
Meta-analysis of Therapeutic Efficacy of Purgation and Catharsis Method for Treating Severe Pneumonia
2021-07-21 06:09YaonanDUHongweiTANGCaixiaSHANZhongxinPUShihongXU
Medicinal Plant 2021年3期
Yaonan DU, Hongwei TANG, Caixia SHAN, Zhongxin PU, Shihong XU*
1. Department of Internal Medicine No.1, Affiliated Nanchong Chinese Medicine Hospital of North Sichuan Medical College, Nanchong 637000, China; 2. Department of Critical Care Medicine, Affiliated Nanchong Chinese Medicine Hospital of North Sichuan Medical College, Nanchong 637000, China
Abstract [Objectives] To make a systematic evaluation on the therapeutic efficacy of purgation and catharsis method combined with western medicine in treatment of severe pneumonia. [Methods] The literatures were retrieved from China Knowledge Infrastructure (CNKI), Chinese science and technology journal full-text database (VIP database, VIP), Wanfang Data, the Chinese biomedical database, PubMed, Embase, and the Cochrane Library. The retrieval time was set to the period from the creation of the database to June 2020. The randomized controlled trial (RCT) was conducted on the comparison between the purgation and catharsis method combined with western medicine and the western medicine alone in the treatment of severe pneumonia. The literature information was extracted and the methodological quality of the included literature was evaluated according to the bias risk assessment tool developed by the Cochrane Collaboration. Meta-analysis was performed with the aid of RevMan 5.3 software for the patient response rate, acute physiology and chronic health evaluations II (APACHE II), clinical pulmonary infection score (CPIS), oxygenation index (OI), procalcitonin (PCT), mechanical ventilation time, etc. [Results] A total of 20 articles were included, involving a total of 1 661 patients, and the literature quality was low. Meta analysis results showed that compared with the treatment by western medicine alone, the purgation and catharsis method combined with western medicine can further improve the response rate [RR=1.21, 95% CI (1.14,1.27), P<0.000 01], and reduce the APACHE II score [WMD=-5.92,95% CI(-7.94, -3.89), P<0.000 01], reduce CPIS score [WMD=-1.41, 95% CI (-1.70, -1.12), P<0.000 01], increase oxygenation index [WMD=39.52, 95% CI (29.39, 49.65), P<0.000 01], reduce PCT level [WMD=-2.85, 95% CI (-3.68, -2.01), P<0.000 01], shorten the mechanical ventilation time [WMD=-13.00, 95% CI (-16.51, -9.48), P<0.000 01]. [Conclusions] Within the scope of the study included, the purgation and catharsis method combined with western medicine in the treatment of severe pneumonia can further reduce the pulmonary infection, reduce PCT levels, increase oxygenation index, and improve vital organ functions, thereby improving clinical efficacy, shortening the mechanical ventilation time (MVT), and reducing the economic burden of patients.
Key words Purgation and catharsis method, Severe pneumonia, Meta-analysis
1 Introduction
Severe pneumonia (SP) is a pneumonia with aggravated inflammation of lung tissues (bronchioles, alveoli, interstitial). It is mainly characterized by dyspnea, pulmonary rales, high fever and consciousness disorder, causing organ dysfunction or even endangering life[1]. Community-acquired pneumonia (CAP), hospital-acquired pneumonia (HAP), healthcare-associated pneumonia (HCAP), and ventilator-associated pneumonia (VAP) can cause severe pneumonia. Severe pneumonia has the characteristics of rapid progress, many complications, and high mortality, and it can cause serious complications[2-3]. Epidemiological surveys show that the mortality rate of severe community-acquired pneumonia (SCAP) is 50%, and the mortality rate of severe hospital-acquired pneumonia (SHAP) is up to 70%[4-5]. The treatment of severe pneumonia has mainly antibacterial drugs, oxygen therapy, mechanical ventilation, glucocorticoids, symptomatic support,etc., but the effects of routine treatment are not ideal[6-7]. Severe pneumonia is mainly characterized by high fever, shortness of breath and delirium, and belongs to the category of "dyspnea syndrome", "pulmonary fever" or "wind-warm lung-heat syndrome" in Chinese medicine. According to the theory of traditional Chinese medicine, the lungs and the large intestine are exterior and interior, and high lung heat can be passed down the intestines, leading to intestinal conduction failure, and the obstruction of the intestines can also lead to the failure of lung qi, and the ascending counterflow of lung qi will aggravate dyspnea, yang brightness and interior heat will aggravate the heat situation, the two are closely related with each other. In the course of the occurrence and development of severe pneumonia, they can be mutually cause and effect, so both need to be considered in treatment. At present, there are many randomized controlled trials (RCT) reports on the treatment of severe pneumonia with purgation and catharsis Chinese medicine prescriptions. Studies have found that the purgation and catharsis method can further improve the clinical symptoms of severe pneumonia, reduce inflammation, reduce mortality, and improve clinical efficacy on the basis of conventional treatment. However, there is a lack of large-scale clinical studies and existing literature on research methods, and there are differences in the level of evidence-based medicine, and the level of evidence is insufficient[8-10]. Based on RCT, we conducted a meta-analysis, and systematically evaluated the efficacy and safety of purgation and catharsis method in the treatment of severe pneumonia, to provide evidence-based medical evidence for clinical application.
2 Data and methods
2.1 Literature inclusion criteria(i) Research type: RCT. (ii) Research objects: adult non-viral pneumonia patients who meet the diagnostic criteria for severe pneumonia; for the diagnostic criteria for severe pneumonia, we referred to the diagnostic criteria for severe pneumonia established in 2007 by the Infectious Diseases Society of America/American Thoracic Society (IDSA/ATS)[11]. (iii) Interventions: western medicine standardized treatment, including antibiotics, oxygen therapy, mechanical ventilation, combined medication: patients with chronic obstructive pulmonary disease, coronary atherosclerotic heart disease, hypertension, diabetes and other diseases should take medicines according to relevant guidelines. The treatment group was added with traditional Chinese medicine preparations (including Chinese medicine decoctions and granules) with main function of purging and catharsis by oral, nasogastric gavage, or perfusion method. Different Chinese medicinal preparations belonging to the same treatment method (purgation and catharsis) can be used in combination at the same time, and the control group adopted the western medicine standardized treatment. (iv) Evaluation indicators[1]: primary indicators include the response rate, and the secondary indicators include acute physiology and chronic health evaluations II (APACHE II), clinical pulmonary infection score (CPIS), oxygenation index (OI), procalcitonin (PCT), and adverse reactions.
2.2 Research literature exclusion criteria(i) NCTs, and literature with not accurate randomized methods or unreasonable analysis of experimental data. (ii) Animal experiments, case reports, expert reviews, reviews, animal experiments,etc.(iii) Repeatedly published literature.(iv) Literature without clear diagnostic criteria or efficacy evaluation criteria, or the diagnostic criteria or efficacy evaluation criteria used in the literature not conforming to the inclusion criteria. (v) Studies that do not have complete efficacy data. (vi) Clinical studies using treatment groups combined with other western medicines, or using traditional Chinese drugs without functions of purgation and catharsis, or combined with other treatment methods (such as psychotherapy, exercise rehabilitation, acupuncture, cupping, moxibustion, manipulation or massage,etc.) to compare with conventional western medicine treatment. (vii) Studies comparing with other western medicines and traditional Chinese medicines, or the control group did not use the western medicine standardized treatment for severe pneumonia.
2.3 Search strategies and methods(i) Search scope: literatures were retrieved from China Knowledge Infrastructure (CNKI), Chinese science and technology journal full-text database (VIP database, VIP), Wanfang Data, the Chinese biomedical Database, PubMed, Embase, and the Cochrane Library. (ii) The retrieval time was set to the period from the creation of the database to June, 2020. (iii) Literature language: Chinese and English. (iv) Search words include severe pneumonia, purge, catharsis, diarrhea, Tongfu, Gongxia, Xiafa, Dahuang,Rheumofficinale, rhubarb, and Chengqi Decoction (both in Chinese and English).
2.4 Literature screening and extractionFirst, two researchers independently searched the literature, read the titles and abstracts, and excluded the unrelated literature (giving reasons for exclusion). Then, they searched the full texts and screened those studies conforming to the inclusion criteria, and read to determine whether they conformed to the inclusion criteria. In case of disagreement, and the analysis and discussion failed to reach consistent conclusion, a third party should be invited to make the final decision. When the literature information extraction table was prepared and the relevant information the literature was incomplete or unclear, necessary information could be reasonably inferred from the literature. If it could not be inferred, the literature that cannot obtain the necessary information should be excluded. The literature information was input independently by two researchers and cross-checked jointly. The extracted content included (i) basic information of the literature: first author, year of publication; (ii) basic characteristics of original research: sample size, gender, age, intervention measures (name of medication, dose, course of treatment), and outcome indicators; (iii) outcome indicators: response rate, APACHE II score, CPIS, OI, PCT, and adverse reactions (Table 1).
2.5 Methodological quality evaluation of the included literatureThe quality of the included literature was evaluated in accordance with the bias risk assessment tool developed by the Cochrane Collaboration. The evaluation included random allocation method, allocation scheme concealment, blinded method, data integrity, selective reporting research results, and other sources of bias. The two researchers independently made judgment of "yes" (low bias), "no" (high bias), and "unclear" on the above 6 items. If the judgment results were inconsistent, and the discussion failed to reach an agreement, a third party would be invited to make the final decision. If the information was incomplete, the literature author would be contacted.
2.6 Statistical methodMeta-analysis was carried out with the aid of RevMan 5.3 software. The relative risk (RR) was used as the effect scale for the counts of the response rate. The weighted mean difference (WMD) was used as the measurement data for APACHE II, CPIS, OI, PCT, and MVT. The degree of effect was expressed with 95% confidence interval (CI). For the heterogeneity test,χ2test was performed. If the heterogeneity measurement resultP>0.1 orI2≤50%, it indicates that there was no heterogeneity between several studies, which was tested by the fixed effect model; if there is heterogeneity (P≤0.1 orI2>50%), the random effect model and a funnel plot were used to observe the publication bias.
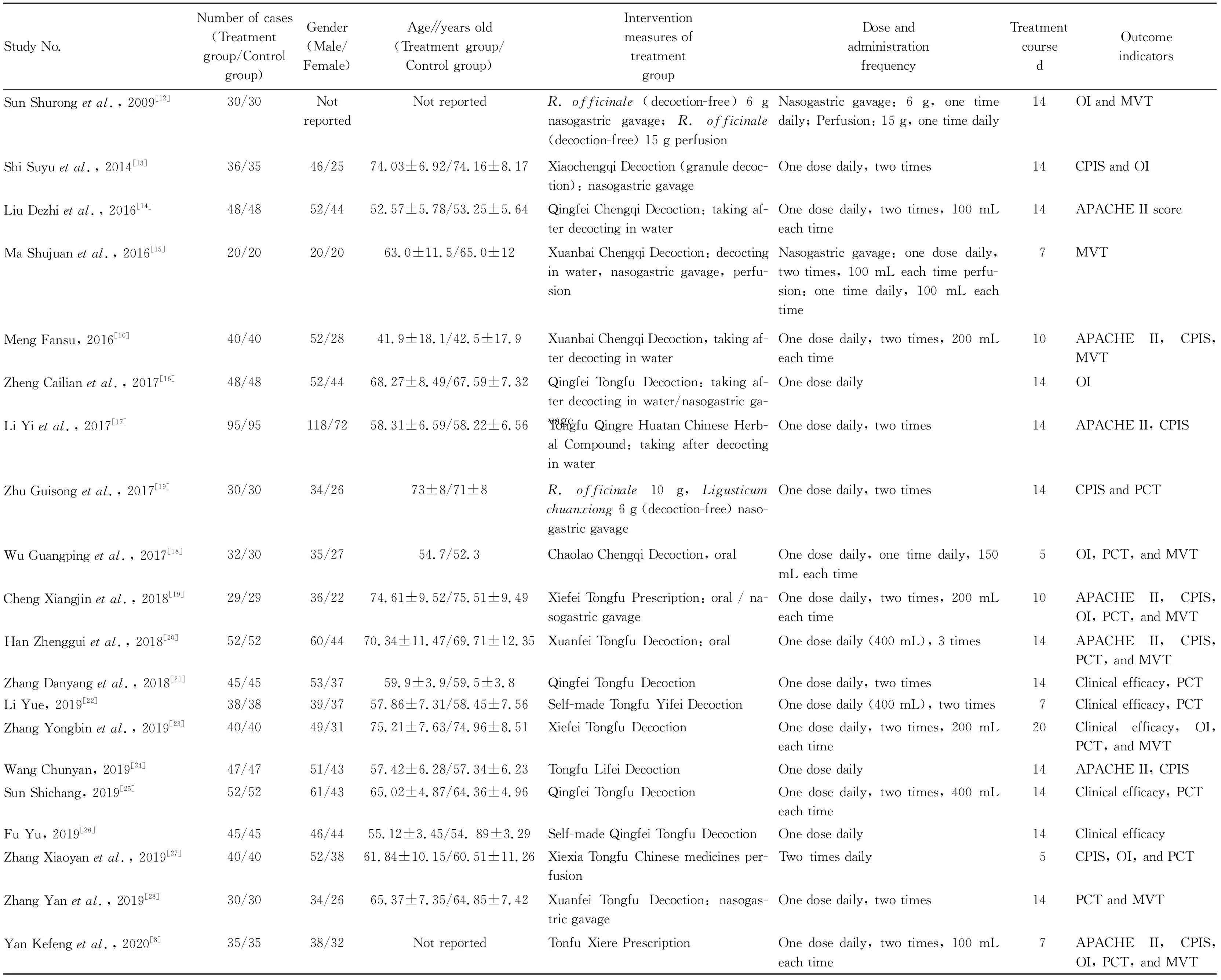
Table 1 Basic characteristics of the included studies
3 Results and analysis
3.1 Literature search resultsA total of 161 articles were retrieved. After reading the literature titles and abstracts, 86 articles containing duplicate literature, reviews, case reports, expert reviews, animal experiments, repeated publications, literature with clear research objects or interventions inconsistent with the inclusion criteria were excluded, 75 articles were included in the preliminary screening. After reading the full texts, 55 articles were excluded, and finally 20 articles were included, all these 29 articles were Chinese literature.
3.2 Information of patients in the included literatureTwenty RCTs[8-10, 12-28]included a total of 1 661 patients with severe pneumonia, of which 832 were in the treatment group and 829 were in the control group; 928 were males (55.87%), and 683 females (41.20%), one article[12]did not report the proportion of men and women included in the case, as shown in Table 1.
3.3 Literature quality assessmentIn the included 20 articles, 13 articles[8-9, 14, 16, 19-22, 24-28]provided random methods, and other articles did not explain the items in the risk assessment of bias, and none of them used the blind method, so the overall literature quality was low.
3.4 Clinical efficacy assessment
3.4.1Response rate. A total of 11 articles[10, 13-15, 17, 19-22, 25-26]were included, and there was no statistical heterogeneity among the results (P=1.21,I2=15%). The statistics were combined using the fixed effect model, and the relative risk (RR) was used as the effect scale. Fig.1 shows that the response rate in the experimental group was significantly higher than that in the control group [RR=1.21, 95%CI(1.14, 1.27),P<0.000 01]. The funnel plot analysis of this indicator shows that the left and right were not symmetrical, indicating that there was possible publication bias (Fig.2).
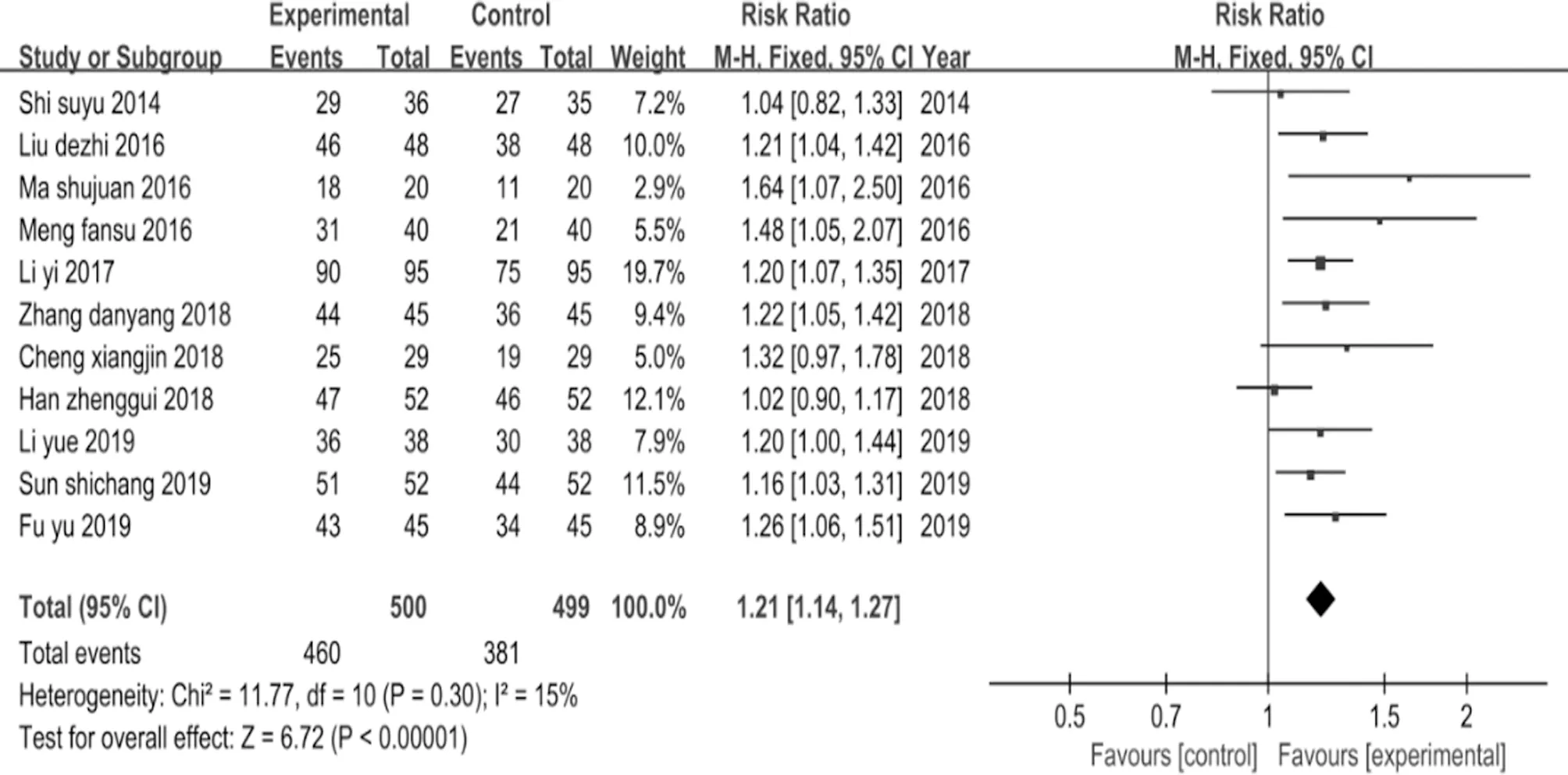
Fig.1 Meta-analysis forest map for the comparison of response rate between the two groups
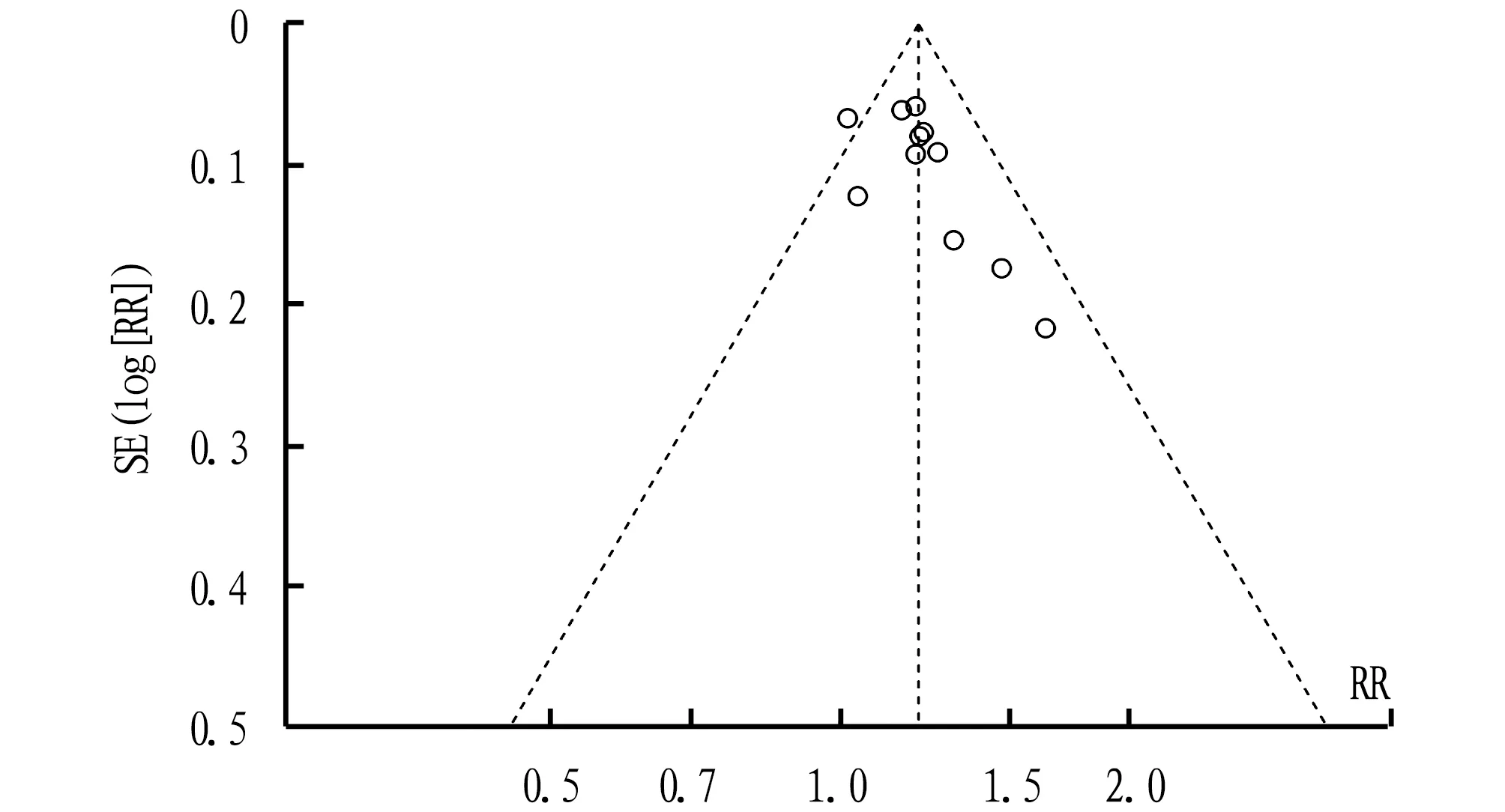
Fig.2 Funnel chart for the response rate intervention effect of purgation and catharsis method for patients with severe pneumonia
3.4.2APACHE II score. A total of 7 articles[8, 10, 14, 17, 19, 20, 24]were included, and there was statistical heterogeneity among the results (P<0.000 01,I2=97%). The statistics were combined using the random sampling effect model, and the WMD was used as the effect scale. Fig.3 shows that compared with the control group, the APACHE II score of the experimental group was significantly reduced [WMD=-5.92, 95%CI(-7.94, -3.89),P<0.000 01].

Fig.3 Meta-analysis forest map for the comparison of APACHE II score between the two groups
3.4.3CPIS. A total of 9 articles[8, -10, 13, 16-17, 19-20, 27]were included, and there was statistical heterogeneity among the results (P<0.006,I2=62%). The statistics were combined using the random sampling effect model, and theWMDwas used as the effect scale. Fig.4 shows that compared with the control group, the CPIS of the experimental group was significantly reduced [WMD=-1.41, 95%CI(-1.70, -1.12),P<0.000 01].
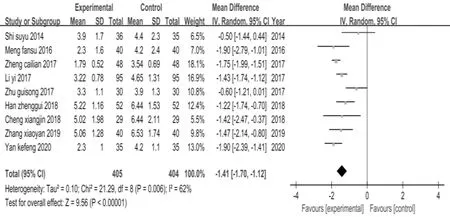
Fig.4 Meta-analysis forest map for the comparison of CPIS between the two groups
3.4.4OI. A total of 8 articles[8, 12-13, 16, 18-19, 23, 27]were included, and there was statistical heterogeneity among the results (P<0.000 1,I2=77%). The statistics were combined using the random sampling effect model, and theWMDwas used as the effect scale. Fig.5 showed that the OI was significantly improved in the experimental group than in the control group [WMD=39.52, 95%CI(29.39, 49.65),P< 0.000 01].
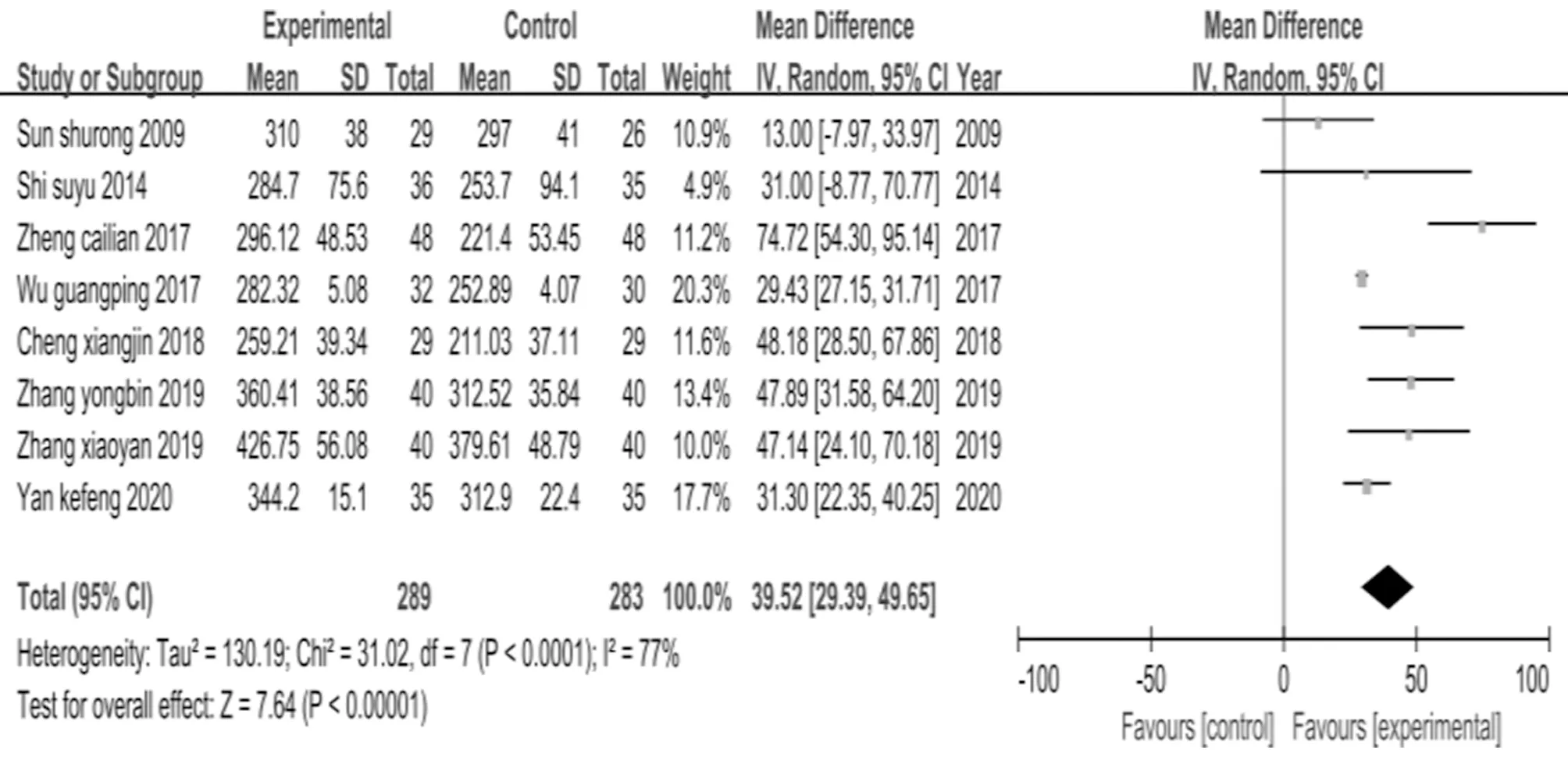
Fig.5 Meta-analysis forest map for the comparison of OI between the two groups
3.4.5PCT. A total of 12 articles[8-9, 18-25, 27-28]were included, and there was statistical heterogeneity among the results (P<0.000 01,I2=96%). The statistics were combined using the random sampling effect model, and theWMDwas used as the effect scale. Fig.6 shows that compared with the control group, the PCT of the experimental group was significantly reduced [WMD=-2.85, 95%CI(-3.68, -2.01),P<0.000 01]. The funnel plot analysis of this indicator shows that the left and right were not symmetrical, indicating that there was possible publication bias (Fig.7).
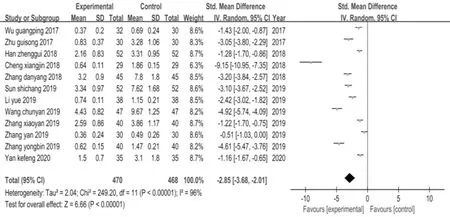
Fig.6 Meta-analysis forest map for the comparison of PCT between the two groups
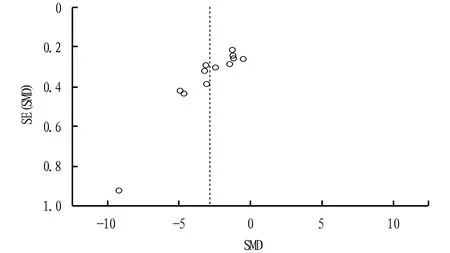
Fig.7 Funnel chart for the PCT intervention effect of purgation and catharsis method for patients with severe pneumonia
3.4.6MVT. A total of 9 articles[8, 10,12, 15, 18-20, 23, 28]were included, and there was statistical heterogeneity among the results (P<0.000 01,I2=99%). The statistics were combined using the random sampling effect model, and theWMDwas used as the effect scale. Fig.8 shows that compared with the control group, the MVT of the experimental group was signifi-cantly reduced [WMD=-13.00, 95%CI(-16.51, -9.48),P<0.000 01].
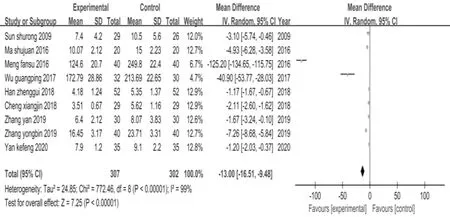
Fig.8 Meta-analysis forest map for the comparison of MVT between the two groups
3.5 Adverse reactionsIn the 20 articles included, only 7 articles[8-10, 15, 18, 23, 25]mentioned adverse reactions, and 1 article[8]reported diarrhea in both the experimental group and the control group, followed by vomiting, skin rash, no specific number of cases was reported; 1 article[23]reported 6 cases of mild skin irritation in the experimental group, manifested as skin burning, itching, and redness, which resolved spontaneously after 1 week without treatment; 5 cases in the control group had mild skin irritation, burning and itching; 1 article[25]reported 1 case of vomiting, 1 case of headache in the experimental group, 1 case of dizziness in the control group, and no statistical difference in the incidence of adverse reactions between the experimental group and the control group; the other 4 articles[ 9-10, 15, 18]had no adverse reactions.
4 Discussion
Severe pneumonia has the characteristics of rapid progress, many complications, and high mortality. These significantly increase the economic burden of patients. The evaluation of severe pneumonia includes two aspects: evaluation of the severity of pneumonia itself and evaluation of the degree of impairment of organ function. Clinically, a scoring system is usually used[1]. Oxygenation index (OI) and clinical pulmonary infection score (CPIS) are used to evaluate the severity of pneumonia itself, procalcitonin (PCT) is used to evaluate the degree of bacterial infection, and the above indicators can be used to evaluate the severity of pneumonia and the effect of treatment. Patients with severe pneumonia need to be admitted to ICU for treatment, and other organ dysfunctions are often combined. Therefore, patients with severe pneumonia need to be evaluated in terms of the degree of objective and quantifiable organ dysfunction. Multiple organ dysfunction syndrome (MODS) score, sepsis-related organ failure assessment (SOFA) score and acute physiology and chronic health evaluations II (APACHE II) score are often used, of which APACHE II score is relatively simple and reliable, and is the most widely used clinically[1]. The mechanical ventilation time (MVT) can be used to evaluate the effect of treatment, but because the cost of mechanical ventilation is relatively expensive, it can also be used to evaluate the degree of medical economic burden. The above indicators can comprehensively evaluate the clinical efficacy of patients with severe pneumonia. Therefore, the above indicators are used as evaluation indicators in this study.
According to the theory of traditional Chinese medicine, the lungs and the large intestine are exterior and interior. The purgation and catharsis method is an important method for treatment of severe pneumonia. There have been many reports about the treatment of severe pneumonia using the purgation and catharsis method, but there is still no systematic evaluation of the efficacy and safety of the purgation and catharsis method in the treatment of severe pneumonia. In this study, using meta-analysis, we systemically evaluated the clinical efficacy of the purgation and catharsis method in the treatment of severe pneumonia. The results indicate that the purgation and catharsis method combined with western medicine standardized treatment could reduce CPIS, increase the OI, improve the severity degree of pneumonia, reduce PCT level and infection level, increase APACHE II score, improve the functions of organs, and ultimately increase the clinical efficacy. Besides, the literature included in this study was only 20 articles, the number was small, and all were Chinese literature, and the cases included were domestic cases, so the extrapolation of the research results is limited. In addition, the overall quality of the included literature is low, and less attention is paid to adverse reactions and end-point events. Furthermore, the results of the literature included in the five observation indicators of APACHE II score, CPIS, OI, PCT and mechanical ventilation time are highly heterogeneous. This may be related to the severity of the disease between the studies, the conventional treatment methods of Western medicine are not the same, the experimental group’s traditional Chinese medicine prescriptions, traditional Chinese medicine administration methods, dosage, and frequency are different, and the measurement unit of the laboratory indicators is inconsistent. Finally, we conducted a funnel chart analysis in this study. The two sides of the funnel chart are asymmetrical, and the literature has publication bias. Therefore, the meta-analysis results have limitations. In summary, the purgation and catharsis method has certain advantages in the treatment of severe pneumonia, and the safety is high. However, it still needs more large-sample, high-quality randomized controlled trials with endpoint events as observation indicators to provide stronger evidence-based evidence.
- Medicinal Plant的其它文章
- Difference Analysis of Secondary Metabolites of Herba Polygoni Chinensis from Guangxi
- Effects of Temperature on Seed Germination and Metabolism of Scutellaria baicalensis Georgi
- Quality Standard of Quercetin in the Leaves of Heritiera littoralis
- Effect of ATM/CHK2/CDC25A Signal Pathway on the Resistance of Colorectal Cancer Cells to L-OHP
- Microbial Limit Test of Zhideke Granules
- Based on the Theory of Five Yun Six Qi to Study the Clinical Effect of Chaigui Decoction on Jueyin Type Hypertension