
Focuses and trends of the studies on pediatric palliative care:A bibliometric analysis from 2004 to 2018
2021-02-28 09:48MiaoZhangXiaohanLi
Miao Zhang,Xiaohan Li
School of Nursing,China Medical University,Shenyang,Liaoning,China
Keywords:Bibliometrics Communication Decision making Hospice and palliative care nursing Neoplasms Parents Pediatrics Professional-family relations
ABSTRACT Objectives:To investigate the focuses and trends of the studies on pediatric palliative care (PPC) and provide directions for future research.Methods:Relevant papers about PPC published from 2004 to 2018 were analyzed using bibliometric analysis methods,including co-word analysis,biclustering analysis,and strategic diagram analysis.The included papers were divided into three groups based on the publication time,including 2004-2008,2009-2013,and 2014-2018.Results:A total of 1132 papers were published between 2004 and 2018,and there were 293 papers published between 2004 and 2008,396 between 2009 and 2013,and 443 between 2014 and 2018.There were 42 high-frequency MeSH terms/MeSH subheadings in papers published between 2004 and 2018,including 12 between 2004 and 2008,13 between 2009 and 2013,and 17 between 2014 and 2018.Conclusion:Studies on PPC were making progress,with the increasing number,expanding scope,and uneven global distribution.Integration palliative care into pediatrics,cancer treatments in pediatric oncology,education methods on PPC,and establishment of professional teams were the major themes during 2004-2008,then the themes changed into establishing interventions to enhance the quality of life of the patients and parents,building professional-family relationship,and investigating attitude of health personnel in PPC during 2009-2013 and subsequently turned into communication skills,end-oflife decision making,and guidelines making on PPC during 2014-2018.Underdeveloped and protential themes including effective approaches to deal with the ethical dilemmas,training programs on communication skills,family support and guideline making are worth studying in the future.
What is known?
·Both the number of studies and the scope on pediatric palliative care improved from 2004 to 2018.However,the research focuses and trends have not been investigated yet.
What is new?
·Integration palliative care into pediatrics,pediatric palliative care interventions,methods to improve quality of life,and pain management in pediatric palliative care were the focuses from 2004 to 2018.
·Communication skills between professionals and parents,the methods of resolving ethical issues,family support and evidence-based guidelines are potential hotspots in the future.
1.Introduction
According to the estimate of the Centers for Disease Control and Prevention,approximately 2000 children had life-limiting diseases(LLDs) in the year 2017 in the USA,and the number had been increasing year by year[1].Connor et al.estimated that more than 21 million children needed pediatric palliative care(PPC)[2].When firstly put forward in the paper titled Dying children need help too by Chapman and Goodall[3],PPC aroused great attention.In 1998,PPC was officially defined as “the active total care of the child’s body,mind,and spirit,and also involved in giving support to the family and it began when illness was diagnosed,and continued regardless of whether or not a child received treatment directed at the disease” [4].Since 2003,PPC has been recognized as a pediatric subspecialty by the Royal College of Paediatrics and Child Health(RCPCH) [5],and more and more researchers have noticed that children with LLDs need more attention.In fact,PPC is far more different from the palliative care for adults [6],especially in care skills such as communication skills with children’s parents and dealing with bereavement care[7].For example,types of diseases,treatments,and various needs in different age groups.Moreover,13.6% of the children are undiagnosed,which increases the psychological burden of the parents [8].Although it is extremely suffering from losing a child,some parents gradually accept palliative care(PC)so that their children can go through the last period of life without over-treatment and unbearable suffering.
To better meet the increasing needs on PPC,the number of relevant research papers is increasing,focusing on different topics,such as suffering relief of the children[9],improving the quality of life of the whole family[10,11],and the therapy of neoplasms[12].Besides,the scope of studies on PPC has also been greatly extended from the children,parents[13],and children’s siblings[14]to the whole family [15].
Bibliometrics was defined as“the study and measurement of the publication patterns of all forms of written communication and their authors” [16],which took quantitative characteristic as research objects to analyze structural distribution,quantitative relation,and management of literature using math and statistic[17].Bibliometrics has been widely applied in biomedicine,psychiatry,military nursing [18],nursing management [19]and genomic nursing [20],but not in PPC as far as we could search in literature.Although there have been a large number of PPC related studies,the research focuses and trends remain unexplored.Therefore,it is meaningful to sort out the focuses,describe the dynamic trends,and predict the future research directions on PPC using bibliometric analysis methods.
In this study,2004 was the starting year because PPC became an independent subspecialty in 2000 in the United States [21]and subsequently it was recognized as a specialty by the Royal College of Paediatrics and Child Health and Royal College of Nursing in 2003[5].Formal recognition of a subspecialty or specialty by official organizations sets standards on which healthcare staff can rely[22].And 2018 was the ending year as the last search was run in July 2019.Fifteen years between 2004 and 2018 were equally divided into three periods:2004-2008,2009-2013,and 2014-2018,in reference to a systematic scoping review on palliative care [23].This study aimed to 1) identify the research focuses in the past 15 years,2) describe the changing trends of the three periods,and 3)predict the research trends in the future.
2.Methods
2.1.Design
Quantitative bibliometric analyses on PPC studies from 2004 to 2018 were carried out to figure out the research focuses and predict future directions.
2.2.Data collection
(((“Child"[MeSH]) OR “Pediatrics"[MeSH])) AND (“Terminal Care"[MeSH]OR “Palliative Care"[MeSH]OR “Hospice Care"[MeSH])for the literature search in PubMed database.The results were collected based on three periods,namely from January 1,2004 to December 31,2008 (2004-2008),from January 1,2009 to December 31,2013 (2009-2013),and from January 1,2014 to December 31,2018 (2014-2018).Since “pediatric” is spelled as“pediatric” in British English,the use of “pediatrics” as the MeSH term ensured complete research results.The language of the articles was limited to only English and the text availability was limited to full text.There was no restriction of article type as well as both“child”and“pediatric”were used so that we could enlarge the sample size to conduct the analyses more comprehensively.The primary results showed 571 literature published between 2004 and 2008,748 between 2009 and 2013,and 939 between 2014 and 2018.Subsequently,we checked the titles,abstracts,and full-texts(if necessary,namely the full-texts of studies needed to be read when we couldn’t exclude or include the studies according to the titles and abstracts) to screen out those irrelevant papers among the primary results (n=2,258).We double-checked the included records based on the relevance of PPC.Finally,we included 1,132 articles (Fig.1) and exported the data with the “XML” format.The ethics approval for this study was not required due to reusing preexisting literature in this study.
2.3.Data extraction and the formation of matrix
Co-word analysis can identify the relations of professional terms in relevant articles,based on the occurrence frequency of these terms,and demonstrate the theme structure changes [24].In this study,the frequency of MeSH terms/MeSH subheadings was calculated by Bibliographic Item Co-Occurrence Matrix Builder(BICOMB),and the high-frequency MeSH terms/MeSH subheadings were sorted into clusters by Graphical Cluster Toolkit (gCLUTO).BICOMB is a text mining system based on the co-occurrence of bibliographic items in literature databases,which was developed by Cui et al.in 2008[25].BICOMB can be used to sort out the MeSH terms/MeSH subheadings,publication years,countries,journals,authors and generate a co-occurrence matrix of the MeSH terms/MeSH subheadings.H-index was chosen to identify the highfrequency major MeSH terms/MeSH subheadings,which was first introduced by Hirsch to evaluate the research output of individuals[26].H-index was calculated according to a previously reported method [27].Firstly,the high-frequency entries were arranged according to the descending order of frequency,and the entries whose word frequency was greater than or equal to their serial number(h)were found out from the list of high-frequency entries,and the frequencies of subsequent terms were less than h.Thus,h was taken as the threshold for intercepting high-frequency terms,and the high-frequency MeSH terms-source article matrix was generated according to the intercepted high-frequency terms.Therefore,we respectively exported the high-frequency MeSH terms-source article matrix and co-occurrence matrix of the three periods.
2.4.Biclustering analysis
Biclustering analysis was proposed by Hartigan to sort heterogeneous data into a homogeneous block by constructing clusters of variables or cases [28].
Based on the high-frequency MeSH terms-source article matrix,gCLUTO 1.0 software (http://glaros.dtc.umn.edu/gkhome/cluto/gcluto) was utilized to conduct the biclustering analysis and create matrix visualization and mountain map.In this study,repeated bisection was selected as the biclustering method,cosine was selected as the similarity function,and I2was selected as the criterion function.Following the principles that external similarity(ESim) should be as small as possible while internal similarity(ISim) should be large,we constantly adjusted the number of clusters to obtain the optimal results.In the mountain map,the height of the peak is directly proportional to the ISim and the volume is proportional to the number of MeSH terms/MeSH subheadings each mountain contains.The distance between clusters stands for the similarity.Different colors of red,yellow,green,light blue,and dark blue are shown in the mountain map,but only the color of the peaks is informative,which represents the internal standard deviation(ISdev),such as red for small ISdev and blue for large ISdev.Red peaks indicate that the similarity of the articles within a cluster is high and the major topics of each cluster are consistent,while blue peaks mean that high variation among the contents.Through the biclustering analysis,the clusters of the three periods were generated.The semantic relations such as causation and influence relation among the high-frequency MeSH terms/MeSH subheadings within a cluster were used in combination with the representative articles of each cluster to conclude the theme of corresponding high-frequency MeSH terms.

Fig.1.Flowchart for literature selection.
2.5.Strategic diagram analysis
Strategic diagram analysis was firstly introduced in 1988 by Law et al.[29],which was described as a 2D coordinate system to show the structure of a field.In other words,it aimed to visually depict the position in the coordinate system of clusters and compared the trends of clusters in 3 periods by calculating the internal association within one cluster and external influences among the clusters.In detail,the x-axis stands for centrality,which represents the influences of clusters on each other by measuring the strength of links among clusters;the y-axis stands for density,representing the development conditions of a cluster by measuring the strength of internal association of MeSH terms/MeSH subheadings within this cluster.According to the co-occurrence matrix,each cluster’s centrality and density were calculated,and the 2D strategic diagram was subsequently delineated.The specific calculation method was illustrated by Callon et al.[30].
The meaning of a strategic diagram is as follows:x-axis(namely density)means internal closeness within the cluster,indicating the ability to sustain and develop itself,whereas y-axis (namely centrality)means external closeness with other clusters,indicating the degree to interact with other clusters.Clusters in quadrant 1 with high centrality and density mean themes of these clusters are the focuses.Quadrant 2 involves clusters with high density but weak centrality,which means they are specialized and less integrated with other disciplines.Clusters with both low centrality and density in quadrant 3 are emerging or outdated and these clusters are less interconnected not only within the cluster but also among other clusters.Clusters with strong centrality but weak density in quadrant 4 mean that although they are closely correlated with other clusters,internal development within the cluster is still immature.
3.Results
3.1.Distribution of the research output
The 1,132 papers included in this study between 2004 and 2018 were divided into three groups based on the publication time.In general,the number of studies was steadily rising,with 293 published between 2004 and 2008,396 between 2009 and 2013,and 443 between 2014 and 2018.The numbers of studies refined by the items of country,journal,and author are shown in Table 1.Most of the articles were published based on research departments in the United States,England,and Germany.Journal of Palliative Medicine has maintained the top highly produced journal since 2004.The authors with the largest numbers of published papers during the three periods were Jones BL,Knapp C,and Downing J,respectively(Table 1).
3.2.High-frequency MeSH terms/MeSH subheadings and the results of biclustering analysis
High-frequency MeSH terms/MeSH subheadings during the three periods were ranked to conclude the corresponding themes since they represent the research focuses.The matrix visualizations show that there were 42 high-frequency MeSH terms/MeSH subheadings between 2004 and 2018,and the number was 12 between 2004 and 2008,13 between 2009 and 2013,and 17 between 2014 and 2018,which were listed on the right side of Figs.2B-4B,respectively.The left hierarchical trees indicate the relationship among the highfrequency MeSH terms/MeSH subheadings,and the top ones represent the relationship among the term-resources articles.Besides,these 12 high-frequency MeSH terms/MeSH subheadings between 2004 and 2008 can be classified into five clusters(Fig.2A).Likewise,the 13 high-frequency MeSH terms/MeSH subheadings between 2009 and 2013,and 17 high-frequency MeSH terms/MeSH subheadings between 2014 and 2018 can be classified into five clusters(Figure 3A) and 6 clusters (Fig.4A),respectively.As shown in the mountain map (Figs.2A-4A),there are red peaks of cluster 2(establishment of a PPC team) of the first period,cluster 2 (professional-family relations) and 3 (interventions on PPC) of the second period,and cluster 2(pain management in PPC)of the third period.The rest of the peaks are light blue ordark blue in these three periods.Furthermore,semantic relation[31]among the high-frequency major MeSH terms/MeSH subheadings were analyzed in combination with the representative articles of each cluster to summarize 5,5,and 6 themes,respectively,in the three periods(Table 2).
3.3.Changes of the research themes on PPC
The results of the strategic diagram analysis are shown in Figs.2C-4C.According to the calculated results,the clusters fell in different quadrants,representing the development conditions of them.For the results of the articles published during 2004-2008,cluster 0 (integration palliative care[PC]into pediatrics) is in the first quadrant.Cluster 1(cancer treatments in pediatric oncology),2(establishment of a PPC team),3(education methods on PPC),and 4(parents’ attitude to their child’s death) are in the third quadrant.
And the results between 2009 and 2013 show that clusters 1(methods to improve quality of life in PPC)and 3(interventions on PPC) are in quadrant 1.Cluster 0 (palliative care in pediatric intensive care units) is located in quadrant 3.Quadrant 4 includes clusters 2 (professional-family relations) and 4 (ethics on PPC and attitude of health personnel in PPC).
For the results in the last period,cluster 2(pain management in PPC) is in quadrant 1.Clusters 0 (attitude of health personnel in PPC) and 4 (communication skills on PPC) are included in the second quadrant.Cluster 1(family support in PPC)is in quadrant 3.And clusters in quadrant 4 are clusters 3 (end-of-life decisionmaking in PPC) and 5 (guideline making on PPC).
4.Discussion
4.1.Interpretation of the results
More and more researchers,especially health professionals in the pediatric oncology field have been studying PPC,and progress has been made in the past 15 years.In this study,co-word analysis,biclustering analysis,and strategic diagram analysis were combined to identify the research focuses in different periods and reveal the trends in the past 15 years.
Although the amount of literature on PPC was increasing,there was a problem that most of the studies were carried out in developed countries instead of being distributed evenly in the world.It can be explained to some extent that there were better economic conditions,policy-making,medical systems,curriculum design,personnel training,and well-established policies in the developed countries at the onset of the studies on PPC [32,33].Besides,the liberal and sociocultural context is also supposed to be taken into consideration [34].We suggest that the developing countries or regions learn the advanced experiences from the developed countries while considering the local situation,to establish their own completed systems.More remarkable and novel findings are expected in a variety of regions to further promote the development of PPC [35,36].
The trends in the changes of the research themes can be explained that the integration of pediatric oncology and PC was the focus and well-developed in the first period.The status quo of palliative care in pediatric oncology,caring for a dying child [37],and education for physicians [38]had been reported during 2004-2008.Place of death,cause of death,funding of PPC,and bereavement care were the most mentioned of the literature in this period [39-41].The frequent place of death for children with lifelimiting conditions was shifted gradually from hospital to community.The percentage of in-hospital death decreased from 83.8%in 2004 to 68.1% in 2014 in England[42].It was also reported that the establishment of a PPC team [43],including professional palliative care teams,psychotherapists,and priests,would facilitate the implementation and development of PPC.Cancer treatments in pediatric oncology,the establishment of a PPC team,education methods on PPC,and parents’ attitude to their child’s death werethe emerging topics during 2004-2008.It is plausible that these clusters will move to other quadrants as time goes by because studies on PPC are becoming more and more popular.There were many fresh ideas but immature in this period.

Table 1 The top three countries,journals and authors of research output on PPC.

Fig.2.Biclustering analysis (A & B) and strategic diagram (C) on PPC in 2004-2008.
Subsequently,quality of life improvement and PPC interventions were focuses in the second period (2009-2013).Most of these interventions were non-pharmaceutical therapies[44,45].For example,music therapy for children in the terminal stage was an effective way to relieve physical and psychological suffering while improving quality of life.Meanwhile,it helped to enhance family bonding and strengthen family cohesion in tough times.In addition,some undeveloped topics were showing up,such as ethics on PPC,attitudes of health personnel in PPC and professionalfamily relations during 2009-2013.
As for ethics,healthcare staff often encountered ethical dilemmas in caring for dying children,such as truth-telling,the best ethical decision making,and do-not-resuscitate (DNR) [46,47].For the family,medical decisions of children generally relied on the parents’willingness,which was influenced by income,relationship,and education.Children were more willing to be included in informing the medical progress,even in the decision about death[48,49].Thus,the voice of children also needs to be further explored.It was essential to suit preferred ethical options for individuals,which varied in different sociocultural contexts and political systems.The attitude of professionals directly influenced the clinical practice,patients’ feelings,parents’ choices and development of PPC [50].Attitudes of health personnel depended on how they experience in the caring or treating and the knowledge and skills on PPC they got [51].Barriers including uncertain prognosis,language barriers,and time constraints frequently or almost always occurred during the caring,which might lead to the staff members’negative emotions,resulting in changes in their attitude[52].PC in pediatric intensive care units became less focused in this period due to comprehensive research in the first period.

Fig.3.Biclustering analysis (A & B) and strategic diagram (C) on PPC in 2009-2013.
In the third period,we can find that health personnel’s attitude[53]moved from quadrant 4 in the second period to quadrant 2,which also was an improvement from immature to mature.Professional-family relations emphasized offering psychological support in the second period,and communication skills were indispensable to maintain and improve the relationship [54,55].Some high-frequency MeSH terms/MeSH subheadings in the second period,such as parents’attitude to death[56]and ethics on PPC[57]reoccurred in the third period.It is worth noting that the same themes may show up in different periods.It may be because studies on the same themes were first conducted in developed countries or regions and gradually extended to other developing countries or regions.
Furthermore,some new topics emerged,such as communication skills [58]and guideline making on PPC [59,60]during 2014-2018.Based on this,we can reasonably speculate that communication skills,guideline making,or policy setting may become the future research hotspots.Besides,there is only one cluster in the quadrant 1 in the first period,indicating superficial research on PPC;there are two clusters in the quadrant 1 and 4 in the second period; finally,there are clusters in every quadrant in the third period,demonstrating the researching scope was expanding.The three strategic diagrams show that the MeSH subheading (organization and administration of PPC) shows up in every period,suggesting that it takes a long time to build a specialized and collaborative team to work on PPC [61].
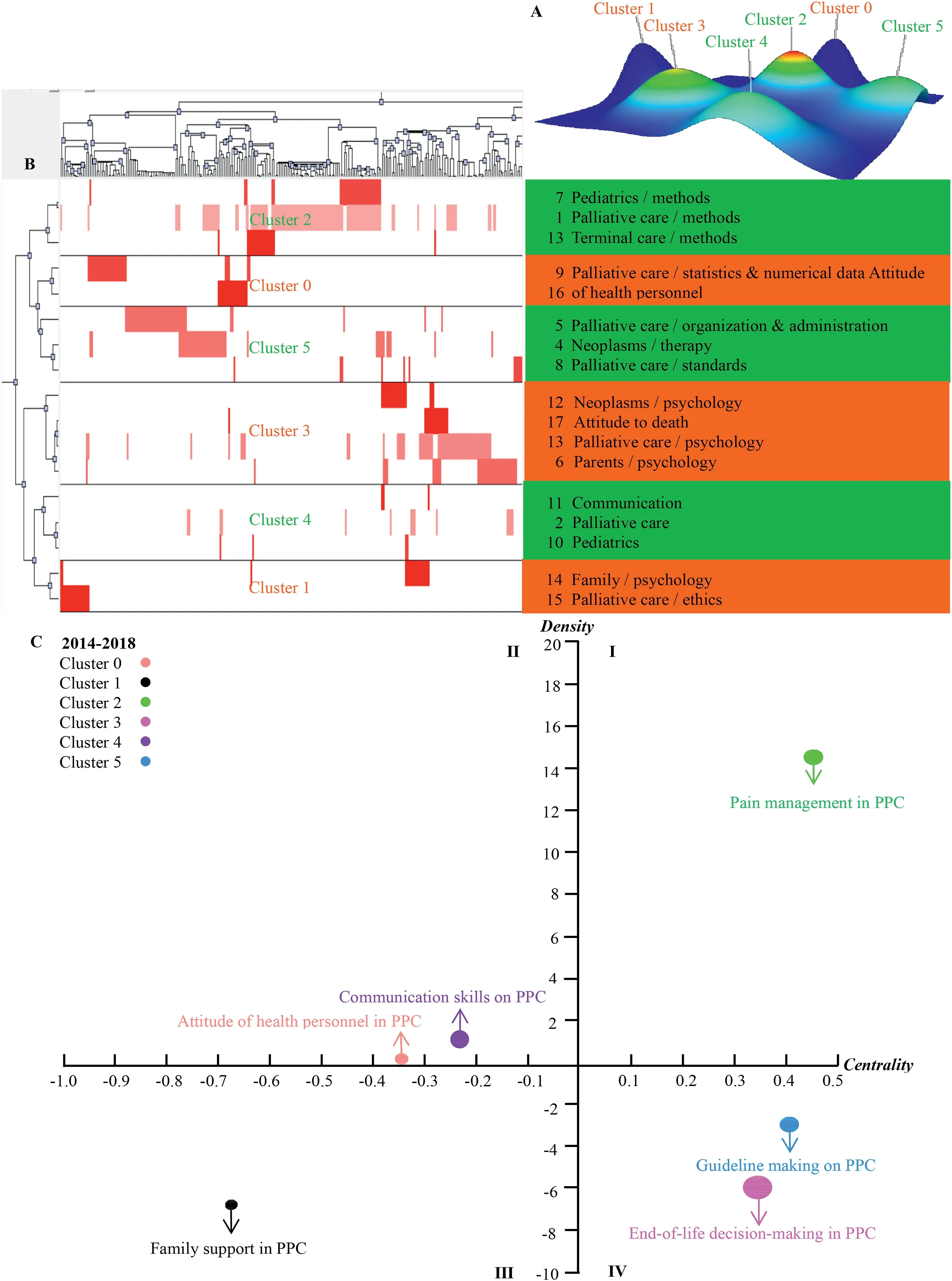
Fig.4.Biclustering analysis (A & B) and strategic diagram (C) on PPC in 2014-2018.
According to our findings,the research trends in the future were concluded as follows.Ethics on PPC was in quadrant 4 in the second period,indicating studies on these themes have been carried out yet still under development.Ethical dilemmas within PPC faced by healthcare staff were mainly conflicting over the right to treatment and withholding,decision-making in the child’s best interests and communication [62].Effective approaches discussed by treatment teams,parents,children and bioethics committees to deal with these issues are required in the future.In the third period,communication skills was in quadrant 2,showing that indistinctive progress has been made on these themes.The difficulties and experiences of professionals when delivering end-of-life discussion inPPC=pediatric palliative care.PPC have been reported [63,64].Nevertheless,training programs on communication skills were still inadequate.Family support was in the quadrant 3 in the third period,indicating family-centered approaches compared to patient-centered ones were a newlydeveloping area.Family support was included in the definition of PPC,and the child and family should be treated as a unit [20].Although the whole family was affected by the child’s illness,most studies focused on parents’needs recently,and the experiences and needs of siblings or even grandparents need to be discovered.Guideline making was in quadrant 4 in the third period,demonstrating that they have advanced to the middle level with a great promise in the future.Guidelines focused on the PPC concepts,principles and models from policymakers’ or societal perspectives in the last two decades,while these theoretical guidelines may not be suitable to the complex and dynamic medical settings [59].In addition,guidelines on bereavement care pathways,multidisciplinary teams and critical assessments are needed [59].End-of-life decision-making was also in quadrant 4 in this period.End-of-life decision making should involve parents and other family members,professionals and the child.The attitudes of parents,nurses and physicians on the decision-making process and the factors influencing the final decision have been discussed.However,the child’s own thoughts and preferences on the decisionmaking need to be explored[65].

Table 2 Outcomes of biclustering analysis of high-frequency MeSH terms/MeSH articles in three periods.
4.2.Limitations
Even though we employed three analysis methods to conduct a comprehensive study as much as possible,there are still some limitations.Literature in Web of Science and PubMed could be analyzed by BICOMB.The MeSH terms/MeSH subheadings were sorted out for literature in PubMed while keywords were sorted out for literature in Web of Science.In addition,the number of included studies in PubMed was more than those in Web of Science.And the final included studies in PubMed contained the studies that met the inclusion criteria in Web of Science.Therefore literature was only chosen in PubMed as MeSH terms are only available in this database.More comprehensive research conditions may be acquired by employing more databases with the implementation of more advanced software in the future.In addition,only the publications of English studies were searched,which may have resulted in missing some points.
5.Conclusion
In this study,we analyzed the research focuses in three periods of the past 15 years and compared the number of publications and trends in the changes of research themes,aiming to provide evidence of PPC development for researchers,policymakers,and leaders.The results suggest that PPC is in a developing period,with an increasing number and variety of literature but an uneven research distribution in the world.Because of the uneven global distribution of the studies,other countries or regions can develop their models on PPC according to the local situation based on those in the lead.The conclusions are as follows.1) Integration PC into pediatrics,interventions on PPC,methods to improve quality of life,and pain management were the focuses from 2004 to 2018.2)The trends in the changes of the research themes followed the sequence.Integration PC into pediatrics,cancer treatments in pediatric oncology,education methods,and professional team establishment were the major themes during 2004-2008.Then the themes changed into establishing interventions to enhance the life quality of the patients and parents,building professional-family relationships,and investigating the attitude of healthcare staff during 2009-2013 and subsequently turned into communication skills,end-of-life decision making,and guideline making on PPC during 2014-2018.3) Ethical dilemmas within PPC,training programs on communication skills,family support for children who have life-limiting diseases,and evidence-based guidelines from different countries are potential hotspots in the future.
CRediT authorship contribution statement
Miao Zhang:Conceptualization,Methodology,Writing-Original draft preparation.Xiaohan Li:Writing-Review and Editing,Supervision.
Funding
This research did not receive any specific grant from funding agencies in the public,commercial,or not-for-profit sectors.
Declaration of competing interest
The authors declare no potential conflicts of interest.
Acknowledgement
We are grateful to Malcolm Peak and Shi Bei for their contribution to this work.
Appendix A.Supplementary data
Supplementary data related to this article can be found at https://doi.org/10.1016/j.ijnss.2020.11.005.
 International Journal of Nursing Sciences2021年1期
International Journal of Nursing Sciences2021年1期
- International Journal of Nursing Sciences的其它文章
- Relationship between negative emotions and perceived support among parents of hospitalized,critically ill children
- The effect of digital health technologies on managing symptoms across pediatric cancer continuum:A systematic review
- Effectiveness of animal-assisted therapy on pain in children:A systematic review and meta-analysis
- Effects of creative expression program on the event-related potential and task reaction time of elderly with mild cognitive impairment
- Struggling to live a new normal life among Chinese women after losing an only child:A qualitative study
- Implementation and evaluation of a pain management core competency education program for surgical nurses