
Pharmacoeconomic Evaluation of Rituximab(Hanlikang)for Patients with Rheumatoid Arthritis
2020-03-23 05:33:28WangYanqiChenBinbinZhaoMengmengSunLihua
Wang Yanqi,Chen Binbin,Zhao Mengmeng,Sun Lihua
(1.School of Business Administration,Shenyang Pharmaceutical University,Shenyang 110016,China;2.Beijing Medical and Health Economic Research Association,Beijing 100069,China)
Abstract Objective To provide reference for clinical medication and drug policy formulation for patients with rheumatoid arthritis.Methods A Markov model was established for patients with moderate and severe rheumatoid arthritis.The model period was 6 months and the simulation time was the average life expectancy of Chinese residents(76 years).The cost-utility analysis method was used to analyze the effect of Hanlikang combined with methotrexate and Yisaipu combined with methotrexate from the perspective of the whole society.The economy of Hanlikang was evaluated and the robustness of the results was verified by sensitivity analysis.Results and Conclusion For the patients with moderate and severe rheumatoid arthritis,compared with Yisaipu,Hanlikang could save 69 228 yuan and gain 0.837 quality adjusted of life years(QALYs)in the whole life cycle with great economic advantages.The results of sensitivity analysis were consistent with those of basic analysis,and the results of probability sensitivity analysis showed that when the willingness to pay was the per capita GDP(64 644 yuan),the economic probability of Hanlikang group reached 79.3%.
Keywords:Rituximab;rheumatoid arthritis;pharmacoeconomic evaluation
1 Introduction
Rheumatoid arthritis(RA)is a systemic autoimmune disease characterized by erosive arthritis.Epidemiological surveys showed that[1],the prevalence rate in mainland China was 0.42%.The total number of patients was nearly 5 million,and the prevalence rate of men and women was about 1:4[1-2].RA not only caused the decline of patients' physical function,quality of life and social participation,but also brought a huge economic burden to patients' families and society[3-5].Clinical studies showed that[6]Rituximab was effective in the treatment of RA,but its original drug price was relatively expensive(10 mL:0.1 g/tube,2 294.44 yuan).In addition,pharmacoeconomic studies showed that[7]Rituximab was uneconomic with the incremental cost-effectiveness ratio(ICER)value of more than 3 times of China's per capita GDP,compared with the traditional disease modifying anti-rheumatic drugs(DMARDs).In February 2019,Hanlikang,the biological generic of Rituximab,was put on the market of China.Compared with its original drug,its efficacy was not significantly different and its price was lower(10 mL:0.1 g/dose,1 648 yuan).Up to now,there is no study evaluating rheumatoid arthritis for its economy.On this basis,Markov model was used to analyze the long-term economy of Hanlikang for the aim of providing reference for the clinical drug usage and policy making.In view of the fact that Yisaipu is a commonly used biological agent for the treatment of moderate or severe RA patients and has been listed in the national medical insurance drug catalog,Yisaipu was selected as the control drug in this study.
2 Model structure
According to the disease activity of index,RA patients could be divided into four states,including remission,low disease activity,medium disease activity and high disease activity.Generally,disease activity score with 28 joint counts(DAS28)is the commonly used criteria[5].The treatment goal of RA is to achieve clinical remission(DAS28≤2.6)or low disease activity state(DAS28≤3.2).In order to simulate the disease progression of RA,a Markov model with three health states was constructed in this study,namely,moderate high disease activity(MHDA),low disease activity or clinical remission(LDA-CR)and death.The model structure is shown in Fig.1.
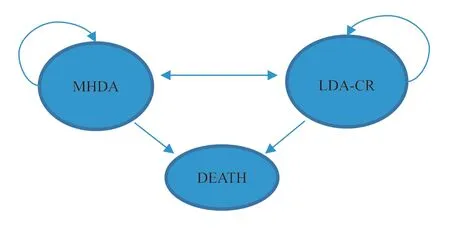
Fig.1 Markov model structure
According to the guideline[1],when the treatment of single traditional synthetic DMARDs is not up to the standard,another one or two traditional synthetic DMARDs is suggested to be combined for the treatment or a biological agent should be combined with a targeted synthetic DMARDs.As shown in Fig.1,when the patient was in MHDA state,he would be treated by Hanlikang combined with methotrexate or Yisaipu combined with methotrexat.After 6 months' treatment,the curative eff ect could be evaluated.If the treatment could reach the standard,only methotrexate would be used for maintenance treatment.Otherwise,another biological agent DMARDs would be used.According to the actual clinical medication of RA,biological DMARDs usually were one of the following three:infliximab,adamummab and tocilizumab.The curative eff ect was evaluated again after 6 months.On the other hand,when the patient entered the LDA-CR state,he could continue to maintain this state or relapse to the MHDA state or enter the death state.When the patient entered the death state,the metastasis could not continue to occur.In addition,due to the long simulation time,this study assumed that all the patients in the study had received the biological agent DMARDs,that is,they had received all the treatment of infliximab,tocilizumab and adalimumab.
The cycle length of this model was set as 6 months and the simulation time was the average life expectancy(76 years).The population baseline data of Markov model included mean age of disease(45 years),mean weight(58 kg),DAS28 score(5.42)and health assessment questionnaire(HAQ)score(1.9),which was widely used to ref lect the impact of arthritis on patients' ability of daily life.The data was from the clinical trial of Hanlikang.The starting queue of the model was assumed to be 1 000 patients.
Considering the time value,this study used the current social discount rate of 8%.
3 Transition probabilities
For the transition probabilities of the f irst cycle,the Hanlikang group came from the efficacy data of its clinical trials.There was no reliable randomized controlled trial about Yisaipu,but some studies showed that Yisaipu was highly similar to Etanercept in key quality characteristics by comparing the two products and they were the same type[7].Therefore,the effi cacy data of Etanercept's randomized controlled trial was used instead[8].Starting from the second cycle,the transition probability from MHDA state to LDA-CR state in the two groups came from the real study on the use of DMARDs for 802 RA patients in 15 hospitals in different regions of China[9].
Regarding the transition probability from LDA-CR status to MHDA status,the Hanlikang group received follow-up data of 194 RA patients using biological DMARDs from 2003 to 2013[10].After stopping TNF-αantagonist,the data of 531 RA patients in LDA-CR status who had relapsed to MHDA state was used in Yisaipu group[11].The transition probability from LDA-CR status to death status was the age-specific mortality rate of Chinese population in 2016.And that from MHDA status to death status was calculated based on the HAQ score of patients' baseline characteristics relative to the death risk of the general population(1.33/HAQ)[12].All transition probabilities were adjusted to the period length.
4 Cost data
From the perspective of the whole society,cost data should include direct costs(direct medical costs,direct non-medical costs),indirect costs and implicit costs that are difficult to calculate with money.In view of the availability of data,direct medical costs(drug costs,other direct medical costs)and indirect costs caused by labor losses were studied in this paper.
4.1 Drug costs
The drug price data were the average bid price of each drug in 2019.According to the proportion of Infliximab,Adalimumab and Tocilizumab used by patients with RA[9],the cost of them was calculated as the weighted average value.Drug costs were shown in Table 1.
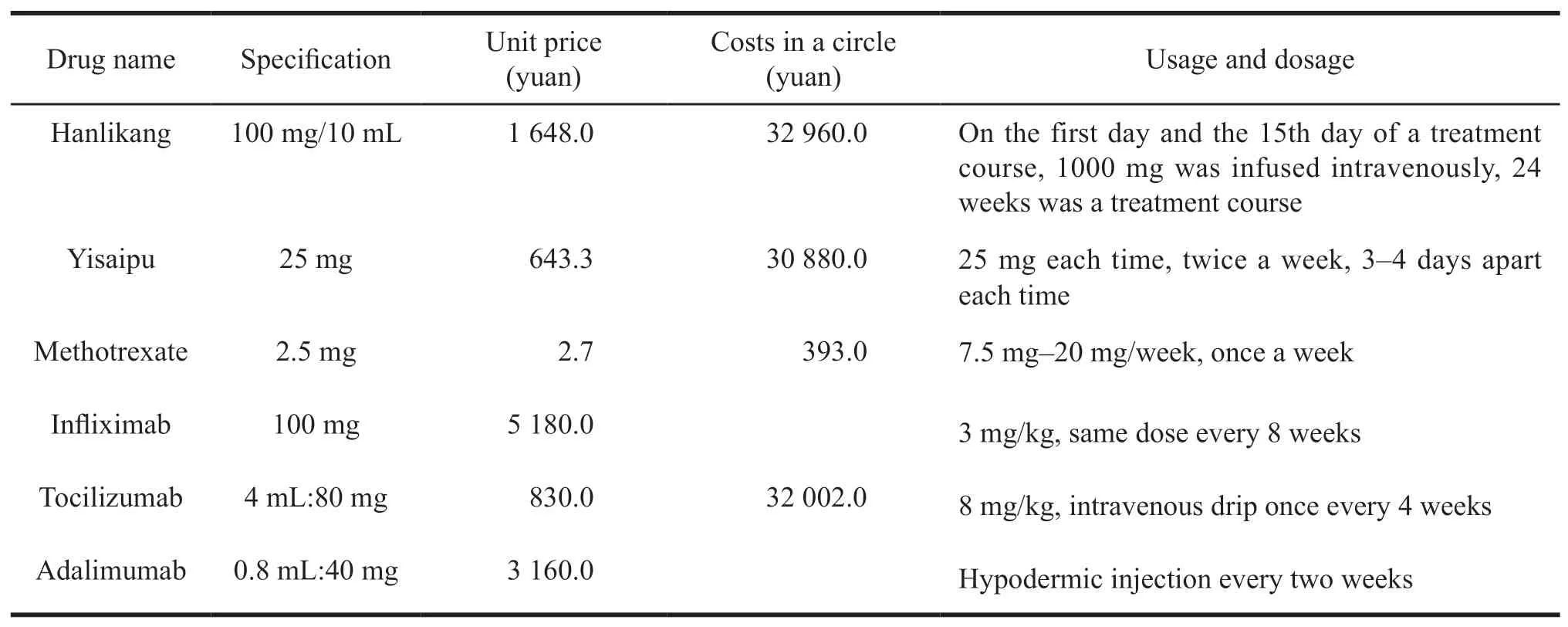
Table 1 Drug costs
4.2 Other direct medical costs
In addition to the drug cost,other direct medical costs incurred by RA patients due to hospitalization and outpatient service,such as registration fees and inspection fees,etc.In this study,other direct medical costs of MHDA status(using biological DMARDs)and LDA-CR Status(without using biological DMARDs)were calculated based on the data of systematic random sampling of RA patients in 12 cities of Beijing,Tianjin,Shanghai,Chongqing,Jinan,Nanjing,Xiamen,Xi'an,Wuhan,Chengdu,Shenyang and Lanzhou in 2017.The results were displayed in Table 2.
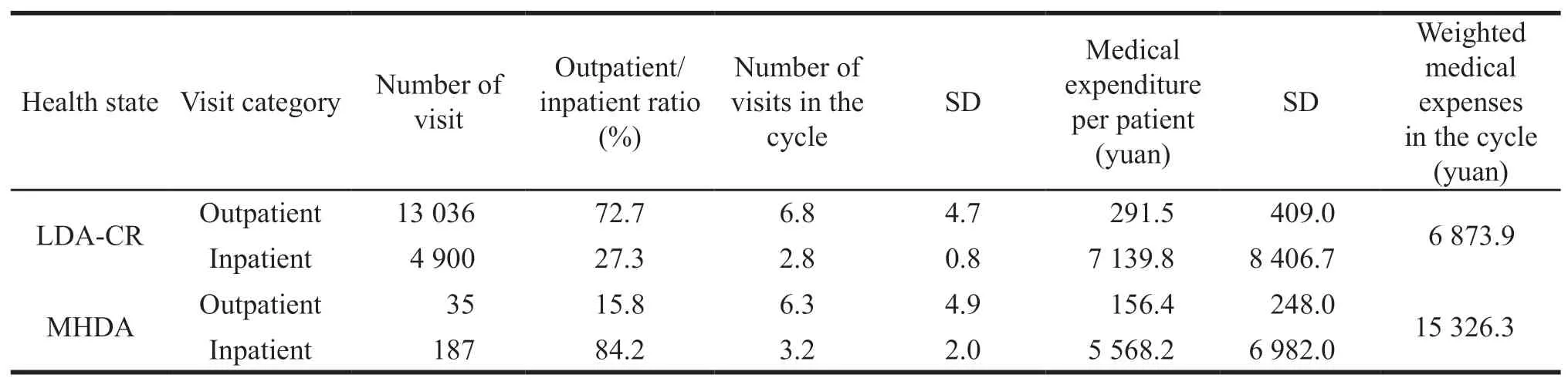
Table 2 Other direct medical costs
4.3 Indirect cost
A retrospective survey showed that 18.8% of RA patients with MHDA status met the disability identification standard[13].Therefore,the cost of labor loss caused by patients' disability with MHDA status was calculated by the average daily wage of urban employees in 2017[14]times the days of disability.Based on the above data,the cost of labor loss caused by disability in a circle was 35 036.4 yuan.
The model assumed that patients in LDA-CR state had no severe functional limitations or no labor loss due to disability.
5 Utility data
In this study,quality adjusted of life years(QALYs)was used as the utility index.The utility value of RA patients was related to their HAQ scores[15].When the HAQ scores were mapped to EQ-5D,the utility values corresponding to different HAQ scores were obtained.When the RA patients were in LDACR state,HAQ score was less than 0.5,and utility value was 0.770.When patients were in MHDA state,HAQ score was 1.9 and utility value was 0.488.But in death state,utility value was 0.
6 Basic analysis
Cost-utility analysis results were showed in Table 3.Compared with Yisaipu,Hanlikang had economic advantages,saving 69 228.4 yuan in cost and getting as much as 0.837 QALYs.

Table 3 Cost-utility analysis results
7 Sensitivity analysis
7.1 Single factor sensitivity analysis
To understand the stability of the research results,the prices for Hanlikang and Yisaipu,the transition probabilities between different states,the utility value of MHDA and LDA-CR state patients,the number of outpatient and inpatient visits,the proportion of patients with disability due to RA and the discount rate were analyzed.The results were shown in Fig.2.It can be seen from Fig.2 that the utility value of LDACR and MHDA states,the number of hospitalizations,discount rate,the proportion of patients with disability due to RA,and the probability of MHDA state transferring to death state had a great influence on the ICER.However,when the factors changed within the adjustment range,the ICER value was also less than the per capita GDP(64 644 yuan),which was consistent with the result of cost utility analysis.The results of single factor sensitivity analysis were displayed in Fig.2.
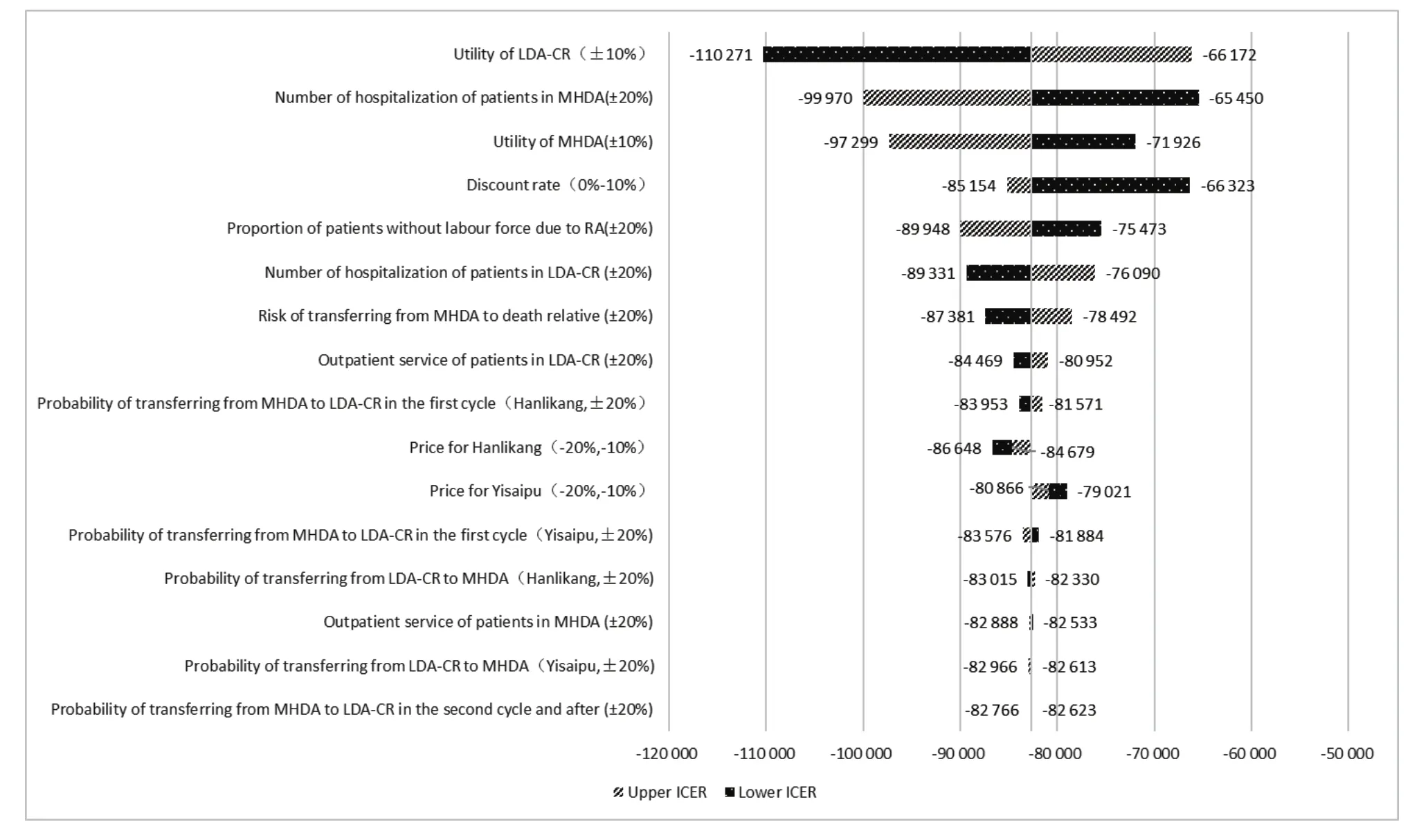
Fig.2 Single factor sensitivity analysis results
7.2 Probability sensitivity analysis
The probability sensitivity of cost data,transition probability data and utility data were mainly analyzed in this study.According to the Monte Carlo simulation,10 000 times of repeated sampling,ICER probability distribution scatter diagram and cost-utility acceptable curve were obtained and were shown in Fig.3 and Fig.4.
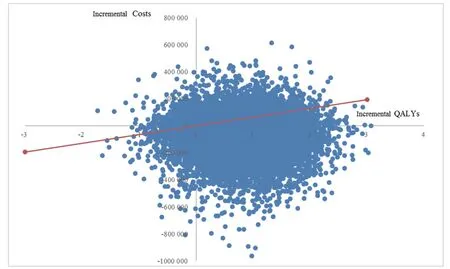
Fig.3 ICER probability distribution scatter diagram
World Health Organization recommends that when ICER<GDP per capita,the increased cost is fully worth it.When per capita GDP<ICER<3 times GDP per capita,the increased cost is acceptable.When ICER>3 times GDP per capita,the increased cost is not worth it[16].It can be concluded from Fig.4 that when the willingness to pay was 1 times of GDP per capita(64 644 yuan),the economic probability of Hanlikang group was 79.3%.
8 Scenario analysis
As the quality of life of RA patients is generally lower than that of healthy people[17]and some studies showed that[18]complications for RA inpatients were as high as 84.71%,which could affect the survival time of patients.Therefore,this study adjusted the simulation time limit to 10 years and 20 years for scenario analysis.
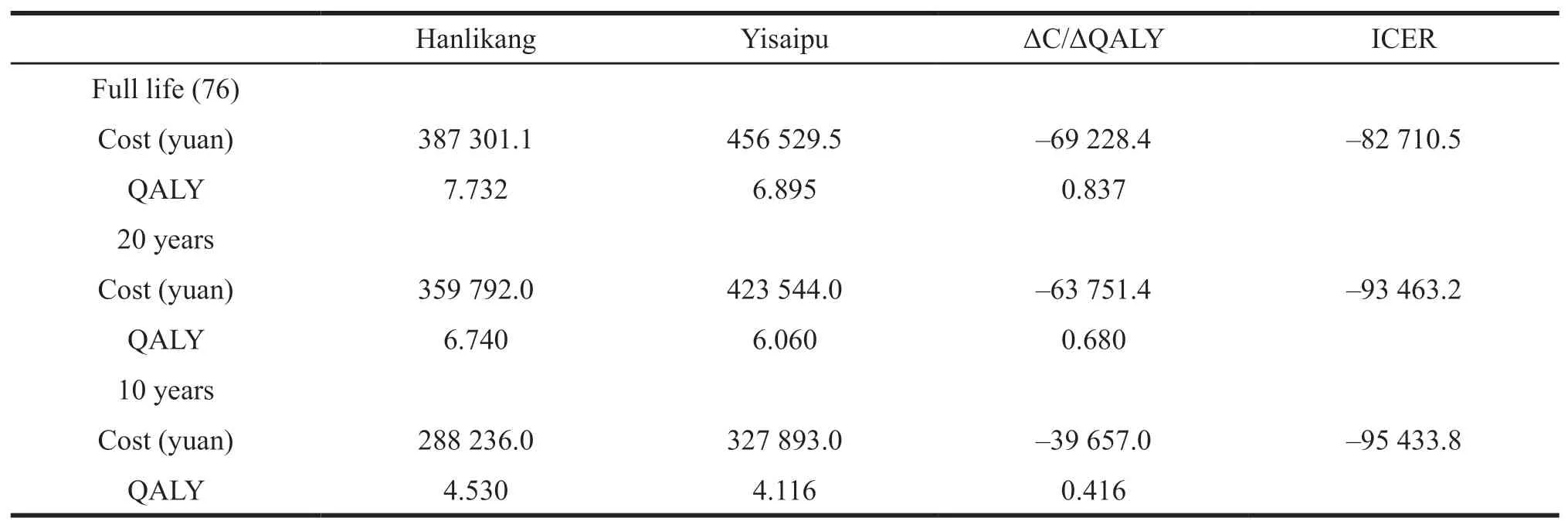
Table 4 Scenario analysis results
It can be summarized from Table 4 that when the simulation time limit was adjusted to 10 or 20 years,Hanlikang was still economical.
9 Conclusions and discussions
The results of cost-utility analysis showed that Hanlikang had economic advantage over Yisaipu.In the uncertainty analysis,the results of single factor sensitivity analysis demonstrated that the utility value of LDA-CR and MHDA states,the number of hospitalizations,discount rate,the proportion of patients with disability due to RA and the probability of MHDA state transferring to death state had great influence on ICER.But when the factors changed within the adjustment range,ICER values were always less than per capita GDP in 2018.The result of sensitivity analysis showed that when the willingness to pay was as much as GDP per capita,the economic probability of Hanlikang was 68.3%.
There are some problems in this study.First of all,it is suggested in the guidelines for the diagnosis and treatment of RA that patients who cannot use Methotrexate should adopt other traditional synthetic DMARDs,such as Leflunomide or Sulfasalazine.But this study only considered the common situation that patients can use Methotrexate.In addition,the model only considered the direct medical cost.The direct non-medical cost,such as the transportation cost and accommodation cost incurred due to medical treatment,was not included in the model.In the future,relevant research can be carried out to obtain more detailed data to reduce the impact of the above bias on the research results.
 Asian Journal of Pharmacentical Sciences2020年1期
Asian Journal of Pharmacentical Sciences2020年1期
- Asian Journal of Pharmacentical Sciences的其它文章
- Information for Authors
- The Analysis of Marketing Strategy of Plendil
- Comparative Study on the Development of Urban Basic Medical Insurance in 14 Cities of Liaoning Province
- Research on the Transformation of Mapping Method for Cancer Patients' Health Utility in the Asia-Pacific Region
- Application Research of Earned Value Management in New Drug Research and Development Projects
- Compulsory Licensing of Pharmaceutical Patents System from the Perspective of Public Interest-Public Health in China