
Effectiveness of taxanes over anthracyclines in neoadjuvant setting:A systematic-review and meta-analysis
2019-08-28 12:35:26MonaPathakSadaNandDwivediSVSDeoBhaskarThakurVishnubhatlaSreenivasGouraKishorRath
World Journal of Meta-Analysis 2019年4期
Mona Pathak,Sada Nand Dwivedi,SVS Deo,Bhaskar Thakur,Vishnubhatla Sreenivas,Goura Kishor Rath
Mona Pathak,Sada Nand Dwivedi,Vishnubhatla Sreenivas,Department of Biostatistics,All India Institute of Medical Sciences,New Delhi 110029,India
Mona Pathak,Bhaskar Thakur,Division of Biostatistics,Kalinga Institute of Medical Sciences,Bhubaneswar 751024,India
SVS Deo,Department of Surgical Oncology,BRAIRCH,All India Institute of Medical Sciences,New Delhi 110029,India
Goura Kishor Rath,Department of Radiotherapy,BRAIRCH,All India Institute of Medical Sciences,New Delhi 110029,India
Abstract
Key words: Docetaxel; Paclitaxel; Epirubicin; Doxorubicin; Pathological complete response; Breast conserving surgery
INTRODUCTION
Neoadjuvant chemotherapy,given prior to loco-regional treatment (surgery/radiotherapy) is standard of care for locally advanced breast cancer but now became popular for early breast cancer as well[1].The response to chemotherapy depends on the used regimen.Anthracyclines and taxanes are more active group of chemotherapy regimen used for breast cancer[2].These regimens are usually administered with other chemotherapy drugs like cyclophosphamide,flurourocil.Anthracyclines based drugs include doxorubicin,epirubicin and mitoxantrone.On the other hand,widely used taxanes,originally identified from plant of genus Taxus,are docetaxel and paclitaxel[3].Neoadjuvant chemotherapy increases the chance of breast conserving surgery (BCS) but there is no consensus regarding role of chemotherapy drugs in further increasing BCS rate[4,5].Further,pathological complete response (pCR) to neoadjuvant chemotherapy predict long term survival outcomes as the breast cancer patients achieving pCR have better survival than the patients who do not[6].The reported results from randomized controlled trials (RCTs) were contradictory as some favored taxanes based chemotherapy over anthracyclines based chemotherapy[7,8]regarding pCR,while some showed the other way[9,10].The efficacy of taxanes over anthracyclines has been examined and found to be associated with increased overall survival in adjuvant setting[11].Two reviews have discussed about the relative effectiveness of taxanes but could not synthesize the results for response because of very few RCTs at that point of time[12,13].Further,these reviews could not comment on the effect of taxanes on long term outcomes.To the best of our knowledge,the relative efficacy of taxanes over anthracyclines has not been synthesized in neoadjuvant setting.Accordingly,present study aims to assess the effectiveness of taxanes based Neoadjuvant chemotherapy in comparison to anthracyclines based neoadjuvant chemotherapy on the basis of pCR,clinical responses,breast conserving surgeries and survival outcomes in female breast cancer patients by systematic review and metaanalysis of RCTs.
MATERIALS AND METHODS
The present systematic review is designed as per the guidelines of Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA)[14-16].This study has been registered with International prospective register of systematic reviews and the registration Number is CRD42016027236.
Eligibility criteria
All RCTs assessing efficacy of taxanes based Neoadjuvant Chemotherapy (NACT) in comparison to anthracyclines based NACT in the management of breast cancer,published in English language were considered.There was no restriction regarding the regimens used in the chemotherapy.The Population,Intervention,Comparator,Outcome and Time considered in the present systematic review is given below:(1)Population:Non-metastatic Female Breast Cancer Patients; (2) Intervention:Taxanes(Docetaxel or Paclitaxel); (3) Comparator:Anthracyclines; (4) Outcomes:PCR,overall response (OR) and BCS; (5) Design:RCTs; and (6) Time:Assessed on and up to 28 April 2017.
Outcome definitions
pCR:pCR was reported under three definitions as follows:(1) pCR1:pCR was defined as complete response of primary as well as axilla; (2) pCR2:pCR was defined as complete response of primary regardless of axilla; and (3) pCR3:pCR was defined as complete response of primary allowing for ductal carcinomain situ(DCIS).
Considering variability in the definitions,results were synthesized separately under these three definitions.
OR:OR was defined as complete disappearance of clinically palpable tumor or more than 50% reduction in tumor volume.
BCS:BCS rate was defined as rate of breast conserving surgery,i.e.,removal of lump only or removal of partial breast including tumor as well as some normal tissues.
Long term outcomes,i.e.,overall survival,disease free survival,loco-regional recurrence free survival and metastasis free survival were also considered as secondary outcomes.
Information sources and study selection
Details of search strategies development as well as electronic search strategies for PubMed and Cochrane register of controlled trials along with methodologies for study selection are available in the published protocol[17].Data collection process,data extraction tool and method for risk of bias assessment are also available under published protocol.There was no deviation from the published protocol[17].
Summary measures
Effect sizes under consideration were “risk ratio” for all response outcomes and BCS.However,long term outcomes including,overall survival,disease free survival,locoregional recurrence and distant metastasis,it was “hazards ratio”.
Data synthesis and analysis
Statistical heterogeneity was examined byI2statistics[18].Publication bias assessment was performed using Eggers test and visualized using funnel plot[19].In case of very low extent of heterogeneity (i.e.,I2= 0-25%),fixed effect method of synthesizing the effect size was used.However,for moderate to large extent of heterogeneity random effect method of meta-analysis was used.All analyses were performed using Stata 14(StataCorp,Texas,United States) and RevMan 5.3.3,Copenhagen:The Nordic Cochrane Centre,The Cochrane Collaboration,2014.
Additional analysis
To derive additional inferences,Subgroup analyses were performed for the RCTs comparing taxanes versus anthracycline; and,addition of taxanes to anthracyclines versus anthracyclines under neoadjuvant setting.
RESULTS
Study selection
A total of 16 RCTs comparing effectiveness of taxanes versus anthracyclines involving 6752 breast cancer patients and measuring atleast one of the considered outcomes were found eligible out of 1286 searched records.These details are presented using PRISMA flow chart (Figure 1).
Study characteristics
RCTs assessing the effectiveness of taxanes were sub-divided in two groups,i.e.,RCTs comparing taxanes alone to anthracyclines alone[20-23](n= 5); and RCTs comparing taxanes and anthracyclines together to anthracyclines alone[4-6,9,24-30](n= 11).Out of these 16 RCTs,10 RCTs assessed the effectiveness of docetaxel (3 RCT assessed the effectiveness of docetaxelvsdoxorubicin along with other chemotherapy drugs however 7 RCTs assessed effectiveness of addition of docetaxel to anthracyclines based chemotherapy).However,six RCTs assessed effectiveness of paclitaxel,more precisely two RCT assessed paclitaxel and four RCT assessed addition of paclitaxel to anthracyclines based chemotherapy.The details of Population,intervention and outcome are presented in Table 1.
Risk of bias within studies
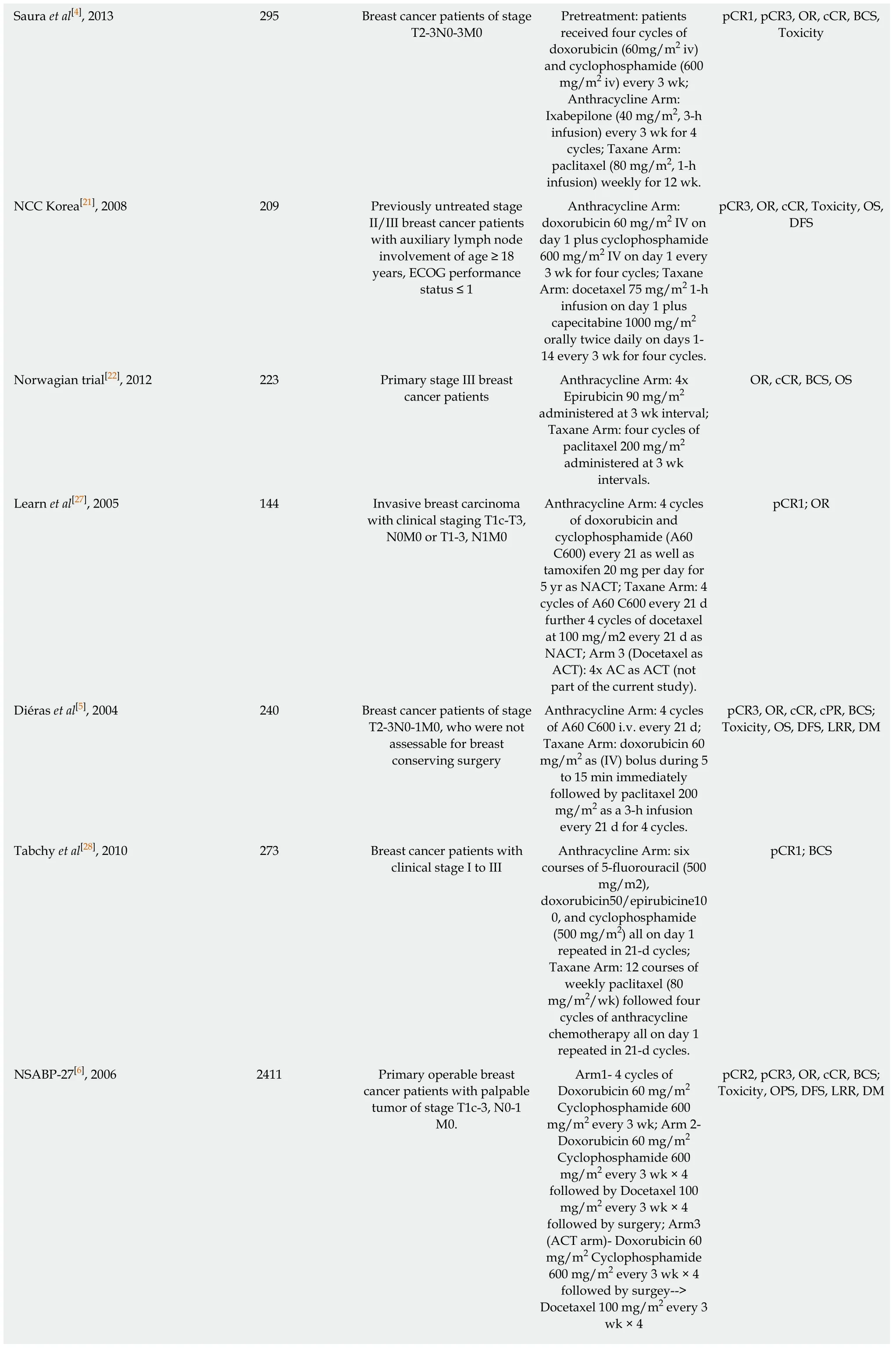
Risk of bias was assessed for each individual study using Cochrane bias assessment tool Figure 2.However,overall summary of risk of bias for all considered studies is presented in Figure 3.In summary,there were around 30% of the studies,which did not perform blinding of patients and/or outcome assessment.In addition,a large proportion of the trials did not report sufficient details to judge blinding.However,it is worthwhile to mention here that objective measurement of pCR and BCS was not affected by non-blinding of outcome assessment.But clinical responses might get affected by non-blinding of outcome assessment because of obvious subjectivity.
Publication bias
There was no publication bias for any of the outcomes except OR while assessing the effectiveness of taxane based chemotherapy tested using Egger's test (Table 2) and visualized using Funnel Plots.
Meta-analysis
Pathological complete response:As mentioned earlier,effect sizes were synthesized separately under three definitions of pCR.Considering pCR to breast as well axilla reported under eight RCTs randomizing 1442 patients,127 (16.8%) in anthracycline arm and 127 (18.5%) in taxane arm achieved pCR.But this increase in pCR with taxane (especially with addition of taxane to anthracycline) was not statistically significant (n= 8,I2= 34.4%,RR = 1.14,95%CI:0.84-1.55).Further,subgroup analyses also revealed the similar results for anthracycline versus taxane (n= 2,I2= 38.3%,RR=0.74,95%CI:0.23-2.39) as well as anthracycline versus taxane along with anthracycline (n= 6,I2= 41.9%,RR = 1.23,95%CI:0.86-1.76).Although some of the RCTs on which evidence is based were non-blinded but objective measurement of pCR would not change drawn evidences which were graded as high (Table 2).
PCR of breast regardless of axilla was reported by seven RCTs randomizing 4007 patients due to inclusion of two large RCTs[26,31]which contribute around 50% in the pooled effect estimates.Out of these seven RCTs,six RCTs assessed the effectiveness of addition of taxanes.pCR by this definition was observed to be 16.8% with anthracycline group and 23.0% in taxane group which was found to be statistically significant because of significant results under two big RCTs involving 390 patients (I2= 72.6%,RR = 1.48,95%CI:1.04-2.12).Similarly,pCR of breast with DCIS was found to be significantly higher in taxanes group (I2= 69.6%,RR = 1.54,95%CI:1.11-2.15).Apart from inclusion of some non-blinded trials for the objectively measured outcomes,evidences were downgraded one label to moderate due to high heterogeneity.The third definition of pCR,i.e.,allowing for DCIS revealed beneficial effect of addition of taxanes to anthracycline based chemotherapy.
Clinical response:OR measured clinically was higher with taxane based chemotherapy (79.0%) in comparison to anthracycline based chemotherapy (73.5%) (I2=69.1%,RR = 1.13,95%CI:1.04-1.24).Similarly,addition of taxane based chemotherapy also improved clinical complete response in comparison to anthracyclines alone (I2= 49.5%,RR = 1.18,95%CI:0.97-1.44).Subjective measurement of these outcomes was based on few non-blinded trials which downgraded the evidence one level.Further,due to high heterogeneity and presence of publication bias,evidence for OR further downgraded to Low but that for complete clinical response remains at moderate level.
Breast conserving surgery:Taxane based chemotherapy could not further improve BCS,weather it was given with or without anthracycline in comparison to anthracyclines (I2= 1%,RR = 1.04,95%CI:0.98-1.10) with high grade of evidence.
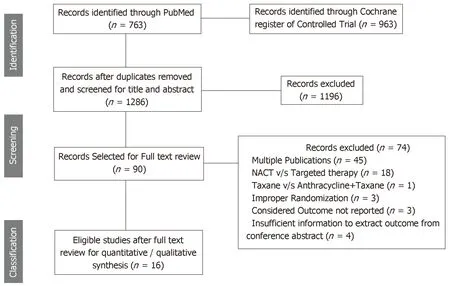
Figure 1 Preferred Reporting ltems for Systematic Reviews and Meta-Analysis flow chart for inclusion of studies.
Survival and recurrences:Long term outcomes like overall survival outcomes,disease free survival and recurrences were reported by very few RCTs.A total of seven RCTs (Three compared taxane v/s anthracycline and four RCTs compared anthracycline + taxane v/s anthracycline) reported overall survival (Table 2).Overall survival was relatively better with taxane based NACT in comparison to anthracyclines but due to few RCTs,it could not reach at significance level [n= 7,RR= 0.86 (0.70-1.05)].However,taxanes based NACT especially addition of taxanes to anthracycline based NACT significantly improved disease-free survival [n= 6,RR =0.89 (0.80-0.99)].Recurrences,i.e.,loco-regional recurrence and distant metastasis were reported by only four RCTs comparing addition of taxanes to anthracycline based NACT in comparison to anthracycline alone.Taxanes played a significant role in combating loco-regional recurrence [RR=0.74 (0.59-0.94)] but not distant metastasis[RR=0.94 (0.82-1.07)].
Toxicities:Meta-analysis of toxicities involve both group of RCTs comparing taxane alonevsanthracycline alone as well as taxane and anthracycline combinationvsanthracycline alone.In comparison to anthracycline based chemotherapy,taxane based chemotherapy was found to lower down the risk for nausea (n=7,RR = 0.33,95%CI:0.24-0.44) and vomiting (n= 4,RR = 0.23,95%CI:0.16-0.33) (Table 3).In contrary,it was found to raise the chance of febrile Neutropenia [n= 4,RR = 2.67(2.33-3.07)] and infection [n= 4,RR = 2.53 (2.00-3.19)] significantly.However,due to lack of sufficient sample size/event rate,stable results could not be obtained for allergic reaction,hand foot syndrome,sensory neuropathy,gastrointestinal problems and dermatological problems as the confidence interval of the related risk ratio was observed to be very wide while comparing taxanes and anthracyclines.
DISCUSSION
A total of 16 RCTs assessing efficacy of taxanes based NACT (taxanes alone or addition of taxanes) in comparison to anthracyclines based NACT in the treatment of breast cancer,reporting at least one of the considered outcomes were included for this systematic review and meta analyses.Out of these trials,most of the big RCTs compared addition of taxanes to anthracyclines over anthracyclines (having 86% of the total randomized patients among all 16 RCTs).Meta-analysis sample size varied for outcome-wise synthesis.It was highest with 11 RCTs reporting clinical responses,i.e.,OR and clinical complete response.Further,pCR was reported by six to eight RCTs with varying definitions and BCS rates were reported by 9 RCTs.Survival outcomes (overall survival and disease free survival) were reported by only seven RCTs and recurrences (loco-regional recurrences and distant metastasis) werereported by only four RCTs assessing the effectiveness of addition of taxanes over anthracyclines alone.Pattern of reported toxicities were also varied among RCTs.Most of the trials (n= 7) reported Neutropenia.All of the included RCTs used proper method for randomization but enough information to assess concealment was not reported by many RCTs.Further,six out of 16 RCTs were open label RCTs and may have an obvious impact on subjectively measured outcomes like OR and clinically complete response.Most of the RCTs have reported results based on intention to treat analysis.Overall,quality of included RCTs can be treated as adequate for objectively measured outcomes.Further,quantity of RCTs was sufficient to assess the relative effectiveness of addition of taxanes to anthracyclines over anthracyclines alone but not for subgroup assessing efficacy of taxanes alone versus anthracyclines alone.
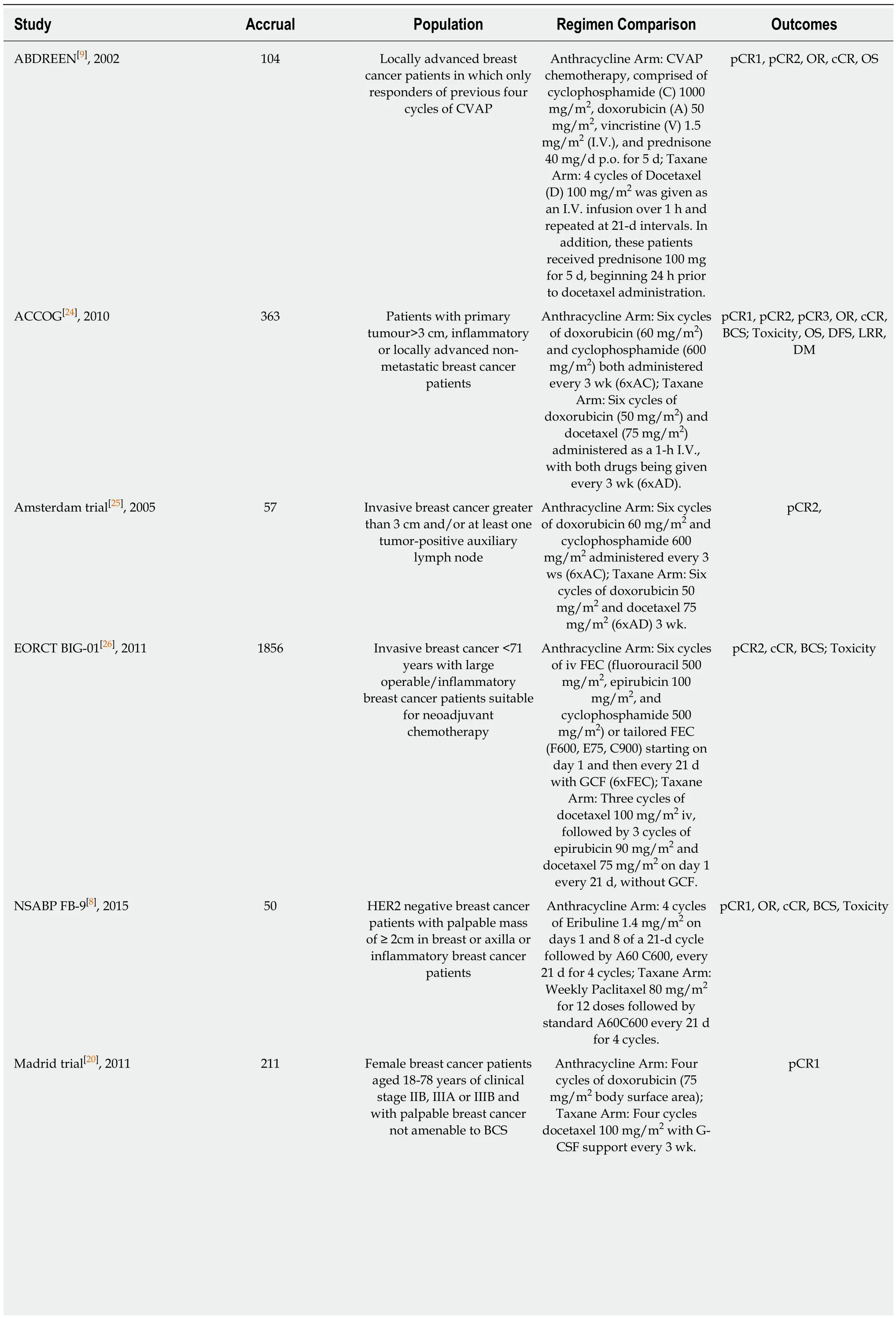
Table 1 Population,intervention,comparison and outcome characteristics of included studies
Saura et al[4],2013 295 Breast cancer patients of stage T2-3N0-3M0 Pretreatment:patients received four cycles of doxorubicin (60mg/m2 iv)and cyclophosphamide (600 mg/m2 iv) every 3 wk;Anthracycline Arm:Ixabepilone (40 mg/m2,3-h infusion) every 3 wk for 4 cycles; Taxane Arm:paclitaxel (80 mg/m2,1-h infusion) weekly for 12 wk.pCR1,pCR3,OR,cCR,BCS,Toxicity NCC Korea[21],2008 209 Previously untreated stage II/III breast cancer patients with auxiliary lymph node involvement of age ≥ 18 years,ECOG performance status ≤ 1 Anthracycline Arm:doxorubicin 60 mg/m2 IV on day 1 plus cyclophosphamide 600 mg/m2 IV on day 1 every 3 wk for four cycles; Taxane Arm:docetaxel 75 mg/m2 1-h infusion on day 1 plus capecitabine 1000 mg/m2 orally twice daily on days 1-14 every 3 wk for four cycles.pCR3,OR,cCR,Toxicity,OS,DFS Norwagian trial[22],2012 223 Primary stage III breast cancer patients Anthracycline Arm:4x Epirubicin 90 mg/m2 administered at 3 wk interval;Taxane Arm:four cycles of paclitaxel 200 mg/m2 administered at 3 wk intervals.OR,cCR,BCS,OS Learn et al[27],2005 144 Invasive breast carcinoma with clinical staging T1c-T3,N0M0 or T1-3,N1M0 Anthracycline Arm:4 cycles of doxorubicin and cyclophosphamide (A60 C600) every 21 as well as tamoxifen 20 mg per day for 5 yr as NACT; Taxane Arm:4 cycles of A60 C600 every 21 d further 4 cycles of docetaxel at 100 mg/m2 every 21 d as NACT; Arm 3 (Docetaxel as ACT):4x AC as ACT (not part of the current study).pCR1; OR Diéras et al[5],2004 240 Breast cancer patients of stage T2-3N0-1M0,who were not assessable for breast conserving surgery Anthracycline Arm:4 cycles of A60 C600 i.v.every 21 d;Taxane Arm:doxorubicin 60 mg/m2 as (IV) bolus during 5 to 15 min immediately followed by paclitaxel 200 mg/m2 as a 3-h infusion every 21 d for 4 cycles.pCR3,OR,cCR,cPR,BCS;Toxicity,OS,DFS,LRR,DM Tabchy et al[28],2010 273 Breast cancer patients with clinical stage I to III Anthracycline Arm:six courses of 5-fluorouracil (500 mg/m2),doxorubicin50/epirubicine10 0,and cyclophosphamide(500 mg/m2) all on day 1 repeated in 21-d cycles;Taxane Arm:12 courses of weekly paclitaxel (80 mg/m2/wk) followed four cycles of anthracycline chemotherapy all on day 1 repeated in 21-d cycles.pCR1; BCS NSABP-27[6],2006 2411 Primary operable breast cancer patients with palpable tumor of stage T1c-3,N0-1 M0.Arm1-4 cycles of Doxorubicin 60 mg/m2 Cyclophosphamide 600 mg/m2 every 3 wk; Arm 2-Doxorubicin 60 mg/m2 Cyclophosphamide 600 mg/m2 every 3 wk × 4 followed by Docetaxel 100 mg/m2 every 3 wk × 4 followed by surgery; Arm3(ACT arm)-Doxorubicin 60 mg/m2 Cyclophosphamide 600 mg/m2 every 3 wk × 4 followed by surgey-->Docetaxel 100 mg/m2 every 3 wk × 4 pCR2,pCR3,OR,cCR,BCS;Toxicity,OPS,DFS,LRR,DM

pCR1:Pathological complete response to breast as well as axilla; pCR2:Pathological complete response to breast regardless of axilla; pCR3:Pathological complete response to breast allowing for ductal carcinoma in situ; NACT:Neoadjuvant Chemotherapy; OR:Overall response; cCR:Clinical complete response; BCS:Breast conserving surgery; OS:Overall survival; DFS:Disease free survival; LRR:Loco-regional recurrence; DM:Distant metastasis.
The effectiveness of neoadjuvant chemotherapy depends on the used regimens.Response to neoadjuvant chemotherapy predict the prognosis and recurrence in breast cancer patients regardless of the type of surgery performed[32].Patients having pCR have prolonged disease-free survival and overall survival.NSABP B-18 and B-27 trials revealed significantly better disease-free survival and overall survival among patients achieving pCR in comparison to the patients who could not[6].It revealed that pCR is valid surrogate point for long term outcomes.This may be the reason; most of the trials comparing two neoadjuvant chemotherapy regimens reported tumor response instead of survival outcomes.Anthracyclines and taxanes are most active groups of chemotherapy regimens.Taxanes are standard of care for metastatic breast cancer patients because they are significantly more effective than anthracyclines based regimens[33].Systematic review to assess the role of taxanes was performed a long back in 2004 and 2005 by Nowaket al[12]and Trudeauet al[13].But most of the RCTs assessing effectiveness of taxanes over anthracyclines were reported after publication of these two reviews.Further,these two reviews included abstracts of ongoing trials which were not complete at that point of time.Since trials were not mature to report survival outcomes,these two studies could not comment on efficacy of taxanes for long term outcomes like survival and recurrences[13].Further,Due to availability of very few trials,these two reviews could not perform meta-analysis for response outcomes and limit their finding with qualitative synthesis of these trials.As a matter of fact,present study could be able to quantitatively synthesize the results of tumor responses as well as for long term outcomes like overall survival,disease free survival,loco-regional recurrence and distant metastasis.
Figure 2 Risk of bias assessed for each individual study using Cochrane bias assessment tool.
Addition of taxanes to anthracyclines based chemotherapy was found to be associated with higher pCR,better disease-free survival and decreased loco-regional recurrence.It was also found beneficial for clinical responses like OR and clinical complete response.But evidences on clinical responses have limited use due to downgrading of their quality because of involvement of some non-blinded trials.Also,clinical response to NACT also guides for further systemic therapy[34,35].NACT increases the chance of BCS[36]but taxanes could not further improve the conservation surgery rate over anthracyclines alone.Evidences for the subgroup assessing effectiveness of addition of taxanes to anthracyclines over anthracyclines were rated as of high grade and stable due to availability of large RCTs with adequate number.On the other hand,synthesized results for the subgroup comparing taxanes alone to anthracyclines alone involved few RCTs that too of small sample size.Further,the conclusive results for toxicities cannot be summarized because these were reported by very few RCTs and reporting of toxicities also involved variation in their definitions.In summary,addition of taxanes improves pCR,disease free survival and locoregional recurrence free survival but has no major impact on BCT rates.
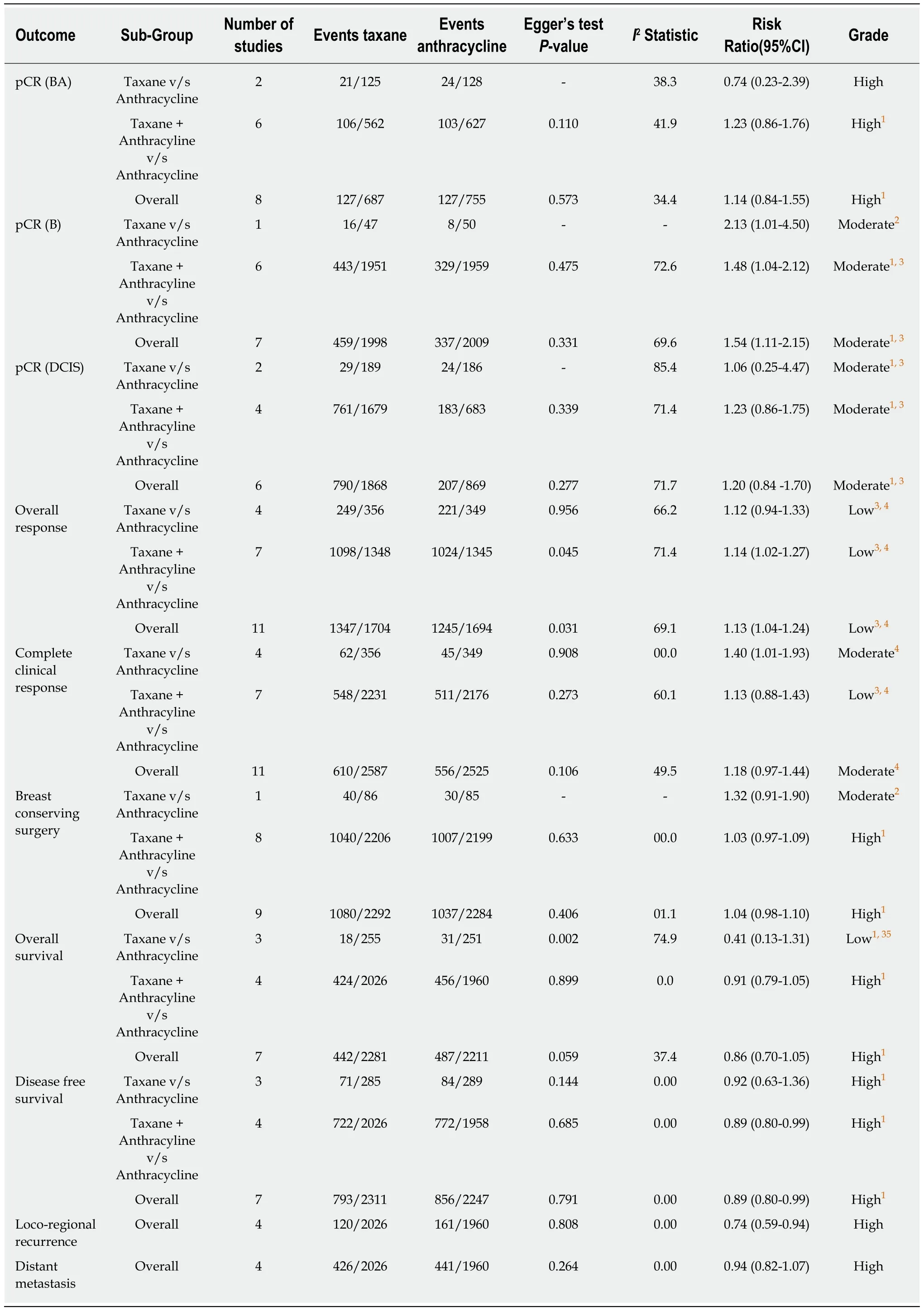
Table 2 Subgroup as well as overall meta-analysis for all considered outcomes
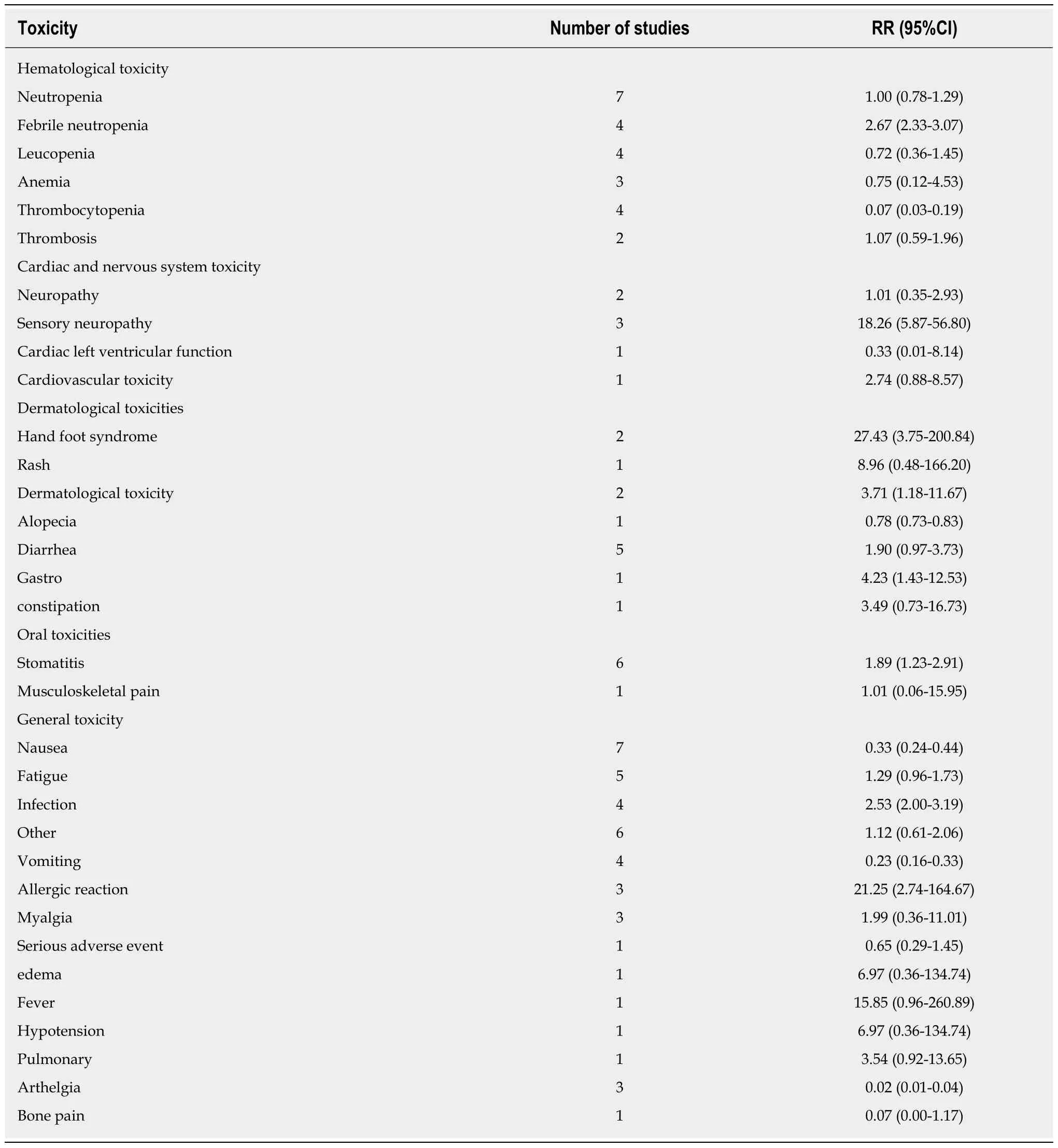
Table 3 Pooled effect estimates for various toxicity in taxanes in comparison to anthracyclines
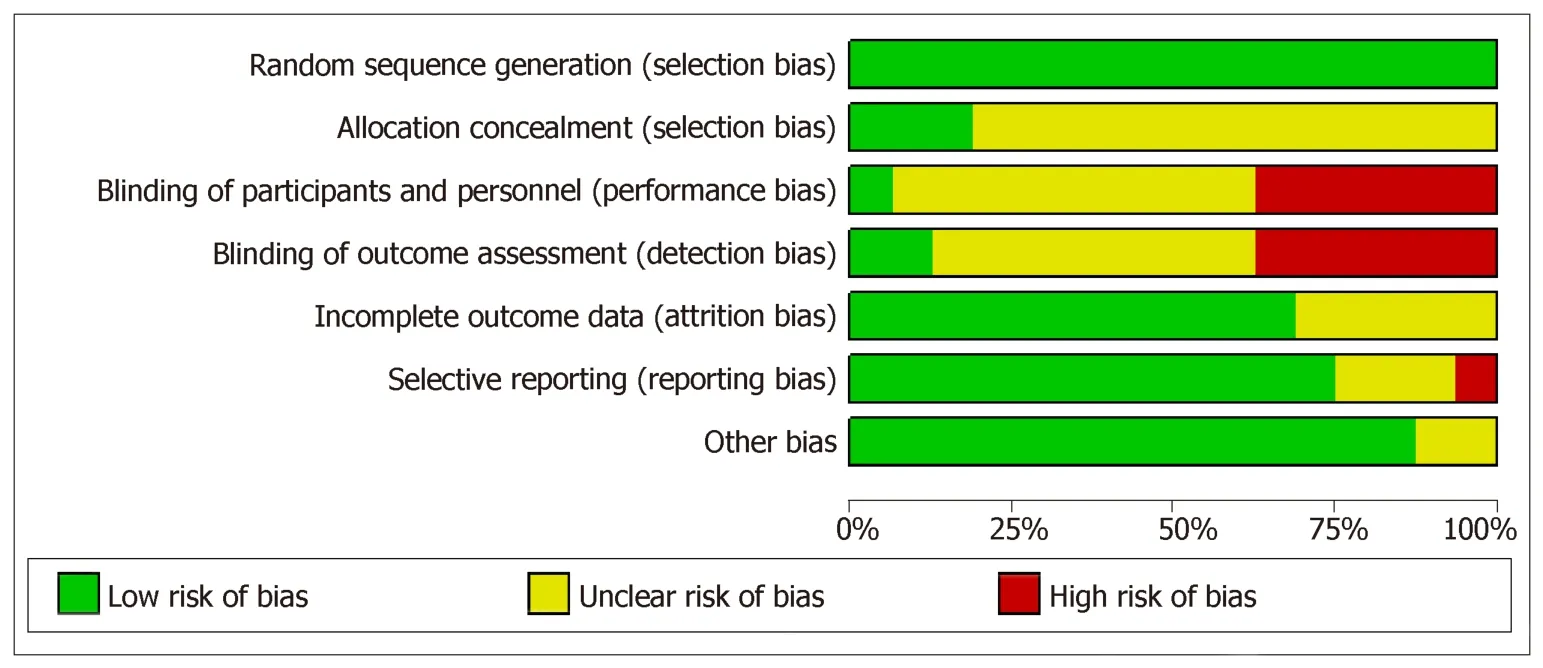
Figure 3 Summary risk of bias using Cochrane bias assessment tool.
ARTICLE HIGHLIGHTS
Research background
There are mainly two active group of chemotherapy regimen namely Anthracyclines and taxanes.Randomized controlled trials (RCTs) have reported variable evidences regarding efficacy of taxanes over anthracyclines especially for tumor response and survival outcomes.Hence,as required,the present study synthesizes the relative efficacy of taxanes over anthracyclines using pathological complete response,clinical responses,breast-conserving surgeries and survival outcomes in female breast cancer patients by systematic review and metaanalysis of available RCTs.
Research motivation
There is contradictory reporting regarding relative efficacy of taxanes over anthracycline.To resolve this,for the first time,present meta-analysis is to assess the relative efficacy of taxanes(Docetaxel and Paclitaxel) alone or their addition to anthracyclines over anthracyclines alone in terms of pCR,clinical response,breast conserving surgery,survival outcomes and toxicity in neo-adjuvant setting.As and when there is further addition in regimes,such appraisals from time to time are unavoidable.
Research objectives
Keeping in view of contradictory reporting,this study aimed to assess the relative effectiveness of taxanes over anthracyclines in neo-adjuvant setting in terms of tumor response and survival outcomes through systematic review and Meta analysis.This was expected to provide important clues regarding appropriate clinical practice.
Research methods
The RCTs have reported contra dictory findings on relative effectiveness of taxanes over anthracyclines in neo-adjuvant setting regarding treatment of breast cancer patients.In spite of this,no earlier attempt is made to synthesize relative effectiveness of taxanes over anthracyclines.For the first time,using a focused systematic review and Meta analysis of existing RCTs,this study attempted to synthesize relative effectiveness of taxanes over anthracyclines in terms of pCR,clinical response,BCS,survival outcomes and toxicity in neoadjuvant setting.For this,all related RCTs were searched through PubMed and Cochrane register of controlled trials on 28 April 2017 and published in English language.Using PRISMA guidelines,retrieved records were screened and data were extracted by two independent reviewers.Depending on heterogeneity assessed through I2 statistic,Meta-analysis was performed using either fixed effect or random effect method.Subgroup meta-analyses were also performed for each considered outcomes on the basis of taxanes alone or taxanes along with anthracyclines in comparison to anthracyclines alone.
Research results
Through a search through PubMed and Cochrane register of controlled trials on 28 April 2017,for this study,a total of 16 RCTs were found eligible in view of reporting at least one of the considered outcomes.The analytical results revealed that taxanes based chemotherapy significantly improved pCR,disease free survival and loco-regional recurrence free survival.Further,subgroup analysis showed that addition of taxanes to anthracyclines has better effectiveness regarding these survivals over anthracyclines alone than taxanes alone over anthracyclines alone.
Research conclusions
This study hypothesized that effectiveness of neo-adjuvant chemotherapy may rely on used regimens.Keeping in view of varying reporting under related RCTs,as an appraisal,to assess relative effectiveness of taxanes in comparison to anthracyclines was planned.For this,it was carried out as a first systematic review and Meta analysis of the related RCTS.As obvious,as a first-time observation,the synthesized results suggest that taxanes based chemotherapy may significantly improve pCR,disease free survival and loco-regional recurrence free survival.Further,as additional clues,subgroup analysis showed that addition of Taxanes to anthracyclines emerged to be more effective regarding these survivals over anthracyclines alone than taxanes alone over anthracyclines alone.
Research perspectives
In presence of contradictory findings under RCTs,a systematic review and Meta analysis of available RCTs may provide important clues towards clinical practice.Completeness of data is crucial for such studies.To achieve this,as true in case of other study designs,an appropriate protocol needs to be written for carrying out such studies.Although such studies are being carried out on other study designs as well,to ensure high level of evidence,such studies on RCTs need to be preferred.
 World Journal of Meta-Analysis2019年4期
World Journal of Meta-Analysis2019年4期
- World Journal of Meta-Analysis的其它文章
- Drug interactions of dipeptidyl peptidase 4 inhibitors involving CYP enzymes and P-gp efflux pump
- Anti-inflammatory properties of antidiabetic agents
- Safety and efficacy of percutaneous transhepatic balloon dilation in removing common bile duct stones:A systematic review
- Subcellular expression of maspin-from normal tissue to tumor cells
- Endoscopic management of biliary strictures post-liver transplantation