
Therapeutic effectiveness of a single exercise session combined with WalkAide functional electrical stimulation in post-stroke patients: a crossover design study
2021-11-11 00:43VivianeRostirolaElsnerLucieliTrevizolIsadoradeLeonMarcosdaSilvaThaynWeissMilenaBragaDanielaPochmannAmandaStolzenbergBlembeelCarolineDaniEleniceBoggio
中國(guó)神經(jīng)再生研究(英文版) 2021年5期
Viviane Rostirola Elsner , Lucieli Trevizol Isadora de Leon Marcos da SilvaThayná Weiss Milena Braga Daniela Pochmann Amanda Stolzenberg BlembeelCaroline Dani Elenice Boggio
Abstract A growing body of evidence has suggested that the imbalance of epigenetic markers and oxidative stress appears to be involved in the pathophysiology and progression of stroke. Thus, strategies that modulate these biomarkers might be considered targets for neuroprotection and novel therapeutic opportunities for these patients. Physical exercise has been reported to induce changes in these epigenetic markers and improve clinical outcomes in different populations. However, little is reported on this in post-stroke patients. The purpose of this study was to investigate the effect of a single exercise session with WalkAide functional electrical stimulation (FES) on cognitive performance,clinical functional parameters, oxidative stress and epigenetic modulation in post-stroke individuals. In this crossover design study, 12 post-stroke individuals aged 54–72 years of either sexes were included and subjected to a single session of exercise (45 minutes) without WalkAide functional electrical stimulation (EXE alone group), followed by another single session of exercise (45 minutes) with WalkAide functional electrical stimulation (EXE + FES group). The clinical functional outcome measures, cognitive performance and blood collections for biomarker measurements were assessed pre- and post-intervention. After intervention, higher Berg Balance Scale scores were obtained in the EXE + FES group than in the EXE alone group. There was no significant difference in the Timed Up and Go test results post-intervention between EXE alone and EXE + FES groups. After intervention, a better cognitive performance was found in both groups compared with before the intervention. After intervention, the Timed Up and Go test scores were higher in the EXE + FES group than in the EXE alone group.In addition, the intervention induced lower levels of lipid peroxidation. After intervention, carbonyl level was lower, superoxide dismutase activity and superoxide dismutase/catalase activity ratio were higher in the EXE + FES group, compared with the EXE group alone. In each group, both histone deacetylase (HDAC2) and histone acetyltransferase activities were increased after intervention compared with before the intervention. These findings suggest that a single exercise session with WalkAide FES is more effective on balance ability and cognitive performance compared with conventional exercise alone in post-stroke patients. This is likely to be related to the regulation of oxidative stress markers. The present study was approved by the Research Ethics Committee of the Methodist University Center-IPA (approval No. 2.423.376)on December 7, 2017 and registered in the Brazilian Registry of Clinical Trials—ReBEC (RBR-9phj2q) on February 11, 2019.
Key Words: cognition; epigenetic; exercise; functional electrical stimulation; functional mobility; oxidative stress; stroke; WalkAide
Introduction
Stroke is one of the most common causes of neurologic morbidity worldwide (Donnan et al., 2008). Irreversible and modifiable risk factors such as sex, ethnicity, age, smoking,excess alcohol consumption, hyperlipidemia, heart disease,diabetes mellitus and sedentary lifestyle have been linked to stroke (Chen et al., 2014; Benjamin et al., 2017). Hemiplegia stands out as the most important clinical outcome present in post-stroke patient, contributing to functional independence(Stewart, 2008). Furthermore, cognitive impairment, including memory loss, is a common symptom that is widely observed to negatively impact the quality of life of survivors (Cullen et al., 2007).
Despite stroke physiopathology being unknown, several research groups have highlighted the pivotal role of epigenetic machinery, including histone acetylation imbalance (Wang et al., 2012; Fessler et al., 2013; George et al.,2013; Gonzalez-Zu?iga et al., 2014; Shen et al., 2014).This epigenetic mechanism is controlled by two enzymes:histone acetyltransferase (HAT) and histone deacetylase(HDAC), which increase and decrease transcriptional activity and gene expression, respectively (Kouzarides, 2007).Decreased levels of histone H3 acetylation in peripheral blood mononuclear cells (PBMCs) from acute cerebral infarction patients compared with healthy controls have been reported.In addition, the use of HDAC inhibitors has been suggested as a promising protective strategy in experimental models of stroke (Wang et al., 2012; Fessler et al., 2013; George et al.,2013).
Accumulative lines of evidence also demonstrate that oxidative stress plays a crucial role in stroke pathophysiology(Basinska et al., 2015; Cetin et al., 2017). Specifically, Tsai et al. (2014) found higher thiobarbituric acid reactive substances (TBARS) levels and lower free thiol level in stroke patients compared with the control group 1 and 7 days after acute ischemic stroke. Moreover, the severity of neurologic damage is inversely correlated with superoxide dismutase(SOD) activity (Spranger et al., 1997; Gariballa et al., 2002).Therefore, strategies that modulate these biomarkers might be considered targets for neuroprotection and novel therapeutic opportunities for these patients.
Importantly, the number of post-stroke patients who need rehabilitation has been rapidly increasing, mainly to improve the function of hemiplegic gait (Coleman et al., 2017). Besides the conventional use of ankle-foot orthosis (AFO), another alternative foot drop option for post-stroke patients includes the functional electrical stimulation (FES) to the common peroneal (fibular) nerve to elicit ankle dorsiflexion during the swing phase of the step cycle. Some research groups have demonstrated better results in clinical functional outcomes when FES is combined with the rehabilitation program in post-stroke patients (Sabut et al., 2011; Sharif et al., 2017),improving gait speed and mobility function (Kottink et al.,2004; Robbins et al., 2006; Morone et al., 2012).
The WalkAide System emerges as a noninvasive new therapeutic tool for foot drop related to brain diseases,presenting some advantages compared with conventional FES, such as a small lightweight battery-powered unitand no adverse effects. Its use appears to decrease foot drop and contributes to normalizing the gait pattern (Sheffler et al.,2006; Cameron, 2010). Morone et al. (2012) found better improvements in the parameters related to walking when post-stroke patients were submitted to WalkAide use (20 sessions, 40 minutes each session, 5times/week) compared with conventional neuromotor rehabilitation with an anklefoot orthosis(AFO). Despite these findings demonstrating the long-term effects, no evidence has shown the impact of a single session of training combined with WalkAide FES in poststroke individuals.
Therefore, this is an important topic to be investigated, since it was reported that single sessions of exercise per se are able to improve skill retention in post-stroke patients, which seems to improve motor recovery in this population (Nepveu et al.,2017). In fact, experimental studies confirmed that these exercise protocols seem to promote neuroplasticity (Mang et al., 2013; Taubert et al., 2015) and are able to reduce the size of the lesion (Middleton et al., 2013). Clinical trials also showed that this exercise modality also improves cognition and motor function (Forrester et al., 2008; Quaney et al., 2009).
It is important to note that the molecular mechanisms associated with the beneficial effects of single rehabilitation sessions with or without the use of FES in post-stroke patients have not yet been fully elucidated. Interestingly, evidence has shown that both single and chronic exercise protocols are able to change oxidative stress and epigenetic parameters in different populations such as obese, schizophrenic and diabetic individuals (Dorneles et al., 2016, 2017; Lavratti et al.,2017; Korb et al., 2018); however, clinical trials involving poststroke patients have been poorly exploited.
Therefore, our hypothesis is that a single session of exercise combined with WalkAide FES improves motor and cognitive outcomes in post-stroke patients through the modulation of epigenetic markers and oxidative stress.
Subjects and Methods
Subjects
Twelve post-ischemic stroke patients of either sex aged 54–72 years were recruited in this study between April and June 2018.Inclusion criteria of the patients were determined as a) having a stroke at least 6months ago; b) having the ability to walk without using a brace and being medically stable (i.e., no history of myocardial infarction). Exclusion criteria were determined as a)having cognitive impairment that causes lack of communication;b) having aphasia; c) having a severe heart disease (e.g., aortic stenosis, angina, hypertrophic cardiomyopathy, arrhythmia, or cardiac pacemaker); d) having uncontrolled diseases (such as hypertension or epilepsy); e) using HDAC inhibitor drugs; f) the presence of other associated neurological diseases, orthopedic and/or musculoskeletal disorders affecting gait; g) deficit of sensitivity in the hemiparetic limb; h) pregnant women and individuals with metal plaques and cancer in the region of the head of the fibula.
The Research Ethics Committee of the Methodist University Center-IPA (approval No. 2.423.376) approved the present study on December 7, 2017 (Additional file 1), and all procedures were performed based on theDeclaration of Helsinki. Written informed consent was given by each participant voluntarily according to Resolution 466/12 of the Brazilian National Health Council (Additional file 2).Furthermore, this study was registered in the Brazilian Registry of Clinical Trials—ReBEC (RBR-9phj2q) on February 11, 2019.
Study design
The current study used a crossover design, where participants were firstly submitted to a single session of exercise without WalkAide FES (exercise group, EXE), followed by another session of exercise with WalkAide FES 7 days later (exercise+ FES group, EXE + FES). All the clinical functional outcome measures and cognitive performance were assessed before intervention and at the end of the intervention. For the biomarker measurements, the individuals were submitted to blood collections before and after the intervention.Interventions and subsequent blood collections were always performed at the same time (2 p.m.–4 p.m.). A blinded observer to the study carried out all analyses. The study design is highlighted in Figure 1.

Figure 1|Study design.
Exercise intervention
The intervention was held in a laboratory at the Methodist University Center-IPA. We used a protocol of exercises based on the study from Modesto and Pinto (2013), which consisted of the following over a period of 45 minutes: 1) Upper and lower limb stretching exercises –10 minutes; 2) active exercise resistance with 1 kg, knee flexion and extension –5 minutes;3) balance and proprioception exercises with walking on mats–5 minutes; 4) dual task motor and cognitive exercises, where the participant should walk on numbered carpets, placing his/her feet according to the number requested by the examiner–10 minutes; and 5) exercises for aerobic conditioning using walking –15 minutes.
WalkAide FES application
The WalkAide foot drop stimulator (Innovative Neurotronics,Austin, TX, USA) was used in the EXE + FES group. The WalkAide foot drop stimulator is characterized as a small(8.2 cm × 6.1 cm × 2.1 cm, 87.9 g) device that delivers asymmetrical biphasic surface electrical stimulation, pulse width 25–300 ms and maximal stimulation period for 3 seconds. The device was initially manually synchronized with each individual walking pattern, within the parameters described above. The intensity (mA) was sufficient to cause the movements of dorsiflexion and eversion, which was tolerable for the participant, and was adjusted using a dial on the device. Dorsiflexion was achieved by common fibular/peroneal nerve stimulation with one electrode at the head of fibula and the other on the main muscle belly of the tibialis anterior.
Clinical functional parameters
Balance abilities and fall risks
The Berg Balance Scale (BBS) (Alonso et al., 2014) was used to evaluate the balance and risk of falls. This instrument is composed of 14 tests measuring the ability to sit, stand, spin around, look over the shoulders, and stand over one-way support and transport steps. The highest score is 56 points,scores < 45 indicate a low to moderate risk of falls, while scores < 36 are associated with a 100% risk of falls.
Functional mobility
Functional mobility was tested by the Timed Up and Go(TUG) test (Podsiadlo and Richardson, 1991; Wennie Huang et al., 2010; Viccaro et al., 2011). In this test, individuals were required to start from a sitting position, get up from a standard chair, walk 3 meters, turn around, return to the chair, and sit again. Periods > 20 seconds to perform the test suggest an increased risk for falls and functional dependence.
Cognitive performance
The Montreal Cognitive Assessment (MoCA) was used to evaluate cognitive performance (Julayanont et al., 2015). This assessment allows the detection of cognitive impairment by assessing various domains of cognition, including attention,executive function, memory, language, visuospatial skills,conceptualization, calculation, and orientation. The highest score is 30, and total values < 26 points are linked to cognitive impairment.
Blood sampling
Venous blood samples (15 mL) were taken from the antecubital vein using sterile vacutainer tubes (Becton-Dickinson, Oxford, UK) before and immediately after experimental exercise sessions. The peripheral blood was used to acquire the PBMCs for epigenetic analysis and plasma for oxidative stress marker measurements. The samples were aliquoted and frozen at –20°C.
PBMC isolation and histone acetylation status analysis
The PBMCs were isolated from EDTA blood according to the technique of Bicalho et al. (1981). HDAC2 and HAT activities were measured using colorimetric assay kits according to the manufacturer’s protocol (Epigentek, Madrid, Spain: P-4006:EpiQuik HDAC2 assay kit; P-4003: EpiQuik HAT activity/inhibition assay kit, respectively).The Coomassie Blue method(Bradford, 1976) taking bovine serum albumin as standard was used to determine HDAC2 and HAT activities.
Parameters of oxidative stress
Thiobarbituric acid (TBA) reactive substances
To evaluate the lipid peroxidation, we used TBARS production,as previously described by Wills (1966). This reaction is an acid-heating reaction, where the samples were mixed with 10% trichloroacetic acid (TCA) and 0.67% TBA, and the levels were determined by absorbance at 535 nm. Results were expressed as nmol/mg protein.
Measurement of oxidation modified protein levels
To evaluate the protein oxidation damage, we determined the carbonyl groups on the basis of their reaction with dinitrophenylhydrazine (DNPH; Levine et al. 1990). DNPH reacts with protein carbonyls to form hydrazones, which can be measured spectrophotometrically (Levine et al. 1990). The absorbance was read at 370 nm. The results were expressed in nmol/mg protein.
Measurement of total sulfhydryl content
The total sulfhydryl (SH) assay is to reduce 5,5′-dithio-bis(2-nitrobenzoic acid) (DTNB) content by thiols and measure spectrophotometrically at 412 nm. The SH content is inversely correlated to protein oxidative damage. Results were reported in nmol/mg protein (Aksenov and Markesbery, 2001).
Measurement of antioxidant enzyme activity
Superoxide dismutase (SOD) activity was measured according to the inhibition of adrenochrome formation at 480 nm(Spectrophotometer SP-2200, Bioespectro, Curitiba, PR,Brazil). The results were expressed in USOD/mg protein(Bannister and Calabrese, 1987). Catalase (CAT) activity was previously described by Aebi (1984) and it determined the rate of H2O2degradation at 240 nm (Spectrophotometer SP-2200) (Aebi, 1984).The results were expressed as UCAT/μg protein. The relation of these two enzymes was calculated by the activity ratio. SOD and CAT activities was determined according to the method described by Lowry et al. (1951).
Statistical analysis
The Shapiro-Wilk test was used to test the normality of variables. The pairedt-test was used for pre-and postintervention comparisons. The Sidakpost hoctest with generalized estimation equation was used to compare between pre- and post-intervention and between groups. All statistical analyses were performed using SPSS 20.0 software(IBM, Armonk, NY, USA) and a level ofP-value < 0.05 was considered statistically significant.
Results
Participant characteristics
The current study included 12 individuals. No participant withdrew from the intervention, and all performed the tests that evaluated clinical functional outcomes. However,the analysis of biomarkers was performed in only six volunteers because of difficulty in blood collection (n= 3) or disagreement of blood collection (n= 3). The baseline of the 12 patients is shown in Table 1.
In other variants, the eldest daughter is covered with tar27 or pitch that cannot be removed, given a box of serpents, riddled64 with leprosy, or cursed with eternal ugliness.Return to place in story.
Clinical functional outcomes
A higher score in the BBS after intervention was observed only in the EXE + FES group (Figure 2A;P= 0.002). Furthermore,there were no significant differences in TUG test results between groups and between pre- and post-intervention(Figure 2B;P> 0.05).
As described in Figure 3, after intervention, better cognitive performance was found in both groups compared with prior to intervention (Figure 3;P= 0.000). Importantly, after intervention, high MoCA scores were obtained in the EXE +FES group than in the EXE group (Figure 3;P= 0.05).
Oxidative stress parameters
When analyzing oxidative stress parameters, especially lipid peroxidation (TBARS) and considering the time factor, we found the values were significantly lower after intervention(0.85 ± 0.14;P= 0.002) compared with before the intervention. When considering only the equipment factor effect, we found the values were significantly lower in the EXE+ FES group than in the EXE alone group (0.45 ± 0.06vs. 0.80± 0.08;P= 0.001). When we analyzed both factors (time and equipment), there were significant differences in the values of oxidative stress parameters before and after the intervention in the EXE alone group (P= 0.003; Figure 4A).
The effect of the isolated factors was not observed during the carbonyl assay; however, an interaction between the factors was found, with a significant reduction in this damage in the EXE + FES group after the intervention compared with before the intervention (Figure 4B;P< 0.05). Considering the nonenzymatic antioxidant defense, there was slight, but not significant difference in the SH level between before and after the intervention (Figure 4C).
When the enzymatic antioxidant activities were analyzed,an interaction of the factors time and equipment use in SOD activity was found, and a significant difference in SOD activity existed between before and after the intervention in the EXE +FES group (Figure 5A;P< 0.05). No differences in CAT activity were observed between the groups no matter before or after the intervention (Figure 5B;P> 0.05). The activity ratio of antioxidant enzymes SOD/CAT was significantly lower in the EXE + FES group than in the EXE alone group (1.61 ± 0.25vs.3.02 ± 0.66;P= 0.013; Figure 5C), suggesting that FES alters the activity ratio of antioxidant enzymes SOD/CAT. Finally, a significant increase in HDAC2 activity was observed after the intervention compared with before the intervention (P= 0.017;Figure 6A) in both groups. The same was observed in the HAT activity, where higher activity was found after the intervention(P= 0.05; Figure 6B). No differences were observed when both factors were considered (P> 0.05; Figure 6).
Discussion
Prolonged FES use has been reported to induce therapeutic effects through physiological changes, such as improvements in muscle strength and volitional control (Burridge et al.,1998; Robbins et al., 2006; Everaert et al., 2013). A previous study showed that conventional rehabilitation combined with FES produced better results in functional outcomes, such as spasticity, dorsiflexor strength and motor recovery, when compared to a single conventional intervention (Sabut et al.,2011), although the knowledge concerning the short-term effects and the molecular mechanisms of this intervention is scarce.
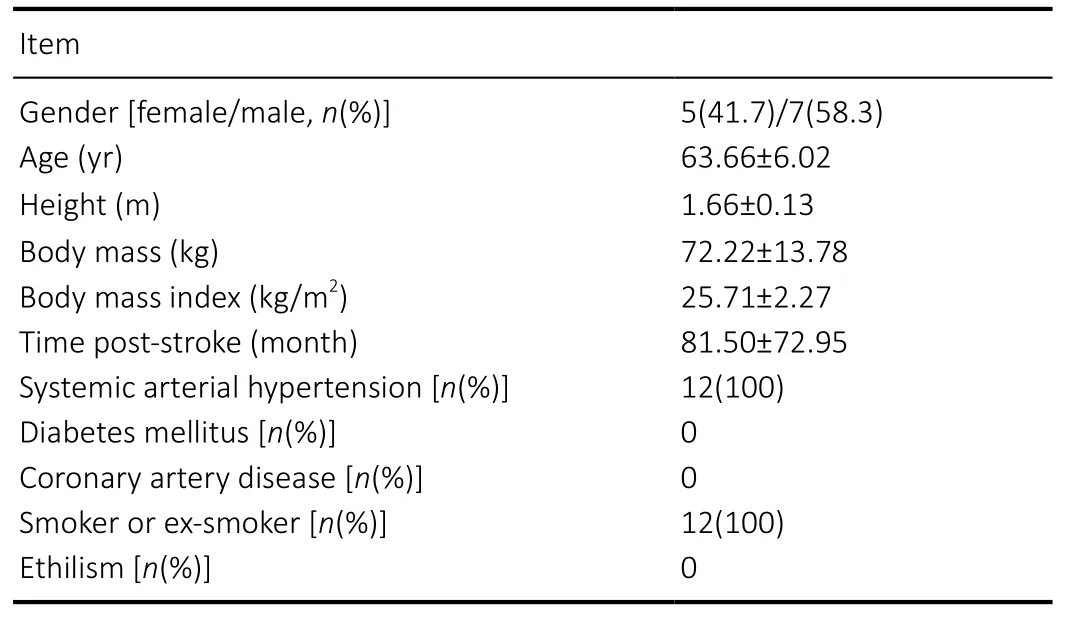
Table 1 |Baseline of the included patients
To date, this is the first evidence demonstrating the impact of a single exercise session associated with the WalkAide FES on clinical functional parameters, cognitive performance,oxidative stress markers and epigenetic modulation in poststroke individuals. We found better outcomes regarding balance ability and cognitive performance in the EXE +FES group compared with the EXE alone group, and the modulation of oxidative stress parameters seems to be related, at least in part, to these beneficial effects.
Clinical functional outcomes
In stroke patients, the standing skill is crucial to gait performance and plays an important role in enabling patients to conduct their daily activities independently. The balance ability, evaluated through the BBS in the current study, was significantly improved in the EXE + FES group, while no significant changes in this variable were observed in the EXE alone group after the intervention. Our data are related to other studies that verified the chronic effects of combined therapy exercises with FES on balance in stroke patients(Dujovi? et al., 2017; Lee et al., 2019). Lee et al. (2019)recently showed that patients who underwent conventional rehabilitation with FES (30 sessions, 5 days a week for 3 weeks) had higher BBB scores than controls. FES therapy combined with conventional rehabilitation (60 minutes each session, 5 days a week for 4 weeks) was reported to be more effective on BBB performance than a single conventional rehabilitation program (Dujovi? et al., 2017). Taken together,these findings suggest the effectiveness of the combined use of FES with therapeutic exercises on the balance in post-stroke patients.
It is widely reported that a single exercise session can ameliorate the cognitive performance in both healthy and patient individuals (Schuch et al., 2015; Moriya et al., 2016).Specifically in post-stroke patients, Moriya et al. (2016)showed that a single session of moderate-intensity aerobic exercise with a cycling ergometer for 15 minutes was able to improve the behavioral performance of the working memory task compared with the control condition and also enhances prefrontal cortex activity. In agreement, we found better cognitive performance after the intervention in both groups, which could be explained, at least in part, to the idea that exercise is able to induce neuroplastic changes that facilitate the consolidation of procedural memories (Taubert et al., 2015; Ostadan et al., 2016). Importantly, it should be noted that the EXE + FES group showed higher scores in the MoCA when compared to the EXE alone group. A possible explanation for this result can be related to the knowledge that the use of a foot drop stimulator may strengthen the residual corticospinal connections that remain after a stroke and therefore improve cognitive abilities (Everaert et al.,2013).

Figure 2|The impact of a single exercise session with FES (Exercise + FES group) or without FES (Exercise group) on clinical functional parameters in post-stroke patients.
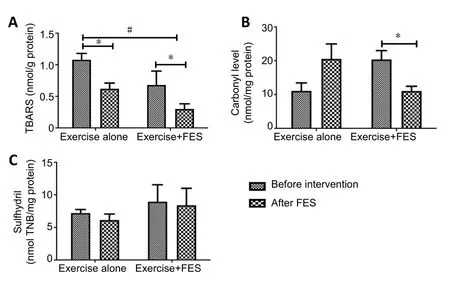
Figure 4|The impact of a single exercise session with FES (Exercise +FES group) or without FES (Exercise alone group) on (A) lipid peroxidation(TBARS), (B) protein oxidation (carbonyl levels) and (C) non-enzimatic content (sulfhydril levels) in post-stroke patients.
In our study, systemic arterial hypertension was present in 100% of the sample. Our data can be partially related to the findings obtained by Elamy et al. (2020) that 81% of post-stroke patients show comorbidities, such as systemic arterial hypertension. The high prevalence of post-stroke comorbidities seems to negatively influence functional outcomes, as stated by Jiang et al. (2020). The authors demonstrated a significant association between increased multiple chronic conditions and worse functional outcomes in post-stroke subjects. Importantly, smoking is still one of the most important risk factors for stroke (Markidan et al., 2018)and also exerts a pivotal role in the disease pathogenesis(Kwan et al., 2013). In fact, all the participants in the current study were smokers or ex-smokers, supporting the extensive literature demonstrating the relationship between stroke and smoking. In this sense, it should be noted that persistent smoking following stroke is associated with poor outcomes and could also contribute to the occurrence of secondary stroke and increased mortality risk (McCarthy et al., 2013).Taken together, these findings could be associated with a compromised performance of the functional clinical data of the participants evaluated in the current study, which were improved after the proposed interventions, demonstrating the effectiveness of exercise and FES use in post-stroke patients.
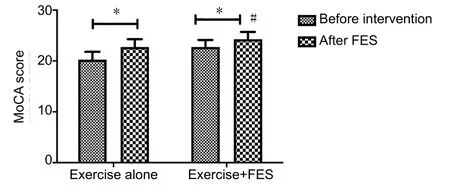
Figure 3|The impact of a single exercise session with FES (Exercise + FES group) or without FES (Exercise alone group) on cognitive performance in post-stroke patients.
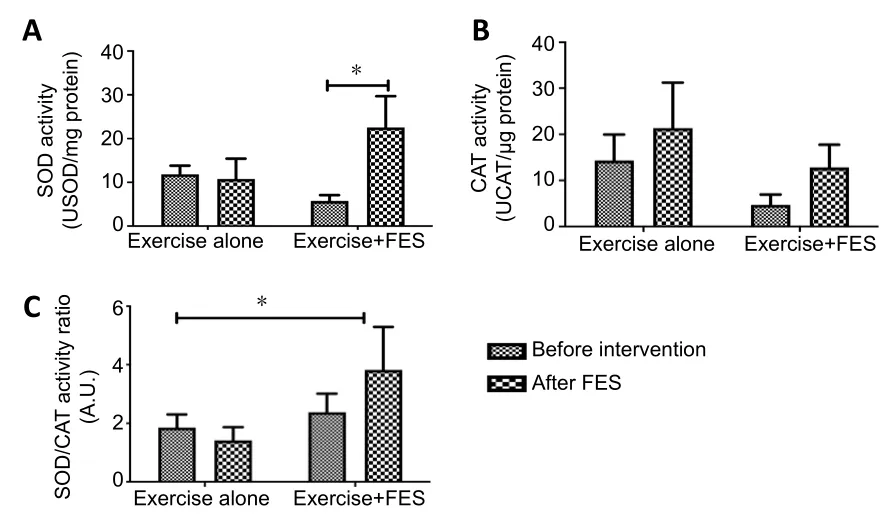
Figure 5|The impact of a single exercise session with FES (Exercise +FES group) or without FES (Exercise alone group) on SOD activity (A), CAT activity (B) and SOD/CAT activity ratio (C) in post-stroke patients.
Oxidative stress parameters
The role of oxidative stress in the pathological mechanism of stroke is well documented (Nayak et al., 2017), since free radicals have been observed in both ischemic and hemorrhagic stroke. In fact, oxidative stress has been found to be one of the mechanisms responsible for tissue damage in these conditions (Hayman et al., 2017; Nayak et al., 2017). In the present study, the lipid peroxidation levels (TBARS) were low considering the time and the FES effects. The same was observed in protein oxidation levels (carbonyl), where FES also reduced its levels. Regarding carbonyl levels, we observed a significant interaction between FES and time only in the EXE+ FES group, as a significant reduction in this parameter was found.
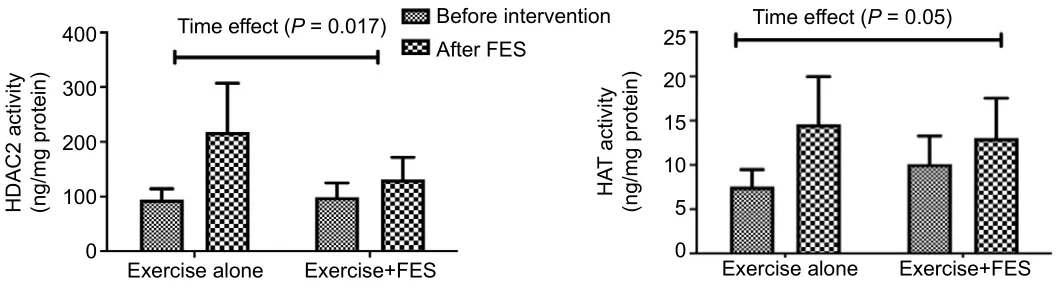
Figure 6|The impact of a single exercise session with FES (Exercise + FES group) or without FES (Exercise alone group) on epigenetic modulation in post-stroke patients.
These results are in accordance with the literature reported by Cichoń et al. (2018) that recently showed all oxidative stress markers were significantly decreased during extremely low frequency and variable pulse shape electromagnetic field therapy when compared with a control group rehabilitated only with aerobic exercises (Cichoń et al., 2018). Moreover,these authors found that extremely low frequency and variable pulse shape electromagnetic field therapy improved the psychophysical abilities of post-stroke patients assessed on various clinical scales, such as Activity of Daily Living, the Geriatric Depression Scale and Mini-Mental State Examination,which evaluate cognitive function (Cichoń et al., 2018).Interestingly, we also demonstrated cognitive improvement in the EXE + FES group compared to the EXE alone group,suggesting that the modulation of oxidative stress markers might be related, at least in part, to the molecular mechanism involved in the beneficial effects of FES use.
It has been reported that stroke could induce an increase in ROS production and also decreased antioxidant enzyme activity by inhibiting inactivation of ROS (Broughton et al.,2009). In fact, ROS are directly involved in oxidative injury to cellular macromolecules, such as proteins, lipids, and nucleic acids, in ischemic tissues, leading to cell death (Cichoń et al., 2015). Regarding the antioxidant defense, we observed that SOD activity and the SOD/CAT ratio was reduced in the EXE + FES group after the intervention. On the other hand,Cichoń et al. (2018) showed that the potential antioxidant mechanism in extremely low frequency and variable pulse shape electromagnetic field therapy was associated with a rise in the activity of the antioxidant enzyme, since this intervention increased SOD and CAT activities and improved the effectiveness of post-stroke rehabilitation.
The importance of CAT activity in ischemic stroke was confirmed by studies performed by Zhang et al. (2017).These authors observed that the supply of CAT to cerebral neurocytes and ischemic subregions in a mouse model of middle cerebral arterial occlusion was significantly enhanced,decreasing the infarct volume (Zhang et al., 2017). In our study, no differences in CAT activity were observed after the intervention in both groups. Contrarily, Cichoń et al. (2018)demonstrated increased levels of CAT mRNA expression after 10 sessions of extremely low frequency and variable pulse shape electromagnetic field therapy compared with the control group. Altogether, these findings suggest that a single exercise session is not able to modulate these oxidative stress parameters. Therefore, we might infer that prolonged interventions are necessary to alter these biomarkers in poststroke patients.
Epigenetic markers
A remarkable point to discuss is the impact of the intervention on epigenetic markers. We observed a remarkable increase in HDAC2 and HAT activities in the EXE and EXE + FES groups after the intervention, suggesting that exercise per se, with or without FES, is able to change these markers. Our results are in accordance with evidence showing that single session of different exercise protocols are able to modulate the histone acetylation status in different populations, such as obese individuals (Dorneles et al., 2016), diabetes (Korb et al., 2018)and cancer patients (Zimmer et al., 2014).
As previously described by Elsner et al. (2011), HAT and HDAC activities regulate chromatin status and gene transcription.Altogether, these findings led us to hypothesize that exercise may acutely regulate the expression of specific genes related to various clinical conditions, including post-stroke patients,which might influence its progression. Future studies may be carried out to elucidate which specific genes can be modulated in response to this intervention.
Interestingly, during physiological conditions, the balance of HAT/HDAC is rigorously maintained and precise epigenetic regulation may be critical for neuronal homeostasis(Fahrner and Bjornsson, 2014). On the other hand, HAT/HDAC discrepancy is linked to neuronal dysfunction and degeneration (Saha and Pahan, 2006). In this sense,the imbalance of histone acetylation status has been demonstrated in both experimental models (Wang et al.2012; Fessler et al., 2013; George et al., 2013) and clinical trials regarding stroke (Shen et al., 2014). As described above,we found a significant increase in HAT and HDAC2 activities after the intervention. Considering that these enzymes have opposing functions on gene transcription, we suggest that acute exercise interventions, with or without FES, are effective in maintaining transcriptional machinery homeostasis in poststroke patients.
Notably, the present study should consider its limitations,including the reduced sample size. However, we believe that these preliminarily findings could encourage future investigations with a larger sample in order to elucidate the impact of a single exercise session combined with WalkAide FES on functional clinical outcomes, as well as the molecular mechanisms associated with that response. In addition, the study population included patients who had had a stroke for at least 6 months. It would be interesting for other studies to evaluate these responses in patients in more acute stages in order to draw a temporal profile demonstrating the shortand long-term effects of the intervention on the analyzed variables.
Conclusion
The current study demonstrated for the first time the therapeutic effectiveness of a single exercise session combined with or without WalkAide FES on clinical functional parameters and cognitive performance in post-stroke individuals. Importantly, our findings suggest that WalkAide FES combined with conventional rehabilitation might be more effective on balance ability and cognitive performance compared with a single conventional rehabilitation program.The modulation of oxidative stress might be an important molecular mechanism underlying these beneficial effects.
Acknowledgments:The authors would like to thank the physiotherapist Bruno Grigol for the technical support with the WalkAide foot drop stimulator.
Author contributions:VRE and EB contributed to definition of intellectual content, literature search, study design, data analysis and manuscript preparation. LT, IDL, MDS, TW, and MB contributed to the intervention,data acquisition/analysis and manuscript review. CD contributed to blood collection, data acquisition, statistical analysis and manuscript editing and review. DP and ASB participated in biomarker measurements and manuscript review. All authors approved the final version of this paper for publication.
Conflicts of interest:None declared.
Financial support:This work was supported by Funda??o de Amparo à Pesquisa do Estado do Rio Grande do Sul (FAPERGS)/BrazilandConselhoNacional de DesenvolvimentoCientífico e Tecnológico –CNPq/Brazil.
Institutional review board statement:The study was approved by the Research Ethics Committee of the Methodist University Center-IPA(approval No. 2.423.376) on December 7, 2017.
Declaration of patient consent:The authors certify that they have obtained all appropriate patient consent forms. In the form the patients have given their consent for their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity.
Reporting statement:This study followed the Transparent Reporting of Evaluations with Nonrandomized Designs (TREND) statement.
Biostatistics statement:The statistical methods of this study were reviewed by the biostatistician of Centro UniversitárioMetodista IPA in Brasil.
Copyright license agreement:The Copyright License Agreement has been signed by all authors before publication.
Data sharing statement:Individual participant data that underlie the results reported in this article, after the identification (text, tables,figures, and appendices) and Informed Consent Form will be available immediately following publication ending 5 years following article publication for researchers who provide a methodologically sound proposal and investigations whose proposed use of the data has been approved by an independent review committee (“l(fā)earned intermediary”)identified for this purpose.
Plagiarism check:Checked twice by iThenticate.
Peer review:Externally peer reviewed.
Open access statement:This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix,tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
Additional files:
Additional file 1:Ethical Approval Documentation (Portuguese).
Additional file 2:Model consent form (Portuguese).
 中國(guó)神經(jīng)再生研究(英文版)2021年5期
中國(guó)神經(jīng)再生研究(英文版)2021年5期
- 中國(guó)神經(jīng)再生研究(英文版)的其它文章
- Enriched environment boosts the post-stroke recovery of neurological function by promoting autophagy
- Surgical intervention combined with weight-bearing walking training improves neurological recoveries in 320 patients with clinically complete spinal cord injury:a prospective self-controlled study
- Recognition of moyamoya disease and its hemorrhagic risk using deep learning algorithms: sourced from retrospective studies
- D-serine reduces memory impairment and neuronal damage induced by chronic lead exposure
- An integrative multivariate approach for predicting functional recovery using magnetic resonance imaging parameters in a translational pig ischemic stroke model
- AAV8 transduction capacity is reduced by prior exposure to endosome-like pH conditions