
Combination of Chinese and Western medicine in the treatment of aggressive angiomyxoma: a case report
2019-09-05 11:21:02YanLiuZhengWeiJiaoTengHuangSiNingHaYanBoZuoXiaoShiJin
Cancer Advances 2019年3期
Yan Liu , Zheng-Wei Jiao, Teng Huang , Si-NingHa, Yan-Bo Zuo, Xiao-ShiJin,*
Yan Liu1, Zheng-Wei Jiao2, Teng Huang1, Si-NingHa2, Yan-Bo Zuo1, Xiao-ShiJin2,*
1Department of Medicine, Hebei University, Baoding, Hebei 071000, China.2Affiliated Hospital of Hebei University, Baoding, Hebei 071000, China.
Aggressive angiomyxoma (AAM) is a rare soft tissue tumor. Invasiveness and recurrence are important clinical features of AAM. A patient with recurrent AAM was admitted to the hospital. At present, the treatment for AAM is still based on surgerybecause it does not have lymph nodes and distant metastasis. Moreover, chemotherapy is of little significance. Traditional Chinese medicine believes the formation of tumor is related to blood stasis, so after surgery, a Chinese medicine called Xue-Shuan-Tong was used to improve blood circulation and disperses stasis. The drainage tube was removed on the 5th day after the operation and achieved a good wound healing. This article analyzes and demonstrates the pathogenesis of female vulvar invasive angiomyxoma from the perspective of modern medicine and traditional medicine, in order to provide a better understanding of the disease.
Aggressive angiomyxoma, Modern medicine, Traditional Chinese medicine
Although aggressive angiomyxoma (AAM) has some characteristics of malignant tumors, it does not cause distant metastasis.
Surgery combined with traditional Chinese medicine treatment may be a new way to treat AAM.
Introduction
Aggressive angiomyxoma (AAM) is a tumor with a very low incidence, and so far, no more than 500 cases have been reported (about 350 in foreign countries and about 150 in China). AAM always occurs in the lower abdomen and perineal area of women of childbearing age [1]. In clinical practice, the clinical symptoms of female vulvar AAM (FVAAM) are often atypical, and many are gradually increased to a certain extent and found by chance. The FVAAM is often confused with papular gland cysts, fibroids, femoral hernia or perineal abscess. The diagnosis of FVAAM mainly depends on pathological examination, so the preoperative misdiagnosis rate is high and may be close to 80%. At present, the treatment of FVAAM in our hospital is mainly based on surgery and improving blood circulation and dispersing [one of the therapeutic methods of traditional Chinese medicine (TCM)] treatment. Reports have also achieved good results through gonadotropin-releasing agonist.
Medical record information
On November 1, 2018, a patient with FVAAM was admitted to the Affiliated Hospital of Hebei University. The patient was 26 years old. The patient was admitted to our hospital mainly because of the recurrence of vulvar mass after surgery for about 2 years. There is no special medical history in the past. Physical examination demonstrated a mass located at the labia majora on the left side, and the size is about 13 × 10 cm. It was soft and had a good degree of activity. It had a clear boundary with the surrounding tissues. No redness, no tenderness, low surface skin temperature, and the boundary between the root and deep tissue of the mass was unclear. Auxiliary examination: ultrasound showed a low echo mass (solid mass) on the left labia, and the range was about 13.1 × 10.3 cm. The liquid dark area was visible in the pelvic cavity, and no obvious abnormalities were found in the uterus and bilateral attachments. Pelvic CT (Figure 1) showed that a mixed density shadow on the left side of the perineal skin, upward communication with the pelvic cavity, the cervix was pressed to the right, the uterus was normal, the parenchyma density was uniform, and the boundary of the mass with the surrounding tissue was clear. The rectal wall was normal, the lumen is not narrow, and the surrounding fat gap is clear. Preoperative diagnosis: vulvar mass and pelvic effusion.
After the examination, the genital tumor resection was performed. During the surgery (Figure 2), we found the tumor was dumbbell-shaped, extending to the pelvis, close to the rectum, vagina, and the mass was soft. After the operation, cefotiam was used to anti-infection, and sodium aescinate was used to anti-infecion and swelling. A Chinese patent called Xue-Shuan-Tong was used to improve blood circulation and disperses stasis. The drainage tube was removed on the 5th day after the operation and achieved a good wound healing.
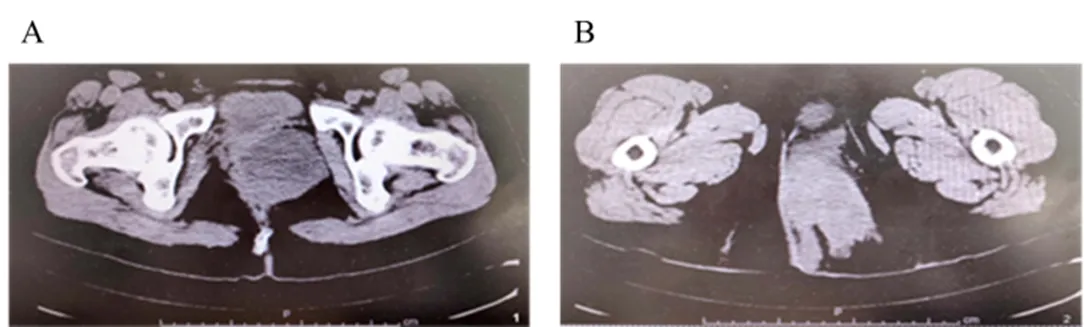
Figure 1 Pelvic CT of the patient
A, The FVAAM upward communication with the pelvic cavity; B, The cervix was pressed to the right. Note: FVAAM, female vulvar aggressive angiomyxoma.
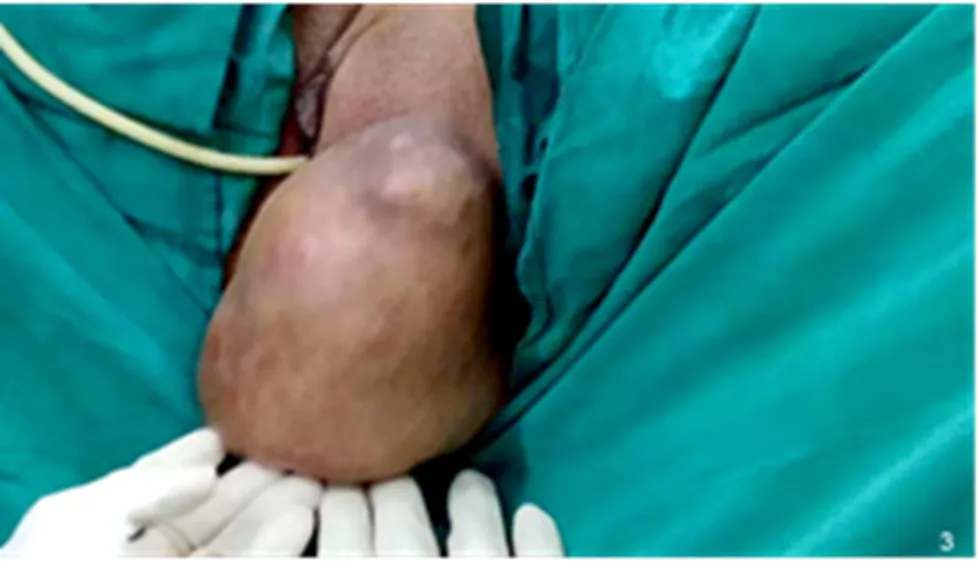
Figure 2 General appearance of FVAAM.
Note:FVAAM, female vulvaraggressive angiomyxoma.
Pathological showed a large number of small blood vessels with different diameters and vascular wall thickness. A large number of red blood cells can be seen in the blood vessels, and scattered, astral or short spindle-shaped tumor cells can be found in the mucus-like stroma. Tumor cells are eosinophilic, slightly stained, and inflammatory cell infiltration around the blood vessels. Pathological findings suggest invasive angiomyxoma (Figure 3). Clinical pathology results demonstrated that vimentin (+), desmin (+), smooth muscle actin (-), S100 protein (-), which meets the diagnosis of angiomyxoma.
Figure 3 Microscopic pathology of the tumor
The arrows indicate the blood vessels in the FVAAM. Note: FVAAM, female vulvar aggressive angiomyxoma.
Discussion
AAM is a clinical rare malignant stromal tumor. The disease was first described by Steeper [2] in 1983. There are no specific immunohistochemically markers in previous reports, and there is no unified immunohistochemically detection index [3]. AAM is more common in women, 90% occur in childbearing age, the age of high incidence is 20 to 40 years old, and the incidence rate of men and women is about 1 : 6 [4]. A local slow-growing cystic mass mostly characterizes the disease, the border is not clear, and the course of the disease is generally longer. If the tumor is large or oppresses surrounding tissues or organs, it may be accompanied by symptoms such as discomfort such as the perineum, labia majora, and pelvic cavity, inconvenient walking, discomfort in sexual intercourse, and pain in the compression site. Clinically, the diagnosis of AAM is rarely diagnosed preoperatively because FVAAM is easy to confuse with lipoma, Pap sac cyst, Gartner's cyst (vaginal wall cyst), or perineal abscess. The characteristics of this patient: 1. Young women. 2. The history of local vaginal surgery, the disease is easy to local recurrence. 3. The tumor grows in a dumbbell shape and partially protrudes into the pelvis. Patients are advised to review them regularly after discharge and provide long-term follow-up.
AAM pathology needs to be differentiated from the following diseases, for instance, superficial angiomyxoma, mucin-like liposarcoma, myxoma, and mucin-like neurofibroma. AAM's CT, MRI "vortex" and "stratification" and other specific performance contribute to clinical diagnosis and localization. The gold standard for diagnosis is pathological examination, which can be confirmed by pathological histological features and immunological markers.
At present, the treatment of AAM is mainly surgery, because it does not have lymph nodes and distant metastasis. Moreover, chemotherapy is of little significance [5]. Because of its aggressiveness, many reporting initiatives have taken to expand local vulvar resection to reduce local recurrence [6, 7]. The relevant research data showed that there is no significant difference in the recurrence rate of the disease, whether the resection margin is tumor negative or not [8]. Therefore, the scope of surgical resection has gradually become more conservative [9, 10]. Other related studies have shown that AAM is ER and PR are positive, and the tumor can be reduced or even disappeared by the application of gonadotropin-releasing agonist. By combining the nature of the disease with this nature, it is speculated that the pathogenesis of the tumor is closely related to the level of sex hormones (or factors affecting the endocrine secretion of sex hormone secretion), which is a hormone-dependent tumor [11, 12, 13].
As early as in the Han Dynasty, the Chinese medicine has the record of the name of the "tumor" in the ancient book of Chinese medicien Huangdi Neijing (202 B.C.E.-8 C.E.).In the Sui Dynasty (581-618 C.E.), doctors described that the etiology and pathogenesis of this disease lie in the virtual. TCM believes that the disease is more common in women because female personality is quiet and depressed, which may easily cause liver qi stagnation, and result in blood stasis. The treatment of TCM is based on the principle of "improve blood circulation and disperse stasis".
Conclusion
In summary, the pathogenesis of AAM is not fully understood at present. Surgical treatment combined with traditional medical treatment may be a new treatment. In further studies, the pathogenesis of AAM and the mechanism of recurrence are possible research directions.
1. Guo RJ, Qi Y, Liu S. Clinical analysis and literature review of 12 cases of invasive angiomyxoma. Chin J Practical Gynecol Obstet 2014, 1:55-58.
2. Steeper TA Rosai J. Aggressive angiomyxoma of the female pelvis and perineum. Report of nine cases of a distinctive type of gynecologic soft-tissue neoplasm. Am J Surg Pathol 1983, 7: 463-475.
3. McCluggage WG. A review and update of morphologically bland vulvovaginal mesenchymal lesions. Int J Gynecol Pathol 2005, 24: 26-38.
4. Yan H, Qin XG, Ren Y. Imaging diagnosis of invasive angiomyxoma. Chin J Clin Med Imag 2018, 29: 645-648.
5. Liang HX, Zhao J. Invasive angiomyxoma with vestibular gland abscess: a case report. China J Modern Med 2011, 21:1067-1068.
6. Simo M, Zapata C, Esquius J,. Aggressive angiomyxoma of the female and perineum: report of two cases and review of the literature. Br J Obstet Gynecol 1992, 99: 925- 927.
7. Elchalal U, Lifschitz-Mercer B, Dgani R,. Aggressive angiomyxoma of the vulva. Gynecol Oncol, 1992, 47: 260-262.
8. Mathieson A, Chandrakanth S. Aggressive angiomyxoma of the pelvis: a case report. Can J Surg 2007, 50: 228-229.
9. Haldar K, Martinek IE, Kehoe S. Aggressive angiomyxoma: a case series and literature review. Eur J Surg Oncol 2010, 36: 335-339.
10. Han-Geurts IJ, van Geel AN, van Doorn L,. Aggressive angiomyxoma: multimodality treatments can avoid mutilating surgery. Eur J Surg Oncol 2006, 32: 1217-1221.
11. Sutton BJ, Laudadio J. Aggressive angiomyxoma. Arch Pathol Lab Med 2012, 136: 217-221.
12. Shinohara N, Nonomura K. Medical management of recurrent aggressive angiomyxoma with gonadotropin-releasing hormone agonist. Inter J Urol 2004, 11: 432-435.
13. Fine BA, Munoz AK, Litx LE,. Primary medical management of recurrent aggressive angiomyxoma of the vulva with a gonadotropin-releasing hormone agonist. Gynecol Oncol 2001, 81: 120-122.
14. Zhao LM, Ye LH. "Synopsis of prescriptions of the golden chamber" and tumor therapy. J Zhejiang Univer Tradit Chin Med 2015, 39:632-635.
19 May 2019,
13 June 2019,
27 June 2019.
Authors declare that they have no competing interests.
?2019 TMR Publishing Group Limited. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License.
Aggressive angiomyxoma (AAM) is a tumor that occurs mainly in women, and its mechanism and treatment are still in the exploratory stage. Traditional Chinese medicine may exert a certain effect in the treatment of AAM. But the mechanism that works is still in need of further laboratory research.
Xiao-Shi Jin, Affiliated Hospital of Hebei University, No. 212, Yuhua East Road, Baoding, Hebei, 071000, China, E-mail: doctorjinxiaoshi@126.com.
- Cancer Advances的其它文章
- The clinical efficacy analysis of radiofrequency ablation combined with chemotherapy in treating late non-small cell lung cancer
- Treatment of undifferentiated thyroid carcinoma with darafini and trametinib: a case report and literature review
- The differences and similarities between regional ethnic medicine and traditional Chinese medicine in the prevention and treatment of cancer pain
- Research progress in the treatment of colorectal cancer in classical prescriptions