
Total pelvic exenteration and a new model of diversion for giant primitive neuroectodermal tumor of prostate: A case report and review of the literature
2020-06-28 07:39:42LichenTengLingjunWeiLiLiYongpengXuYongshengChenYnCoWentoWngChngfuLi
Asian Journal of Urology 2020年2期
Lichen Teng , Lingjun Wei , Li Li , Yongpeng Xu ,Yongsheng Chen , Yn Co , Wento Wng , Chngfu Li ,*
a Department of Urology, Harbin Medical University Cancer Hospital, Harbin, China
b Department of Colorectal Surgery, Harbin Medical University Cancer Hospital, Harbin, China
Abstract The present study reports a rare primitive neuroectodermal tumor (PNET) of prostate. A 27-year-old male was admitted to Harbin Medical University Cancer Hospital (Harbin,China)for dysuria and dyschezia.Magnetic resonance imaging(MRI)revealed a large mass that may involve the bladder and rectum next to the prostate. Histopathological analysis of biopsy of prostate indicated mesenchymal origin tumor, and immunohistochemistric staining confirmed diagnosis of PNET of prostate. En bloc total pelvic exenteration and double barrel sigmoidostomy were performed. Double stomas in the skin incision were used for fecal and urinary diversion, respectively. Short-term outcome is satisfactory, while long-term efficacy remains to be poor. Clinical features of PNET of prostate should be paid much more attention and radical surgery and adjuvant chemotherapy should be recommended.
KEYWORDS Prostate;Primitive neuroectodermal tumor;Total pelvic exenteration;Double barrel sigmoidostomy
1. Introduction
According to the tissue of origin, primitive neuroectodermal tumor (PNET) is divided into central PNET and peripheral PNET. A large size of infiltrative soft mass is a common feature of them [1]. The incidence of PNET occurring in urological organs is very rare, previous reports about PNET mainly located in kidney, bladder, and adrenal glands. Compared with these organs, PNET of prostate is rarer, until 2003, Peyromaure et al. [2] documented the first case in the world.Up to date,only less than 20 cases of PNET of prostate were reported. Like other tumors of mesenchymal tissue, the PNET of prostate shows a poor prognosis. Currently, combined therapies, including surgery, chemotherapy, and radiotherapy, have been considered.As for the most urologic oncologists,it is very difficult to choose an optimal therapy regimen. At December of 2016, we treated a patient with PNET in the prostate using the total pelvic exenteration and double barrel sigmoidostomy for double diversion in our hospital, and obtained satisfactory short-term efficacy. Written informed consent was obtained from the family of the patient. The report was approved by the ethics committee (No. 161109).
2. Case report
A 27-year-old male patient presented to the Outpatient of Harbin Medical University Cancer Hospital (Harbin, China),who complained symptoms of fever, dysuria and dyschezia for 2 weeks. Moreover, he had been indwelled a catheter for 2 days prior to admission. His temperature went up to 39°C. We took the digital rectal examination after hospitalization, and the result indicated that a large smooth mass significantly swelled to the rectal cavity. Laboratory examination showed that value of serum prostate-special antigen (PSA) was 1.52 ng/mL and white blood cells (WBC)were 13×109/L,and the magnetic resonance imaging(MRI)revealed a 84 mm × 78 mm × 72 mm mass replaced the prostate gland,which may involve posterior wall of bladder and anterior wall of rectum (Fig. 1). Transrectal biopsy of the prostate gland was performed. Pathological analysis demonstrated malignant tumor of prostate gland mesenchymal origin and untypical morphology. The tumor cells were positive for Desmin and Vim and negative for CD34,CD117 and smooth muscle actin (SMA). The patient was diagnosed as giant prostate malignant tumor and urinary tract infection. After antibiotic treatment of couple days,we carefully communicated with the patient and his family members about regiment of treatment.Finally,the patient received total pelvic exenteration and double barrel sigmoidostomy. During operation, we found a large firm mass companied with seriously surrounding tissue edema,which fixed in pelvic cavity.After en bloc resection of total pelvic organs, 15 cm distal sigmoid colon of stoma was closed. Bilateral ureters were anastomosed end-to-side with sigmoid colon respectively, in which stents were indwelled. The anastomotic site was placed in retroperitoneal space. While faeces were evacuated through upper stoma, urine was discharged via lower one (Fig. 2). At 48 h after operation, the patient started to drink, and then was allowed to eat at the 4 day postoperation. The patient could freely ambulate from postoperative day 5, and he was discharged from hospital at 2 week post operation.The histopathological study revealed that area of tumor was filled with a lot of small round cells (Fig. 3A), indicating a PNET. Moreover, bladder and rectum were involved, and pelvic lymph nodes were free of metastasis.The cells were positive for CD99, CD56 and Vim (Fig.3B and C and D), and negative for CK and CD34 (Fig. 3E and F). The patient was found to have lung metastasis and the peritoneal recurrence at postoperative 5 months, and he finally died of multiple organ failure.

Figure 1 Magnetic resonance image(MRI)of the pelvic region.(A)Coronal T2-weighted scan revealing adherence between mass and base of bladder; (B) Sagital T2-weighted image showing a 84 mm × 78 mm × 72 mm mass replaced prostate gland, which compressed posteriorly rectum and superiorly bladder,respectively; (C) Transverse image showing the mass potentially adhere to pelvic wall.
3. Discussion
PNET is a kind of extremely rare malignant tumor with high aggressiveness. Early diagnosis and timely radical surgery would contribute to the prolonged survival of patients.Therefore,to early diagnose and treat PNET of prostate for the satisfactory outcome, it is very helpful to deeply understand its clinical features, and to reasonably choose treatment regimen.
Peripheral PNET could originate from the different organs or tissues, such as lung, liver, vertebra, et al.,however,PNET of urologic organs-origin is rare occurrence.According to the previous reports, kidney is a common organ of origin, and compared with kidney, incidence of PNET in prostate gland is much less. Additionally, the disease commonly occurs in the 20-to 30-year-old population.
To our best knowledge, since 2003 to now, totally 16 cases along with the present case have been reported[2-16], with median age of 27 years (Table 1). Due to insidious onset, there is commonly asymptomatics for the patients at early stage,thereafter,with increasing of tumor size,significant dysuria and dyschezia would seriously affect life style of the patients, and hematuria and chronic anal pains were complained by some patients. In addition, a lot of residual urine and frequent indwelling catheter would also result in refractory urinary tract infections.All of cases exhibited large diameter of primary mass (>5 cm) at the time of diagnosis.Digital rectal exam should be performed.Similarly to our case, the value of PSA maintain in the normal range in most cases except for three cases [7,8].Primary tumor appears rapid progress. For example, in the present case, the diameter of tumor increased by about 1 cm per month, and incidence of multiple systemic metastases for PNET of prostate gland was low. Two cases of pulmonary and lymph node metastasis were reported[9,10].Imaging examinations, such as computed tomography (CT)and MRI can show a large occupying lesion replaced prostate gland in the pelvic cavity,which may involve in surrounding organs or pelvic wall, such as bladder, rectum or seminal vesicles. Besides some necessary imaging examinations,establishment of PNET of prostate gland mainly bases on the immunohistochemistric staining, which can confirm PNET by positive for CD99 and/or other neuronal markers in many small round cells. At the same time, lymphoma and myogenic tumor should be excluded. In addition, because PNET in the prostate is a very rare disease,its pathogenesis still remains unclear,and a recent published report based on screening differentially expressed genes and constructing protein-protein interaction network found that calcium signaling pathway and several genes (CDK1, CDC20, BUB1B,and BUB1) may involve in the pathogenesis of the supratentorial PNET [17]. These genes should be further confirmed in the PNET of prostate in the near future.
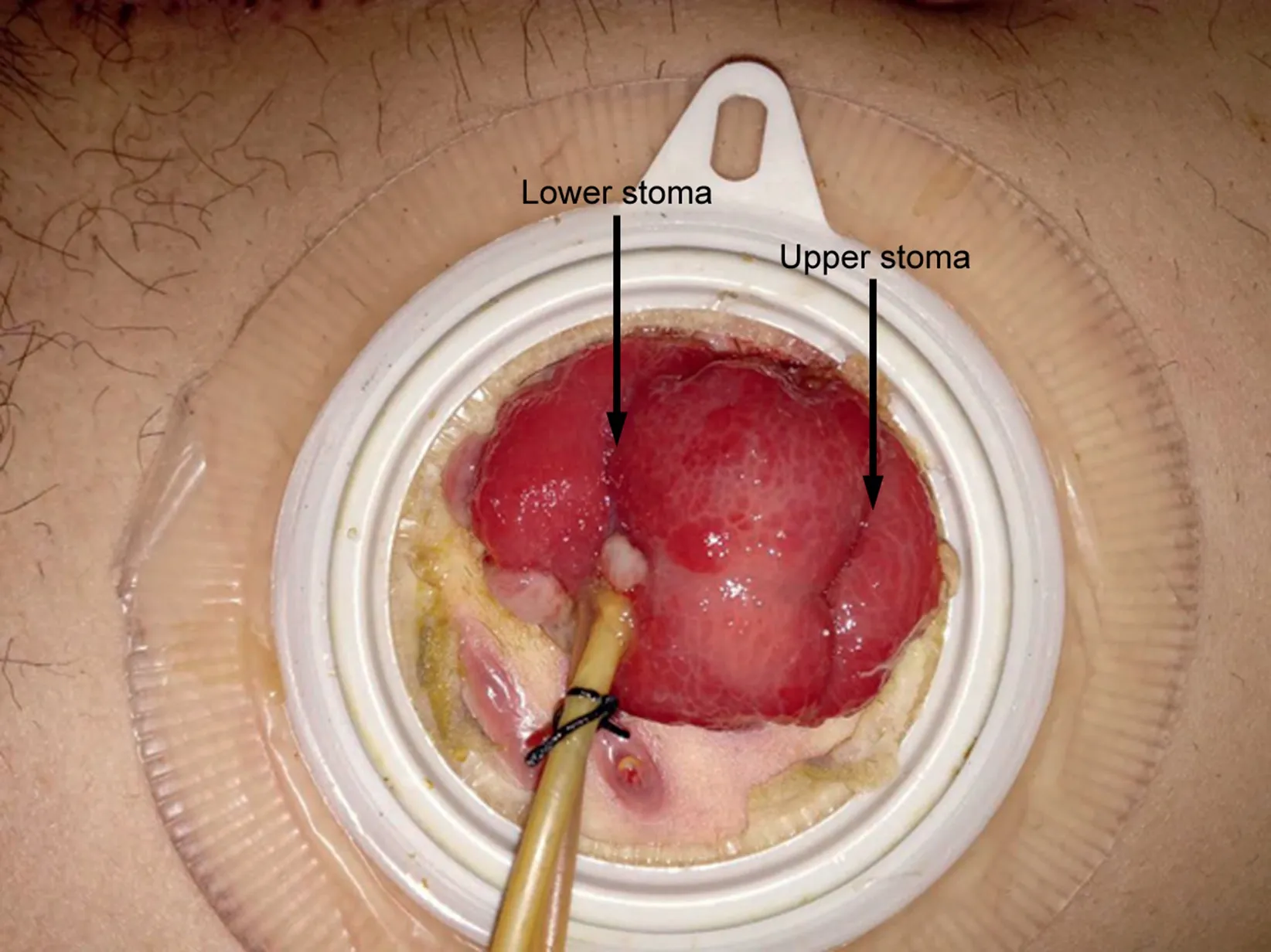
Figure 2 Double barrel sigmoidostomy: Upper stoma is used for fecal diversion,and lower one is used for urinary diversion.

Figure 3 Reprehensive images with H&E staining and immunohistochemistric staining. (A) H&E staining revealed a lot of small round cells distributed in tumor region (×200); (B) Immunohistochemistric staining demonstrating small round cells positive for CD99 (×200); (C) and (D) reveal small round cells is positive for CD56 and Vim, respectively (×200); (E) and (F) show small round cells negative for CK (×200) and CD34 (×100), respectively.
Due to the low incidence of PNET of the prostate and cohort study of large number of cases, currently, the standard treatment regimen has not yet been established.In previous studies, combined therapy with surgery, neoadjuvant or adjuvant chemotherapy and radiation therapy were effective, and most of cases underwent radical prostatectomy[2,3,9,11].Because peripheral PNET is prone to develop distant metastases and local recurrence within 2-3 year after surgery, to decrease this possibility, as for localized PNET of prostate, we performed aggressively an en bloc total pelvic exenteration in the present case, and double barrel sigmoidostomy was used for both the urinary and fecal diversions [18]. Compared with ureterostomy or urinary conduit diversion, we took advantage of reflected part of sigmoid colon with end in subtle ways as urinary diversion.It is helpful to take supportive care for the stoma and improve quality of life.More importantly,the operation did not further increase incidence of related complications,such as gut leakage and urinary tract infection. Moreover,surgical complexity is not increased furthermore. In addition to radical surgery, chemotherapy is a potentially effective treatment for localized PNET of the prostate[19].Chemotherapeutic agents include incristine, adriamycin/doxorubicin, cyclophosphamide and actinomycin-D, which are commonly used in combination with each other [20].
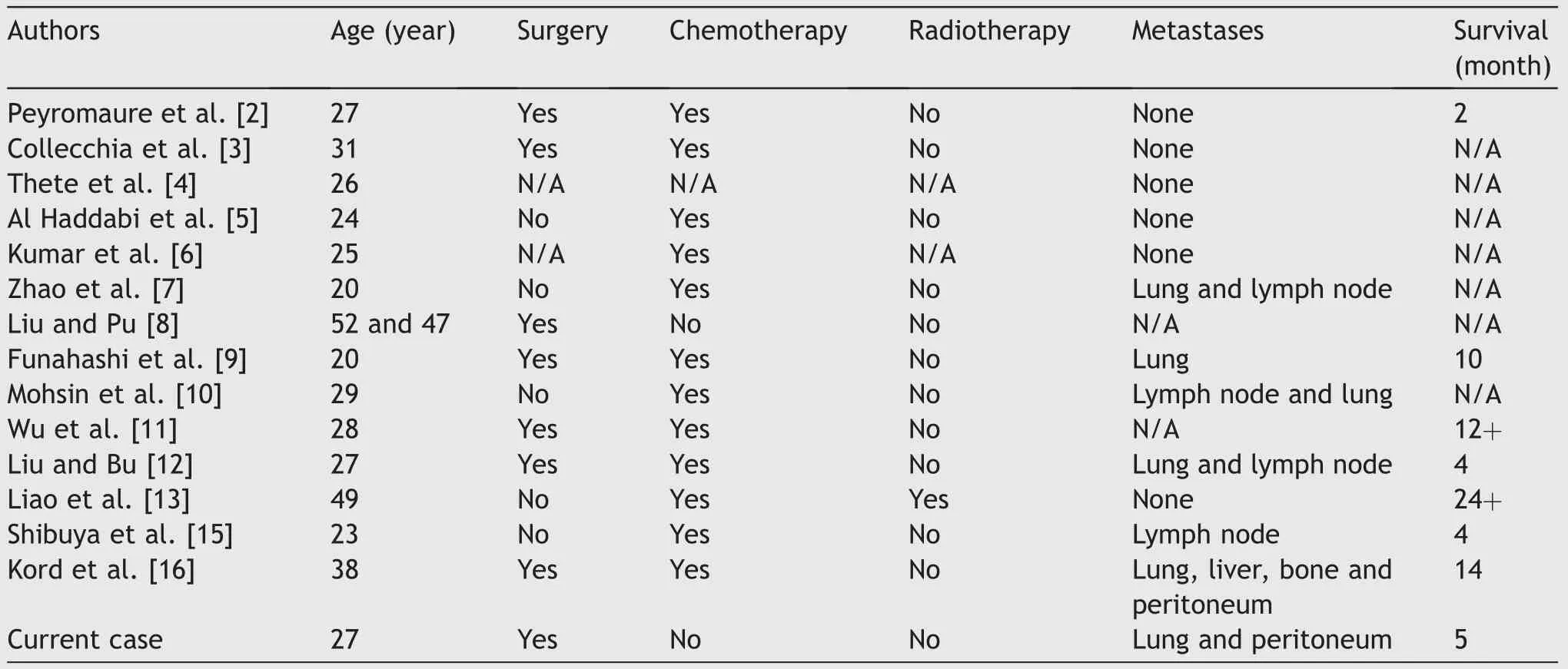
Table 1 Clinical characteristics of reported primitive neuroectodermal tumor of prostate cases.
4. Conclusion
Although PNET of prostate is extremely rare, to early establish diagnosis of PNET of prostate,urologic oncologists should pay much more attention to the young male patients with above mentioned clinical features. To minimize the harm of the disease,radical surgery should perform as early as possible in localized PNET of prostate, and combined therapy would be helpful to improve efficacy of treatment.
Author contributions
Study design: Lichen Teng.
Contribution to the surgery: Li Li.
Data acquisition: Liangjun Wei, Yongpeng Xu.
Data analysis: Yongsheng Chen, Yan Cao.
Drafting of manuscript: Lichen Teng, Changfu Li.
Critical revision of the manuscript: Wentao Wang.
Conflicts of interest
The authors declare no conflict of interest.
Acknowledgement
This study was partly supported by Natural Scientific Research Project (H2018048) of Heilongjiang province Science and Technology Department, and it was partly supported by the China Scholarship Council.
 Asian Journal of Urology2020年2期
Asian Journal of Urology2020年2期
- Asian Journal of Urology的其它文章
- Robot-assisted laparoscopic prostatectomy:How can we get better?
- Management of staghorn stones in special situations
- Preoperative imaging in staghorn calculi,planning and decision making in management of staghorn calculi
- Staghorn calculi: Understanding the paradigm shift in management
- Carcinoma bladder and sliding bladder hernia: Unusual association of paramount significance
- A prospective study of patient reported urinary incontinence among American,Norwegian and Spanish men 1 year after prostatectomy