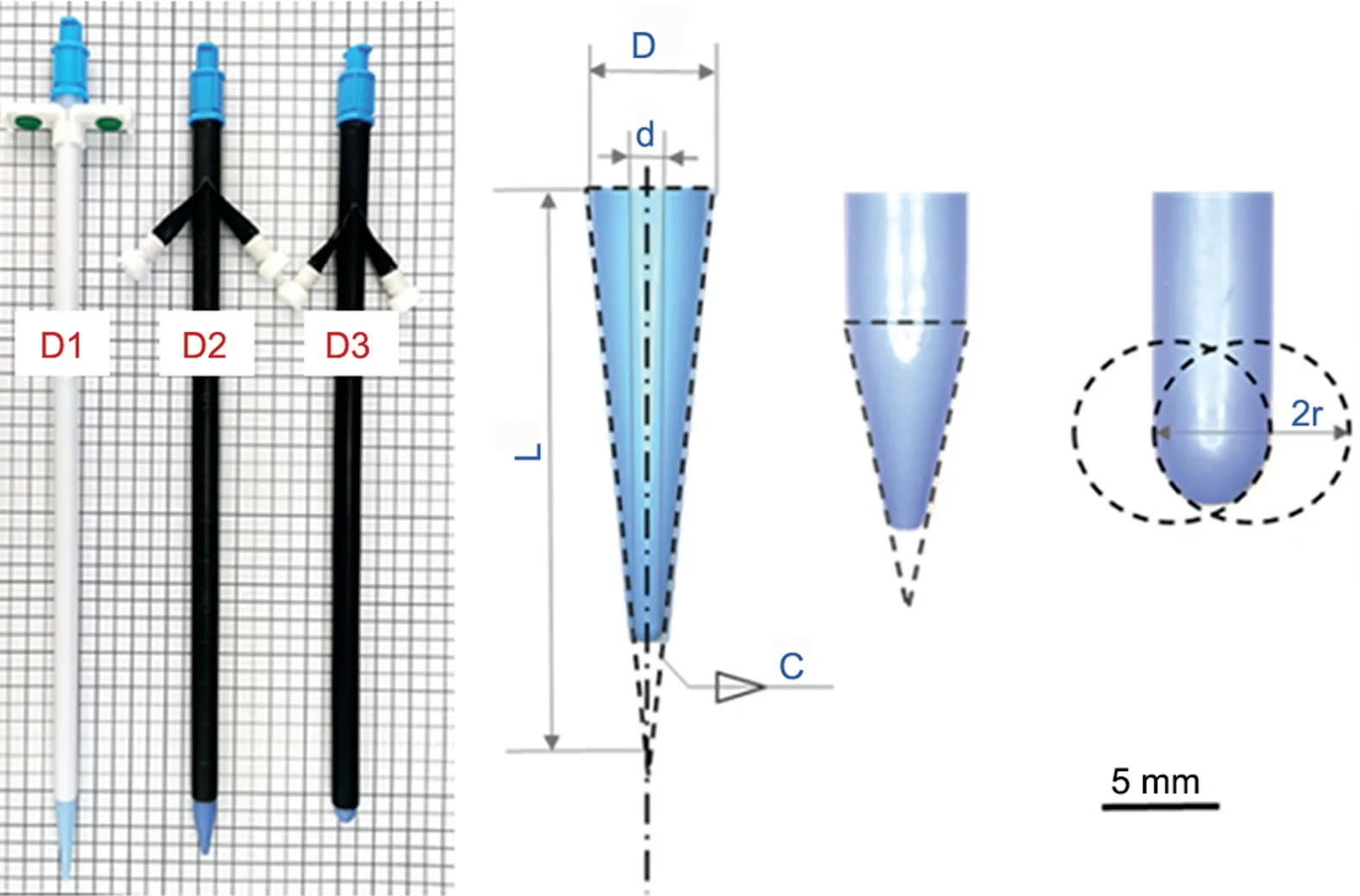
Figure 1 Morphology of dilators.D1 and D2 dilaters have tapered heads with flat tips;D3 dilator has a sphericalhead.D means bulk diameter;d means tip diameter;C means taper;r means radius of curvature;L means cone length.The physical features of stated dilaters are listed in Table 1.
2.4.Surgical procedures
Following induction of general anesthesia,the patients were placed in a prone position,and the 16 Fr nephrostomy tube was gently pulled back until meeting resistance.At that point,the scale mark on the tube was recorded.A 0.035-inch zebra guide wire was inserted through the lumen of the nephrostomy tube into the collecting system.The nephrostomy tube was removed and using ultrasound guidance,the novel spherical-headed fascial dilator along with an 18 Fr working sheath was passed down the access tract into the collecting system guided by the zebra wire.The depth of insertion was guided by the scale mark recorded on the nephrostomy tube.The spherical-headed fascial dilator was then withdrawn from the working sheath,and the planned nephrolithotomy procedure proceeded.A single surgeon performed all surgeries.
2.5.Analysis
Statistical analyses were conducted with R 3.5.1(R Foundation for Statistical Computing,Vienna,Austria).Statistical analysis was performed using one-way ANOVA followed by the LSD test.Statistical significance was determined as p≤0.05.
3.Results
3.1.In vitro static puncture resistance behaviour of dilators
The static puncture results of dilators advanced against the PE and NBR membranes are shown in Fig.2.Typical puncture resistance-displacement curves from three samples are shown in Fig.2A and 2B,with corresponding quantification shown in Fig.2C and 2D.When the dilators were advanced into the same material,they encountered similar initial resistance,as determined by the Young’s modulus of the PE or NBR membranes.In contrast,when D3 was advanced(novel spherical headed dilator),the tested material could withstand higher elongation and demonstrated the highest static puncture resistance,significantly different from D1 and D2(p<0.005).Specifically,when penetrated into PE film,the average maximum resistance of D1 was 4.23 kg?m/sand the average maximum deformation was 3.89 mm;the comparison data of D3 were 11.63 kg?m/sand 12.46 mm,three times that of D1.Similar results were found when tested with the more elastic NBR film.Notably,when D3 was used to pierce the tested materials,since the puncture resistance and displacement were three times that of D1 and D2,more than nine times of puncture energy was costed(Fig.2E),which corresponds to the area under the resistancedisplacement curve.The scenario of a static puncture test is depicted in Fig.2F.
3.2.Patient characteristics and clinical outcomes
The spherical-headed fascial dilator was used for the secondstage PCNL in eight patients.The baseline characteristics including age,gender,and stone characteristics have been summarized in Table 2.The indications for second-stage PCNL were as follows:Two patients had residual stones>1 cm;four patients had planned,two-stage operations due to the initial large stone burden;and two patients had undergone initial nephrostomy placement to relieve pyonephrosis 2 weeks prior to the second-stage PCNL.Urine cultures for all patients were negative.The novel dilators were successfully passed into the collecting system in all cases.No renal pelvic perforation or brisk hemorrhage was identified and no transfusions were necessary.
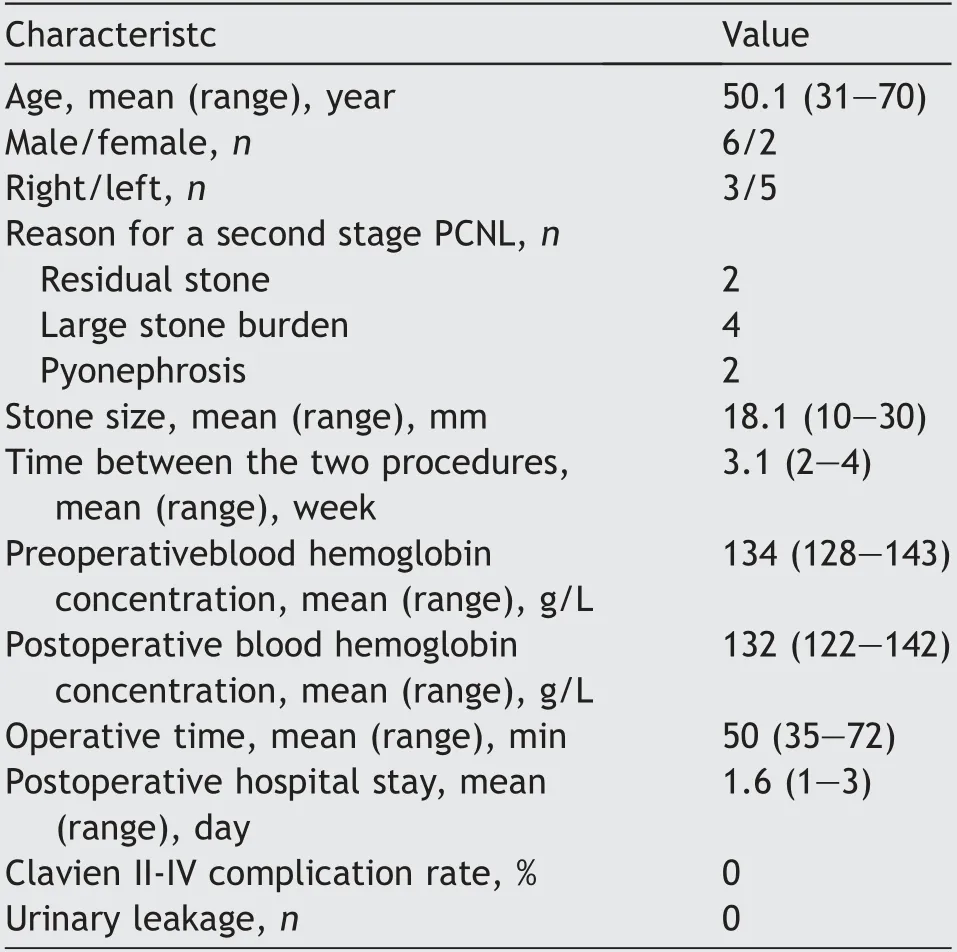
Table 2 Patient characteristics and perioperative findings.
4.Discussion
The classic technique of fluoroscopy guided PCNL is accepted by the majority of urologists worldwide[8].Using fluoroscopy with antegrade pyelography,the dilator can be guided precisely to the correct depth,avoiding injury to the opposite mucosa.A significant disadvantage,however,is the radiation exposure to both patients and doctors[9].Urologists had investigated multiple methods attempting to reduce radiation exposure during PCNL procedures[10].With the feasibility and reliability of ultrasound-guided PCNL having been verified in previous reports,an increasing number of urologists have embraced ultrasound guidance[6].Nevertheless,the most frightening and controversial aspect of ultrasound guided PCNL is the sequential dilation,which relies heavily on urologist experience.In totally ultrasound-guided PCNL,Teflon Amplatz dilators are recommended[11].Because the tips of Amplatz dilators are sharp,one of the most seriouscomplications of using them is penetrating injury of the opposite renal pelvic wall by advancing the dilator too deeply.This injury can occur even under fluoroscopic or ultrasound guidance[10].As evidence of this serious concern,during the same period of this study,we encountered 2(8%)cases of opposite side renal pelvis perforation during dilation procedures in 25 cases of second-stage PCNL using conventional dilators.Even though the novel spherical-headed dilator was designed specifically for second-stage PCNL using ultrasound guidance,it can be utilized equally effectively if fluoroscopic guidance is preferred.
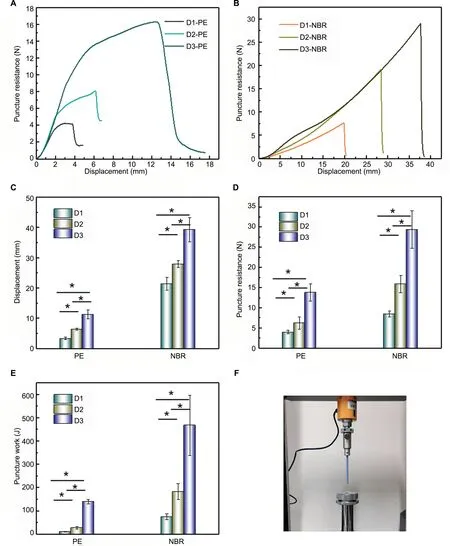
Figure 2 Static puncture resistance-displacement behavior of dilators against PE or NBR film.(A and B)Typical puncture resistance-displacement curve;(C)Displacements of dilators;(D)Puncture resistance of dilators;(E)Puncture work of dilators;(F)Testing method.PE,polyethylene;NBR,nitrile butadiene rubber.
Logically,in cases of kidney stones without hydronephrosis,the space in the collecting system is limited,making dilation even a bigger challenge,with similar associated risks of hemorrhage and channel loss[7].The insertion of the working sheath poses a significant challenge,and because of limitations to all monitoring methods in this circumstance,the experience of the urologist becomes paramount.
In contrast,when an existing tract has been established at the initial stage PCNL or there is a nephrostomy,there are critical elements to achieve a successful second-stage PCNL.When inserting the dilator along with the working sheath,most important is the depth of insertion,thereby avoiding injury to the opposite side of the renal pelvis.Additionally,due to the mobility of the kidney in the retroperitoneum,the tract may shift due to shrinkage of dilated kidney.
Because there is no existing method to simulate the force applied to the dilator by a surgeon during the PCNL surgery,we utilized an in vitro technique to mimic the procedure.Puncture strength tests(static puncture test)are commonly used to determine the puncture or rupture characteristics of a material.It is a compressive test where a material is compressed by a probe or other type of deviceuntil the material ruptures or until an elongation limit is achieved.In the present study,we used static puncture tests for the reverse purpose to test the pressure under which the testing probe,the dilator,could rupture the membrane.From the results,the tapered-headed dilators with smaller tips and sharper edges easily stabbed into the soft membranes,even when the taper was adjusted.The design of the spherical end diffused the pressure by increasing the contact area thereby distributing the pressure.This design enhanced the stab resistance and displacement and reduced the risk of stabbing into soft materials.In the experimental study,we selected PE and NBR to simulate renal pelvis.For each kind of material,when elongation limit was achieved,the puncture resistance force to the novel spherical-headed fascial dilator was 2-3 times higher than the force to a tapered-headed dilator(Fig.2D).These results provided strong support to proceed with the clinical study.
There are limitations to our study.These include the application of static puncture tests to simulate a real surgical procedure,specifically the difference between the test membrane material and the human renal pelvis.We have considered using porcine renal pelvis in future studies.In addition,we could not equate stab force applied to the membrane to the force applied by the surgeon to the dilator.
To our knowledge,our novel spherical-headed fascial dilator was used for the first time to perform a PCNL.Because this was a pilot study,our aim was to investigate the feasibility and initial safety of using a spherical-headed fascial dilator in second-stage PCNL.Due to a small number of patients,it is only possible to make conclusions regarding the feasibility of the method.For safety requires a large population to verify,we are designing a randomized controlled trial in the future to include not only secondstage PCNL,but perhaps to include all ultrasound guided PCNL,with or without associated hydronephrosis.
5.Conclusion
The novel spherical-headed fascial dilator was developed to avoid concentration of the pressure at the tapered,sharp tip of a dilator by increasing the contact area and uniformly distributing and diffusing the pressure.It proved feasible to use in a limited clinical trial for secondstage PCNL.No renal pelvic injury or brisk hemorrhage was observed.
Author contributions
Study concept and design:Yiwei Wang,Lu Wang,Jun Da,Zhong Wang.
Data acquisition:Liheng Gao,Mingxi Xu,Wenfeng Li,Yuanshen Mao.
Data analysis:Yiwei Wang,Liheng Gao,Mingxi Xu.
Drafting of manuscript:Yiwei Wang,Liheng Gao,Mingxi Xu.
Critical revision of the manuscript:Yiwei Wang,Liheng Gao,Fujun Wang.
Conflicts of interest
The authors declare no conflict of interest.
Acknowledgements
This study was funded by grants from Shanghai Sailing Program(19YF1427200),National Natural Science Foundation of China(81902556),Shanghai Municipal Commission of Health and Family Planning Program(20184Y0151),Shanghai Association of Chinese Integrative Medicine Program(ZHYY-ZXYJHZX-1-03),and Shanghai Ninth People’s Hospital Chuangke Projects(CK2018009).All these study sponsors have no roles in the study design,in the collection,analysis,and interpretation of data.
 Asian Journal of Urology2021年4期
Asian Journal of Urology2021年4期
- Asian Journal of Urology的其它文章
- Radical cystoprostatectomy with orthotopic neobladder for a case of treatment emergent neuroendocrine prostate cancer presenting as bladder mass with hematuria-a rare instance of tumor remission after local control
- Late upper urinary tract urothelial carcinoma following radical cystectomy,presenting as page kidney
- Metachronous chest wall metastasis from clear cell renal cell carcinoma-A rarity
- Perioperative anticoagulation and open distal corpora cavernosa shunt in the management of a case of stuttering idiopathic persistent childhood ischaemic priapism
- Effect of tamsulosin versus tamsulosin plus tadalafil on renal calculus clearance after shock wave lithotripsy:An open-labelled,randomised,prospective study
- Impact of COVID-19 on endourology surgical practice in Saudi Arabia:A national multicenter study