
Carcinoma bladder and sliding bladder hernia: Unusual association of paramount significance
2020-06-28 07:39:44ManavAgrawalGauravGargSunnyGoelManojKumar
Asian Journal of Urology 2020年2期
Manav Agrawal, Gaurav Garg*, Sunny Goel, Manoj Kumar
Department of Urology, King George’s Medical University, Lucknow, Uttar Pradesh, India
A 60-year-old man,a diagnosed case of inguinal hernia was referred for evaluation of voiding lower urinary tract symptoms (LUTS). There was no history of hematuria. On local examination,he had right-sided-direct inguinal hernia with right hydrocoele. Routine biochemical parameters were within normal limits. Urine routine microscopy revealed presence of field full of red blood cells. On uroflowmetry there was presence of decreased peak flow rate (12 mL/s)and average flow rate (8 mL/s). Ultrasound examination of the abdomen revealed presence of urinary bladder mass(35 mm × 21 mm) in right posterior wall with right hydroureteronephrosis and 19 mL prostate. Further evaluation with contrast-enhanced CT (CECT) of abdomen showed a well-defined polypoidal mass(43 mm×21 mm)arising from the right posterior wall involving the vesicoureteric junction, causing right-sided hydroureteronephrosis. There was evidence of right-sided inguinal hernia(containing omental fat and part of bladder wall) extending to upper pole of scrotum with right vaginal hydrocele (Figs. 1 and 2).Cystoscopy revealed a ~4 cm × 2 cm polypoidal growth involving right uretero-vesical (UV) junction but herniation of bladder was not seen, and transurethral resection of bladder tumor(TURBT)was done.Histopathology report was suggestive of transitional cell carcinoma, low grade, and non-muscle invasive. Follow-up and cystoscopy after 3-months revealed no evidence of tumor re-growth. Subsequently, the patient underwent right-sided Lichtenstein mesh hernioplasty and hydrocelectomy. Postoperative course was uneventful. The patient is now under regular follow up. Elderly patients having an inguinal hernia with voiding LUTS are often referred to urologists and most of them are found to have benign prostate hyperplasia/cystitis[1]. This was an unusual case in which the cause of voiding LUTS was inguinal bladder hernia (IBH) and/or bladder tumor.Around 1% -4% of inguinal hernias are associated with herniation of the bladder [1]. IBH results from the bladder being pulled out with a sheath of peritoneum into direct hernial sac due to factors like obesity,chronic urinary tract obstruction,decreased tone of the bladder and pelvic floor muscles [1,2]. Neoplasm of urinary bladder coexisting with IBH is uncommon. Oruc? et al. [3] reported that urological malignancies were found in 11.2% cases of IBH.Ugur et al.[4]reported case of a 75-year-old male with inguinal bladder hernia and proposed that preoperative diagnosis of this condition can prevent complications like bladder injury[4].Occurrence of IBH is more likely to occur in elderly patients having inguinal hernia with accompanying LUTS [5]. CECT abdomen is the best diagnostic imaging modality for evaluation and diagnosis of IBH with co-existing bladder neoplasms [5]. Preoperative diagnosis of inguinal bladder hernias with co-existing bladder neoplasms can modify the treatment approach of an inguinal hernia and may prevent inadvertent surgical bladder injuries.
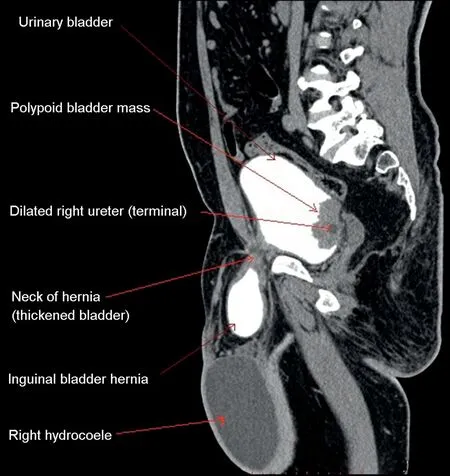
Figure 1 Contrast-enhanced computed tomography sagittal section image depicting the presence of polypoidal bladder mass arising from the right posterior wall with the presence of inguinal bladder hernia and hydrocoele.
Author contributions
Study concept and design: Manav Agrawal, Manoj Kumar Data acquisition: Gaurav Garg, Sunny Goel
Drafting of manuscript: Manav Agrawal, Gaurav Garg Critical revision of the manuscript: Manoj Kumar.
Conflicts of interest
The authors declare no conflict of interest.
 Asian Journal of Urology2020年2期
Asian Journal of Urology2020年2期
- Asian Journal of Urology的其它文章
- Robot-assisted laparoscopic prostatectomy:How can we get better?
- Management of staghorn stones in special situations
- Preoperative imaging in staghorn calculi,planning and decision making in management of staghorn calculi
- Staghorn calculi: Understanding the paradigm shift in management
- Total pelvic exenteration and a new model of diversion for giant primitive neuroectodermal tumor of prostate: A case report and review of the literature
- A prospective study of patient reported urinary incontinence among American,Norwegian and Spanish men 1 year after prostatectomy