
Narrative nursing for cancer patients: a meta-analysis
2019-12-09 09:05:32MinZhangYingMingSunNaSunYaNanLeng
Cancer Advances 2019年4期
Min Zhang, Ying-Ming Sun, Na Sun, Ya-Nan Leng,*,
Narrative nursing for cancer patients: a meta-analysis
Min Zhang1, Ying-Ming Sun1, Na Sun1, Ya-Nan Leng1,*,
1Graduate School, Tianjin University of Traditional Chinese Medicine, Tianjin 301617, China.
To systematically review the effect of narrative nursing for cancer patients.Systematic searches in PubMed, EMBASE, The Cochrane Library, Web of Science, Chinese biomedical literature database, China National Knowledge Infrastructure, Wanfang medical and VIP database were performed for randomized controlled trials (RCTs) or quasi-RCTs which explored the effects of narrative nursing mode for cancer patients. Then, meta-analysis was performed by RevMan 5.3 after two independent investigators screened the literature, extracted the data and evaluated the risk of bias of all included studies.A total of 15 studies were included, including 1778 cancer patients. The meta-analysis showed that narrative nursing could effectively relieve patients' anxiety and depression compared with the conventional nursing model (WMD = -9.04, 95% CI = -11.82, -6.27;< 0.001), reduce the the inner shame(WMD = -2.28, 95% CI = -3.76, -0.88;= 0.001), improved the mental resilience (WMD = 18.20, 95% CI = 3.30, 33.11;< 0.001) and the quality of life.This study has been systematically evaluated to show that narrative care can effectively improve the negative mood of patients with cancer and improve their quality of life. However, subject to the quality limitations of the included studies, the appeal conclusions are yet to be tested in more high-quality studies.received traditional nursing and routine care. Including life nursing: like bed making unit; Medication nursing: like liquid infusion speed and Time and effect of oral medicine; Symptomatic nursing: like pain nursing; Special nursing during radiotherapy and chemotherapy; Side effects of treatment nursing, such as nausea, vomiting; Psychological nursing: comfort patients.
Narrative, Nursing, Cancer, Anxiety, Depression, Quality of life
Introduction
The number of new cases of cancer in China has reached 4.29 million each year, accounting for 20% of the world, among which the annual death toll is as high as 2.81 million [1]. As a significant adverse stress event, cancer has a severe impact on patients' health. Because of the uncertainty of the therapeutic effects and adverse effects of radiotherapy and chemotherapy, heavy economic burden, and imperfect social support system, Cancer poses excellent challenges for patients [2, 3]. Researches have shown that cancer patients who receive treatment may suffer severe mental distress like depression, anxiety. Thus, this leads the patients' challenging to adjust to daily life [4]. Many studies have indicated that one-third of cancer patients suffer from negative emotions such as depression and anxiety. Patients may generate the shame of disease especially like prostate, breast cancer, and stoma patients. The social support is an influential factor in cancer patients. The patients obtained low levels of social support during cancer treatment would encounter more mental problems than those who obtained high levels of social support [5-7].
With the continuous improvement and development of modern medicine, the concept of holistic nursing has gradually emerged. Adhering to the return of humanities is the only way to achieve overall care. Narrative nursing, as a way of humanistic care, has steadily attracted the attention of the nursing community [8]. Narrative care refers to the humanistic care, respect, listening, and empathy of narrative medicine. It combines a sequential treatment model and methods in postmodern psychology with clinical nursing [9]. The core concepts of narrative care include 5 points: 1. People are not equal to diseases, and diseases are diseases. 2. Everyone is an expert in their diseases. 3. Everyone has resources and abilities. 4. Everyone is the author of his own life. 5. Disease does not mean 100% manipulator [10]. In recent years, scholars' research on narrative care has gradually shifted from the level of concern to the level of intervention. A recent data analysis in China shows that narrative care is gradually used in the care of cancer patients [11]. This paper conducts a meta-analysis of narrative nursing for cancer patients.
Methods
Inclusion and exclusion criteria
Study Design: Randomized controlled trials (RCTs) or quasi-RCTs were included.
Subjects: Patients were diagnosed with malignant tumors based on clinical diagnosis and laboratory examination.
Interventions
Narrative nursing group: Through listening to and understanding patients' stories, combined with patients' conditions and medical conditions and abilities. Nurses can help patients to reconstruction the meaning of life. Finding out the patients' demands and nursing points according to patients' stories, then improving nursing intervention for patients.
Outcome
The self-rating anxiety scale was used to measure the degree of anxiety and self-rating depression scale or hamilton depression scale or the edmonton symptom assessment scale.
The social impact scale was adopted to measure the level of patients’ inner shame.
The resilience scale-14 was used to measure the capacity of inner shame.
SF-36 or the functional assessment of cancer therapy-generi was used to measure the quality of life.
Exclusion criteria
Non-Chinese and English literature. Duplicated literature. Lack of relevant research background and data literature.
Literature search
Systematic searches in PubMed, EMBASE, The Cochrane Library, Web of Science, Chinese biomedical literature database (CBM), China National Knowledge Infrastructure (CNKI), Wanfang medical database and VIP database were performed for identifying randomized controlled trials (RCTs) or quasi-RCTs which explored the effects the narrative nursing were applied to patients diagnosed with cancer. In this paper, medical subject headings and free words were combined to search for studies. They were as follow: (narration (MeSH) OR narrations (Title/Abstract) OR narrative therapy (Title/Abstract) OR narrative nursing (Title/Abstract) OR narrative medical (Title/Abstract) OR close reading (Title/Abstract) OR reflective writing) AND (neoplasms (MeSH) OR neoplasia* (Title/Abstract) OR neoplasm* (Title/Abstract) OR tumor* (Title/Abstract) OR cancer* (Title/Abstract) OR malignancy (Title/Abstract) OR malignancies (Title/Abstract) OR malignant neoplasm* (Title/Abstract) OR benign neoplasm* (Title/Abstract) OR) AND (nursing (MeSH) OR nursing (Title/Abstract) OR nur*).
Literature screening and data extraction
All eligible articles were imported into the NoteExpress Literature management software for first time repeated screening. The two researchers respectively screened the records and extracted the data. Any disagreement during this process was resolved by discussion or consulting with the third reviewer. The obtained data included: (1) necessary information of records including the title, the first author, time of publication, national, the type of study, (2) sample size, (3) baseline level of subjects, (4) intervention, and outcome, (5) bias of the included literature.
Assessment of risk of bias
According to the Cochrane Handbook for systematic review of interventions 5.1.0 [12], the risk of bias in all included records was assessed by two researchers independently. The seven items recommended by Cochrane Handbook are as follows: adequacy of the generation of the allocation sequence, concealment of allocation, blinding participants and personnel, blinding outcome assessment, incomplete outcome data, selective outcome reporting, and other sources of bias.
Statistical analysis
Meta-analysis was performed by RevMan 5.3 software. The risk ratio (RR) was used as the effect statistics for the dichotomous variable. The weight mean difference (WMD) was used as the effect statistics for the continuous variable. The effect size and 95% confidence interval (CI) were given. The heterogeneity between the included studies was tested by the χ2test orIstatistic. If there was no statistical heterogeneity across the studies, the fixed-effect model was used. If there was heterogeneity across studies, a random-effect model was used. If clinical heterogeneity was significant, subgroup analysis, sensitivity analysis, or a descriptive analysis was used.
Results
Literature screening process and results
Three hundred forty-five articles were collected after the initial literature search. Finally, 15 articles were included, with a total of 1778 eligible patients [12-27]. The literature screening and process are shown in Figure 1.
The basic characteristics of the included studies
This study extracted correlative characteristics of the included studies, as shown below: the first author, publication date, and country, Types of trail, sample size, age, intervention approach, and outcome indicators.
Bias risk assessment results of the included studies
The 15 included studies were reported the baseline level of subjects, and 7 literatures have introduced the generation of random sequences [14, 16, 17, 19-23, 25, 26]. The risk and detail of bias in the literature is shown in Figure 2.
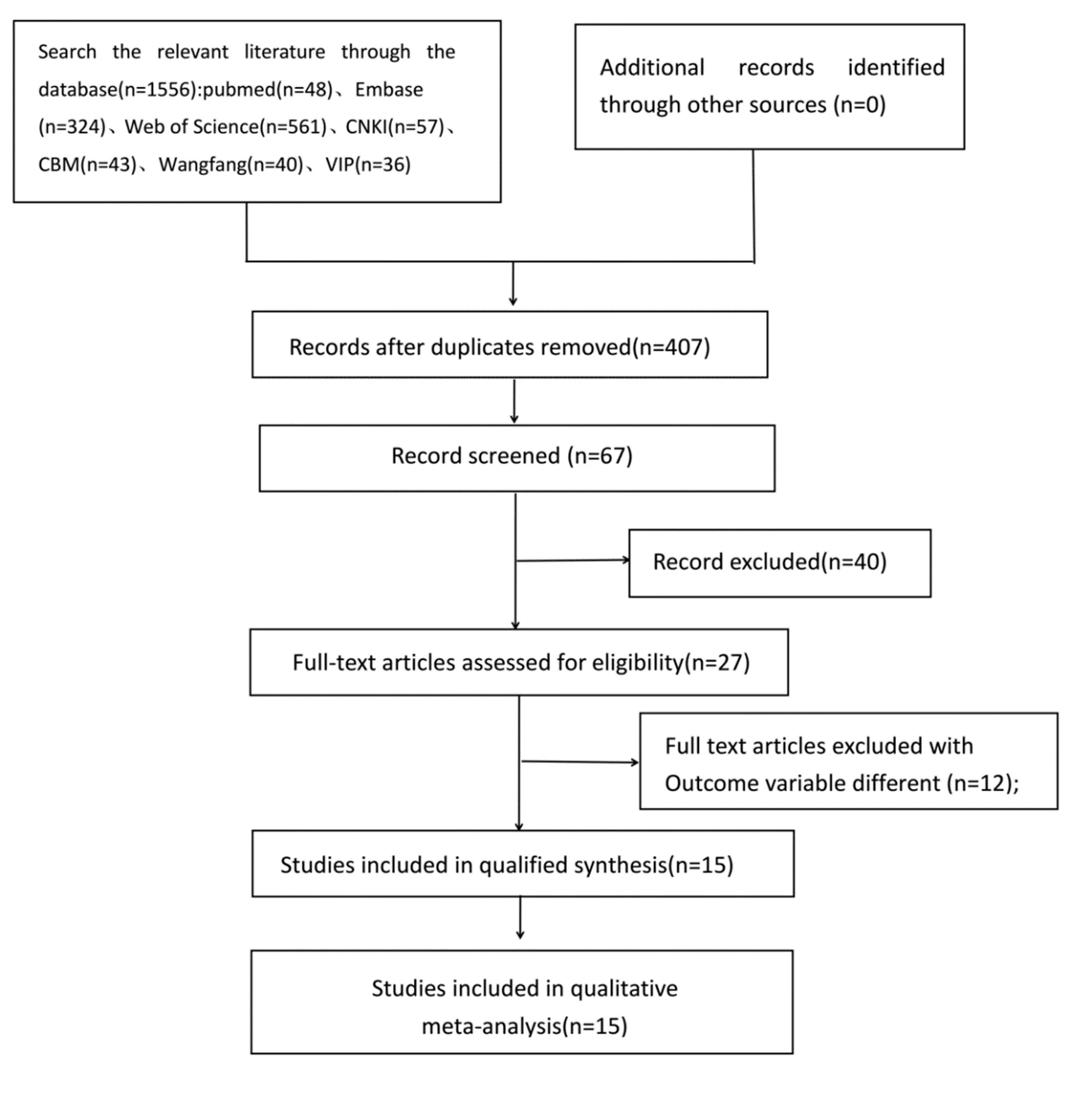
Figure 1 Flow diagram of included and excluded studies
Analysis Result
The degree of anxiety and depression
A total of 8 studies with 712 in the narrative nursing group and 691 in the control group reported outcomes about the anxiety and depression [13-15, 17, 20, 12-24]. The meta-analysis of the random model showed that the degree of anxiety and depression of the patients with cancer in the narrative nursing group was lower than that in control group, and the difference was statistically significant (WMD = -9.04, 95% CI = -11.82, -6.27;< 0.001).
The meta-analysis of the random model showed the degree of anxiety of the patients with cancer in the narrative nursing group was lower than that in the control group, and the difference was statistically significant (WMD = -11.94, 95% CI = -16.33, -7.55;< 0.001).
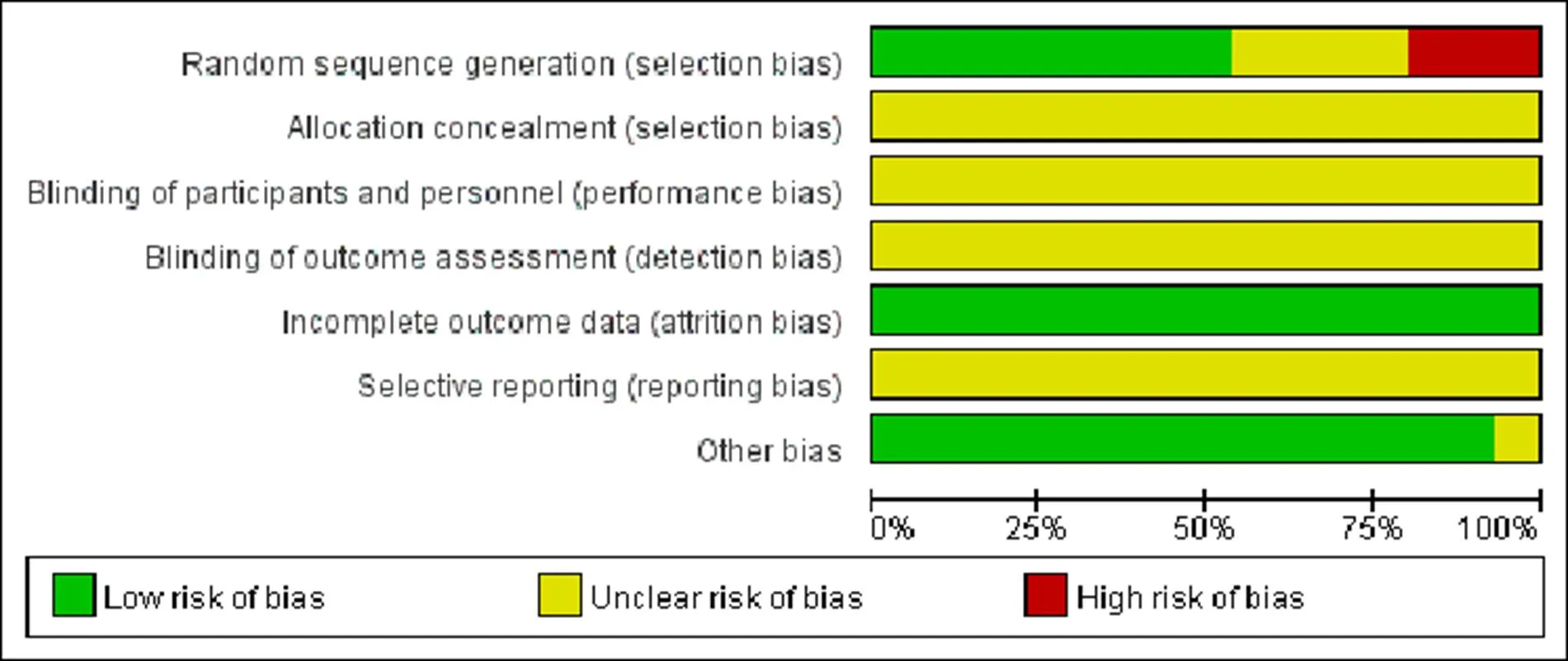
Figure 2 Risk of bias graph
The meta-analysis of the random model showed the degree of depression of the patients with cancer in the narrative nursing group was lower than that in the control group, and the difference was statistically significant (WMD = -5.72, 95% CI = -8.86, -2.58;< 0.001). The result was shown in Figure 3.
Descriptive analysis of the degree of depression: three studies have adopted other scales to measure the degree of patients’ degree, such as Li, Williams, and Wise [25-27]. They used different tools, so a descriptive analysis of these three studies was provided. All three studies showed that narrative therapy was more effective in relieving patients' anxiety compared with the control group, and the difference was statistically significant (< 0.05).
The capacity of mental resilience
A total of 2 studies with 61 in the narrative nursing group and 61 in the control group reported the outcome of mental resilience [16, 18]. The meta-analysis of the random model showed the capacity of resilience of the patients with cancer in the narrative nursing group was higher than that in the control group, and the difference was statistically significant (WMD = 18.20, 95% CI = 3.30, 33.11;< 0.001). The result is shown in Figure 4.
The level of inner shame
Two studies with 288 in the narrative nursing group and 290 in the control group reported the outcome of inner shame [19, 21]. The meta-analysis of the random model showed the level of the inner shame of the patients who with cancer in the narrative nursing group was lower than that in the control group, and the difference was statistically significant (WMD = -2.28, 95% CI = -3.76, -0.88;= 0.001). The meta-analysis of the random model showed the level of the inner shame of the patients with cancer in the narrative nursing group after one and six months was fewer than that in the control group, but the difference was not statistically significant. (WMDone month= 1.45, 95% CI = -4.58, 1.69;= 0.37), (WMDsix month= -3.09, 95% CI = -7.11, -0.93;0.13). But at after three month and the difference was statistically significant (WMDthree month= -2.25, 95% CI = -3.71, 0.80;= 0.002). The result was shown in Figure 5.

Figure 4 Forest plot shows the effect of narrative nursing on the capacity of patients’ mental resilience
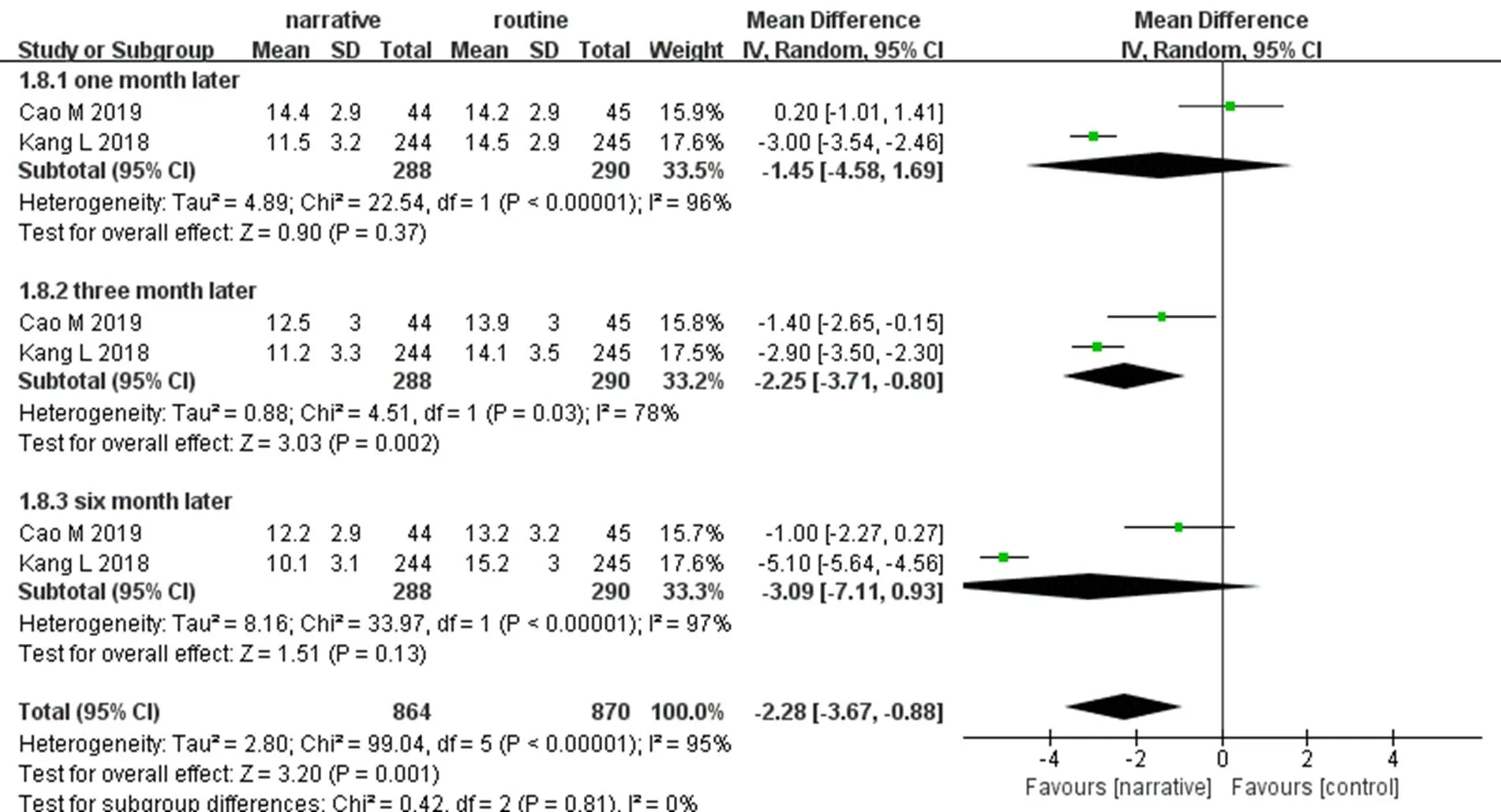
Figure 5 Forest plot shows the effect of narrative nursing on the level of patients’ inner shame
The quality of life
A total of 3 studies with 57 in the narrative nursing group and 163 in the control group reported the quality of life [15, 21, 25]. Ma and Jiang adopted the SF-36 scale to measure the level of the quality of life, but they used different calculate way. Li adopted the functional assessment of cancer therapy-generi scale to measure. Therefore, Descriptive analysis was conducted for the outcome indicator of quality of life. All studies showed that compared with the control group, narrative nursing could improve the quality of life of patients better, and the results were statistically significant (< 0.05).
Discussion
The leading cause of death in malignant tumors in China is lung cancer, followed by liver cancer, gastric cancer, esophageal cancer, and colorectal cancer, and the top five cancers of cancer deaths are not high in 5 years [28]. Most cancer patients have to undergo radiotherapy, chemotherapy, and surgery, which are painful and expensive to treat, as well as a series of side effects. Once a patient is diagnosed with any cancer, they face many physical, psychological, and social problems, struggle to adapt to life after the disease, and lose hope for the future [29]. What cancer patients want most is the care of family and friends and effectively help and care form medical staff. Encouraging patients to speak up and listen to their concerns is an integral part of cancer treatment.
With the change of nursing concept and the approached of humanistic nursing, paying full attention to the physiological, psychological and social of patients has been a primary task of nursing. In 2001, Professor Charon put forward the concept of narrative medicine and defined it as a medical humanity. Doctors can comfort patients by applying narrative therapy such as close reading and reflective writing [30, 31]. Narrative nursing originates from narrative medicine. It requires nurses to listen to patients' stories actively and carefully, Help patients regain confidence in life, and improve mental resilience. Discover nursing points and provide personalized care to patients [32]. Narrative nursing usually follows the following process: (1) get the patient's trust and recognition; (2) make a chronological nursing plan; (3) externalization of internal problems: let patients tell their own inner stories and confusion; (4) deconstruction of stories: Let patients recall past experiences and difficulties, find common conditions and methods to solve problems; (5) rewrite: according to patients. The story and inner fear develop appropriate nursing measures, improve resilience, help patients adapt to their current lives [33]. Numerous studies have shown that narrative care does play an active role in relieving psychological stress, reducing mental burden and improving patients' psychological endurance. Studies have shown that narrative nursing does play an active role in relieving psychological stress, reducing mental burden and improving subjective tolerance of patients [33].
Most cancer patients receive treatments, such as radiotherapy and chemotherapy. Due to the pain of the disease itself, the side effects of treatment, and the high cost of treatment, it has a severe impact on the physical and psychological aspects of the patient, and the patient is prone to anxiety, depression,[24]. Mental resilience is closely related to patients' ability to adapt to emergencies [34]. When patients encounter high external stress, their mental resilience will decline. The hope and attitude towards life will be converted into a negative status [35]. Clinical nurses adopted narrative nursing, actively encourage patients to tell their own stories, listen carefully and objectively ask patients about the psychological problems, understand the real state of the patient's inner, and analyze the problem. According to the actual situation of the patient, Nurses use targeted measures, such as lectures, psychological counseling family interaction, and celebration,, to relieve the patient's inner anxiety and depression, and help them face to live actively.
Patients with breast and colorectal cancer may develop internal shame because of changes in their structure. Changes in body structure will lead to anxiety, depression, low self-esteem, and shame in stomatology patients [36]. On the social aspect, cancer patients are less likely to participate in social entertainment activities and are reluctant to engage with relatives and friends. At the same time, the marital problems of cancer patients have also increased, and the disease will affect patients and their sexual life [37]. This study showed that in the early stage, the change of inner shame in the narrative group was not statistically significant compared with the control group. As time went on, the effect of narrative care gradually appeared. However, after the patient returns to the family and society, the level of shame slowly recovers, indicating that the change of inner shame is a dynamic and long-term process. The excellent effect of narrative care of hospital cannot be extended to the family and the community. It can be seen that the narrative ability is not the patent of the frontline medical staff. If we want to improve the psychological burden of cancer patients for a long time, we need families and communities to cultivate narrative skills to provide a pleasant living environment for cancer patients.
The WHO defines the quality of life as the experience of individuals in different cultures and value systems of their living conditions related to their goals, expectations, standards, and concerns [38]. Quality of life of cancer patients is a health concept that comprehensively evaluates the quality and quantity of various factors such as physical function, psychological, social, economic, emotional, disease itself and symptoms and signs caused by treatment of cancer patients [9], which was considered to be the endpoint of clinical therapy. Therefore, how to help patients, calmly face the change of physical structure and alleviate bad emotions are the main aspects to improve the quality of life of cancer patients. Narrative nursing by relieving patients' nervous and anxious feelings, improving psychological resilience and reducing the shame of the disease can improve the quality of life of patients.
However, there still some limitations to this study.The quality of the literature included in this study is not high. Some studies did not adopt the correct random method and did not report the distribution principle and blind mode, which would lead to selective bias. All articles included in this article are publicly available, unpublished literature is not searched, and there may be publication bias; due to inconsistencies in the measurement tools included in the research, the data types or calculation methods involved are inconsistent and can only be descriptively analyzed.
Conclusion
Narrative nursing is a kind of method that may improve the ability of humanistic nursing. By listening to and responding to the patient's story, the medical staff can make the patient feel the concern of the outside world. At the same time, the patient’s real complaints about internal confusion can alleviate the inner pressure and find a solution to the problem. At present, historical nursing clinical development in foreign countries is relatively perfect. Some hospitals are equipped with a dedicated narrative care practice team [11]. However, the narrative ability of clinical nurses still needs to be improved, and the staff and fund allocation of the department have yet to be developed. Therefore, in the future development of hospitals, it is necessary to actively organize nurses to learn narrative-related knowledge and improve departmental resource allocation. At the same time, narrative therapy not only limited in medical staff, which would be more accessible, covers all aspects form hospital to family. To relieve the adverse emotional and psychological burden of patients, improve the quality of life of cancer patients.
1. 2017 China's latest cancer data. Chin J Clin Oncol Rehabil 2017, 24: 760.
2. Cordova MJ, Cunningham LL, Carlson CR,. Posttraumatic growth following breast cancer: a controlled comparison study. Health Psychol 2001, 20: 176-185.
3. Pinquart M, Duberstein PR. Depression and cancer mortality: a meta analysis. Psychol Med 2010, 40: 1797-1810.
4. Nakash O, Liphshitz I, Keinan B L,. The effect of cancer on suicide among elderly Holocaust survivors. Suicide Life Threat Behav 2013, 43: 290-295.
5. Singer S, Das Munshi J, Br?hler E. Prevalence of mental health conditions in cancer patients in acute care a meta analysis. Ann Oncol 2009, 21: 925-930.
6. Roberts KJ, Lepore SJ, Helgeson V. Social cognitive correlates of adjustment to prostate cancer. Psycho Oncology: J Psychol, Soc Behav Dimens Cancer 2006, 15: 183-192.
7. Friedman LC, Kalidas M, Elledge R,. Optimism, social support and psychosocial functioning among women with breast cancer. Psycho Oncology: J Psychol, Soc Behav Dimens Cancer 2006, 15: 595-603.
8. Shao QJ, Huang WD. Application Status and Prospects of Narrative Nursing. J Changchun Univ Chin Med 2018, 34: 1230-1232.
9. Huang H, Liu YL. Research progress in clinical application of narrative nursing. Chin J Nurs 2016, 51: 196-200.
10. China Petroleum Central Hospital Li Chun. Narrative care: healing is not just a patient. Health News 2018-09-14, 005.
11. Ma WZ, Gu P, Shi ZY,. Analysis of hotspot of narrative nursing researches based on PubMed database. Chin Nurs Res 2018, 32: 3018-3024.
12. Higgins JP, Green S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [DB/OL].
13. Li XF. Influence of Narrative Therapy on Improving the Negative Emotion of Patients with Advanced Lung Cancer. Guangming J Chin Med 2019, 2250-2253.
14. Jin ZL, Hu SH, Chen PP,. Random control trial study on effect of narrative medicine mode on rehabilitation of patients. Chin J Pract Nurs 2017, 33: 1525-1529.
15. Ma L, Bian LL, Zhai QH. The effect of narrative nursing on negative emotion and quality of life in patients with advanced cancer. Pract Clin J Integr Tradit Chin West Med 2018, 18: 175-177.
16. Ding YX, Xie HM. Study on the influence of narrative nursing on the psychological elasticity of first-time cancer chemotherapy patients. Psychological 2018: 15-16.
17. Zeng QJ, Chen CR, Lu JJ,. Effect of narrative nursing on the physical and mental state of patients with esophageal cancer chemotherapy. J Nurs Train 2019, 34: 7-11.
18. Guo MY, Yan QH, Bian LL. Analysis of the influence of narrative nursing on the psychological elasticity of first-time cancer chemotherapy patients. Wisdom Health 2018, 4: 32-33, 36.
19. Kang L, Hao N, Guo PL,. The effect of narrative nursing on stigma of rectal cancer patients with colostomy. Chin Med Ethics 2018, 31: 1060-1064.
20. Jiang YH, Chen LH, Han FX. Effects of narrative nursing intervention on negative psychology and quality of life in patients with advanced gastric cancer. Today Nurs 2019, 26: 145-147.
21. Cao M, Huang JT, Wang G,. The effect of the narrative medicine on the stigma of radical mastectomy patients. Anhui Med Pharm J 2019, 23: 575-579.
22. Cui WW, Chen CL, Bai QX,. Efficacy of narrative medicine on the health education of patients with upper digestive tract cancer with bleeding. Chin J Clin Oncol Rehabil 2016, 23: 381-384.
23. Li N, Xu M, Zhang W,. The effect of narrative medicine mode on psycho-logical condition and life quality of young breast cancer patient underwent chemotherapy treatment. J Guizhou Med Univ 2018, 43: 682-685.
24. Zhu XT. Effect of narrative treatment on negative emotion in patients with lung cancer. Today Nurs 2017: 91-93.
25. Li H, Wang LY, Ma XL. Application of narrative medical nursing mode in patients after colorectal ostomy. Chin Gen Pract Nurs 2019, 17: 1076-1078.
26. Lloyd williams M, Cobb M, O'Connor C,. A pilot RCT to reduce suffering and emotional distress in patients with advanced cancer. J Affect Disord 2013, 148: 141-145.
27. Wise M, Marchand LR, Roberts LJ,. Suffering in advanced cancer: A randomized control trial of a narrative intervention. J Palliat Med 2018, 21: 200.
28. Hao J, Chen WQ. 2012 China cancer registration annual report. Beijing: Military Medical Science Press 2013: 2-3.
29. Xia F, Wei BF. Narrative evidence-based medicine and treatment of cancer. Med Philos (A) 2014, 35: 11-14.
30. Charon R. Narrative medicine: form function and ethics. Ann Intern Med 2001, 134: 83-87.
31. Charon R. Narrative medicine: a model for empathy, reflection, profession and trust. JAMA 2001, 286: 1897-1902.
32. Cheng Y. Advances in the application of narrative medicine in clinical nursing. Chin Gen Pract Nurs 2019, 17: 681-683.
33. Liang SQ, Cheng QM, He CY. Study on the improvement of anxiety and depression in hospitalized patients with liver failure by narrative nursing. J Nurs Train 2018, 33: 937-939.
34. American Psychology Association [Internet]. The road to resilience: what is resilience [cited 2019 Octorber 13]. Available from: http//www.apa.org/helpCenter/road-resilience.aap.
35. Zeng H, Zheng R, GuoY,. Cancer survival in China, 2003-2005: a population-based study. Int J Cancer 2015, 36: 1921-1930.
36. Taal B. Quality of life in colorectal cancer: stoma vs non-stoma patients. Dis Colon Rectum 1995, 38: 361-369.
37. Cakmak A, Aylaz G, Kuzu MA. Permanent stoma not only affects patients quality of life but also that of their spouses. World J Surg 2010, 34: 2872-2876.
38. WHO. The development of the WHO quality of life assessment instrument. Geneva: WHO 1993.
39. Luo J, Sun Y. Study on quality of life of cancer patients (I). Chin Tumors 1995, 4: 15-19.
Narrative nursing mode can effectively alleviate the degree anxiety and depression of patients and improve the capacity mental resilience and the quality of life.
This article systematically evaluated the effect of narrative nursing of patients with cancer. However, narrative therapy was not so widely used in hospitals. Narrative therapy would be more popular, covers all aspects form hospital to family.
Submitted: 14 September 2019,
14 October 2019,
Online: 16 November 2019.
Competing interests: Authors declare that they have no competing interests.
Copyright: ?2019 TMR Publishing Group Limited. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License.
*Correspondence: Ya-Nan Leng, Graduate School, Tianjin University of Traditional Chinese Medicine, No. 312, Anshan West Road, Nankai District, Tianjin 301617, China. E-mail: 1457666132@qq.com.
- Cancer Advances的其它文章
- Xiaoyan decoction inhibits tumor growth and improves the immunity of mouse with A549 lung carcinoma xenograft
- Miao medicine may serve as an essential adjuvant therapy in cancer treatment
- Null links between vitamin B6 and B12 intake and occurrence risk of lung cancer: a meta-analysis
- The role of Fuzheng Peiben in clinical oncology