
Incidence and mortality of thyroid cancer in China, 2008-2012
2019-03-16 03:24:20LingbinDuRunhuaLiMinghuaGeYouqingWangHuizhangLiWanqingChenJieHe
Lingbin Du, Runhua Li, Minghua Ge, Youqing Wang, Huizhang Li, Wanqing Chen, Jie He
1Zhejiang Cancer Center, Zhejiang Cancer Hospital, Hangzhou 310022, China; 2National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Science & Peking Union Medical College, Beijing 100021, China
*These authors contributed equally to this work.
Correspondence to: Wanqing Chen. National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Science &Peking Union Medical College, Beijing 100021, China. Email: chenwq@cicams.ac.cn; Jie He. National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing 100021,China. Email: hejie@cicams.ac.cn.
Abstract Objective: To analyze the incidence and mortality rates of thyroid cancer (TC) in China from 2008 to 2012.Methods: Incident and death cases of TC were retrieved from the National Central Cancer Registry (NCCR)database collecting from 135 cancer registries in China during 2008-2012. The crude incidence and mortality rates of TC were calculated by area (urban/rural), region (eastern, middle, western), gender and age group (0, 1-4, 5-9,…, 85+). China census in 2000 and world Segi's population were applied for age-standardized rates. Joinpoint(Version 4.6.0.0) model was used for time-trend analysis.Results: The crude incidence rate of TC was 7.56/100,000 which ranked the seventh in overall cancers. The agestandardized incidence rates by China population (ASIRC) and by World population (ASIRW) were 6.25/100,000 and 5.52/100,000, respectively. The crude mortality of TC in China was 0.52/100,000. The age-standardized mortality rates by Chinese standard population (ASMRC) and by world standard population (ASMRW) were 0.34/100,000 and 0.32/100,000, respectively. Incidence and mortality rates of TC were higher in females than in males and higher in urban areas than in rural areas. Eastern areas had the highest incidence followed by middle and western areas. TC incidence increased dramatically after age of 15 years, then peaked at 14.08/100,000 in the group of 50-54 years and finally decreased sharply after 55 years old. TC mortality increased with age in population,reaching the peak of 5.09/100,000 in sub-population aged 85 years or older. TC incidence increased by 4.73 times from 2.40/100,000 in 2003 to 13.75/100,000 in 2012 with an average annual increase of 20%, while TC mortality only increased slightly around 0.32/100,000 from 0.26/100,000 to 0.36/100,000.Conclusions: Appropriate targeted prevention, early detection and treatment programs can be carried out to curb the rapid growth trend of TC and control the disease burden.
Keywords: Thyroid cancer; incidence; mortality; cancer registration; China
Introduction
Thyroid cancer (TC) is the most common head and neck malignancy of the endocrine system. In the past 30 years,except for Africa where disease diagnosis technology is limited, the rapid increase of TC incidence in the world has aroused widespread concern. A recent TC incidence in China is 12.40/100,000 in 2014, becoming one of the increasing fastest malignant tumors (1). According to the world cancer report (GLOBOCAN 2012), the global estimated incidence of TC in 2012 was 298,102 cases and 39,771 deaths (2). According to the 2015 annual report of Chinese cancer registry, TC has become one of the top ten cancers threatening the health of Chinese residents (3), and ranked the first among women in some provinces, such as Zhejiang province (4). In order to eliminate the influence of annual random change of rates and guarantee the stability of statistical results, we described the epidemic characteristics of TC in China to provide basic information for the control and research of TC, using a 5-year consolidated database pooled during 2008 to 2012.
Materials and methods
Data source
The data of TC incidence and mortality in 2008-2012 were obtained from the National Central Cancer Registry of China (NCCR) which summarized and reported longterm, high-quality incidence, mortality and survival data submitted by local population-based cancer registries. The cancer information was collected by local hospitals,community health centers, the Basic Medical Insurances for urban residents, the new-rural cooperative medical system and so on. The Vital Statistical Database was linked with the cancer incidence database for identifying cases with death certificate only (DCO) and follow-up. By May 1,2018, a total of 135 cancer registries from 31 provinces including 56 urban and 79 rural registries submitted cancer data of 2008-2012. These cancer registries covered a population of 629,333,910 person-years (318,623,600 males and 310,710,310 females). All TC cases were coded according to the International Classification of Diseases for Oncology, 3rd edition (ICD-O-3) and the International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10). Furthermore, each year,the incidence/mortality rate of TC and the data of population during 2003-2007 were acquired from the database of NCCR.
Quality control
The NCCR assessed quality and comparability of data using standard criteria, which were based on “Guideline for Chinese Cancer Registration” and referring to relevant data quality criterion of “Cancer Incidence in Five Continents Volume IX” by International Agency for Research on Cancer (IARC) (5,6). The percentage of cases morphologically verified (MV%), the percentage of cases with DCO (DCO%), mortality to incidence (M/I) ratio as well as percentage of uncertified cancer (UB%) were used to evaluate the completeness, validity and comparability of data quality (1,7). Only datasets meeting defined quality criteria were included in this study. The data quality indicators of MV%, DCO% and M/I ratio were 52.97%,3.97% and 0.83, respectively (8).
Statistical analysis
The pooled data were stratified by area (urban/rural),gender (male/female), and age groups (0-, 1-4, 5-84 by 5 years and 85+ years). We estimated the numbers of new cases and deaths of TC in 2008-2012 in China, as well as a comprehensive overview of cancer incidence, mortality and cumulative risk of developing or dying from cancer before 75 years of age. The incidence and mortality rates per 100,000 person-years were age-standardized using the Chinese population in 2000 and world Segi's population.SAS software (Version 9.2; SAS Institute Inc., Cary, USA)software was used to calculate the incidence and mortality rates. The Joinpoint Regression Analysis Program (Version 4.6.0.0; Statistical Methodology and Applications Branch,Surveillance Research Program, National Cancer Institute,Rockville, USA) was used to calculate annual percentage changes (APCs) and 95% confidence intervals (95% CIs) to quantify temporal trends in incidence overall (9). P<0.05 was considered statistically significant.
Results
Incidence of TC
There was an estimate of 47,550 new TC cases diagnosed in China during 2008-2012, accounting for 2.67% of all new cancer cases. The total crude incidence rate was 7.56/100,000. The crude incidence rate in males was 3.57/100,000, while the rate in females was 11.64/100,000.The age-standardized incidence rates by China population(ASIRC) and by World population (ASIRW) was 6.25/100,000 and 5.52/100,000, respectively. Among the patients aged 0-74 years old, the cumulative incidence rate was 0.53%. The ASIRC in females (9.58/100,000) was 3.21 times as high as that in males (2.98/100,000).
The crude incidence rate in urban areas during 2008-2012 was 9.99/100,000, while that in rural areas was 3.77/100,000. The ASIRC in urban areas (8.12/100,000)was 2.53 times as high as that in rural areas (3.21/100,000).
The crude TC incidence in eastern areas of China during 2008-2012 was 9.03/100,000, while that in middle areas was 4.63/100,000 and that in western areas 2.69/100,000. The ASIRC in eastern areas of China during 2008-2012 was 7.40/100,000, while that in middle areas was 3.96/100,000 and that in western regions 2.28/100,000.Though in different areas, the ASIRC in females was still higher than those in males (Table 1).
Age-specific incidence of TC
TC incidence was relatively low in population under the age of 15. However, the incidence increased dramatically after age of 15 years, then peaked at 14.08/100,000 in the group of 50-54 years and finally decreased sharply after 55 years old. The incidence rate reached the peak value 6.13/100,000 in males aged 55-59 years, while that reached the peak value 22.80/100,000 in females aged 50-54 years.The incidence in females was higher than that in males at all age groups and the incidence in females was nearly three times that in males at the age of 10-59 years. The incidence peaked at the age of 50-54 years in both urban and rural areas. The incidence at all age groups in urban areas was higher than that in rural areas in both males and females. Eastern areas had the highest incidence rate followed by middle and western areas in males aged under the 70-74 years group and in females aged under the 80-84 years group (Figure 1, 2).
Temporal trend of TC incidence between 2003 and 2012
The ASIRC of TC increased dramatically by 4.73 times between 2003 and 2012, from 2.40/100,000 to 13.75/100,000. And TC incidence rates in males increased by 4.95 times from 1.14/100,000 in 2003 to 6.78/100,000 in 2012, while that in females increased by 4.64 times from 3.68/100,000 to 20.75/100,000. The ASIRC in urban areas had an approximately 5-fold increase between 2003 and 2012 from 2.82/100,000 to 15.89/100,000, in which the ASIRC in males and females increased by 4.82-fold and 4.52-fold, respectively. The ASIRC in rural areas had an approximately 4-fold increase between 2003 and 2012 from 1.00/100,000 to 4.92/100,000, in which the ASIRCs in males and females increased by 4.10-fold and 3.88-fold,respectively (Table 2, Figure 3).
Over the past decades during 2003-2012, the temporal trend of the incidence rate of TC in both sexes in China was increasing (APC: 20.04%; 95% CI: 18.13%, 21.99%).In urban areas, the temporal trend of the incidence rate increased by 20.70% per year and in males the rate increased by 20.85% per year and in females the APC was 21.07% (95% CI: 15.57%, 26.83%). In rural areas, theincidence rate of TC increased by 19.26% per year, and in males the rate increased by 19.63% per year and in females the APC was 19.31% (95% CI: 14.77%, 24.03%) (Table 2,Figure 3).

Table 1 Thyroid cancer incidence in China, 2008-2012

Figure 1 Age-specific incidence of thyroid cancer in urban and rural areas in China, 2008-2012.

Figure 2 Age-specific incidence of thyroid cancer in different regions in China, 2008-2012.

Table 2 Temporal trend of thyroid cancer incidence in China, 2003-2012
Mortality rate of TC
It was estimated that about 3,280 cases died from TC in China during 2008-2012, accounting for 0.29% of cancer deaths. The crude mortality rate was 0.52/100,000(0.36/100,000 in males and 0.68/100,000 in females) and it was the twenty-second cause of cancer-related death in overall cancers. The age-standardized mortality rates of Chinese population (ASMRC) and world population(ASMRW) were 0.34/100,000 and 0.32/100,000,respectively. The ASMRC in females (0.42/100,000) was 1.75 times as high as that in males (0.24/100,000). Among the patients aged 0-74 years old, the cumulative mortality rate was 0.04%.
The crude mortality rate in urban areas (0.60/100,000)was higher than that in rural areas (0.40/100,000). The ASMRC in urban areas (0.36/100,000) was 0.29 times higher than that in rural areas (0.28/100,000).

Figure 3 Temporal trend of age-standardized incidence (ASIRC)of thyroid cancer in China, 2003-2012.
The crude TC mortality in eastern areas of China during 2008-2012 was 0.56/100,000, while that in western areas was 0.47/100,000 and that in middle areas 0.43/100,000.After adjusting for age, the gap of the mortality rates between different regions was narrowed, with the highest in western areas and the same in eastern and middle areas.The ASMRC in eastern areas of China during 2008-2012 was 0.33/100,000, while that in middle regions was 0.33/100,000 and that in western regions 0.37/100,000.Though in different areas, the ASMRC in females was still higher than that in males (Table 3).
Age-specific mortality
The mortality rate increased with age in population,reaching the peak of 5.09/100,000 in sub-population aged 85 years or older. Similarly, the male and female mortality rates increased with age, and both reached the peak after 85 years old. The mortality rate in females was higher than that in males at the same age group. The mortality reached the peak of 6.43/100,000 in population at the age group of 85 years or older in urban areas, while that reached the peak of 2.70/100,000 in population at the age group of 80 years or older in rural areas. The male age-specific mortality rate in urban areas was higher than that in rural areas after 45 years old (Figure 4). There was no obvious regional disparity trend of the age-specific mortalities among different regions of China (Figure 5).
Temporal trend of TC mortality between 2003 and 2012
The ASMRC of TC increased slightly between 2003 and 2012, around 0.32/100,000 from 0.26/100,000 to 0.36/100,000. The mortality rates in males increased from0.18/100,000 to 0.31/100,000, while that in females increased from 0.32/100,000 to 0.45/100,000. The ASMRC in urban areas increased between 2003 and 2012 from 0.27/100,000 to 0.37/100,000, while that in rural areas increased from 0.17/100,000 to 0.31/100,000. The ASMRCs in females were higher than that in males in every year and any areas (Table 4, Figure 6).

Table 3 Thyroid cancer mortality in China, 2008-2012
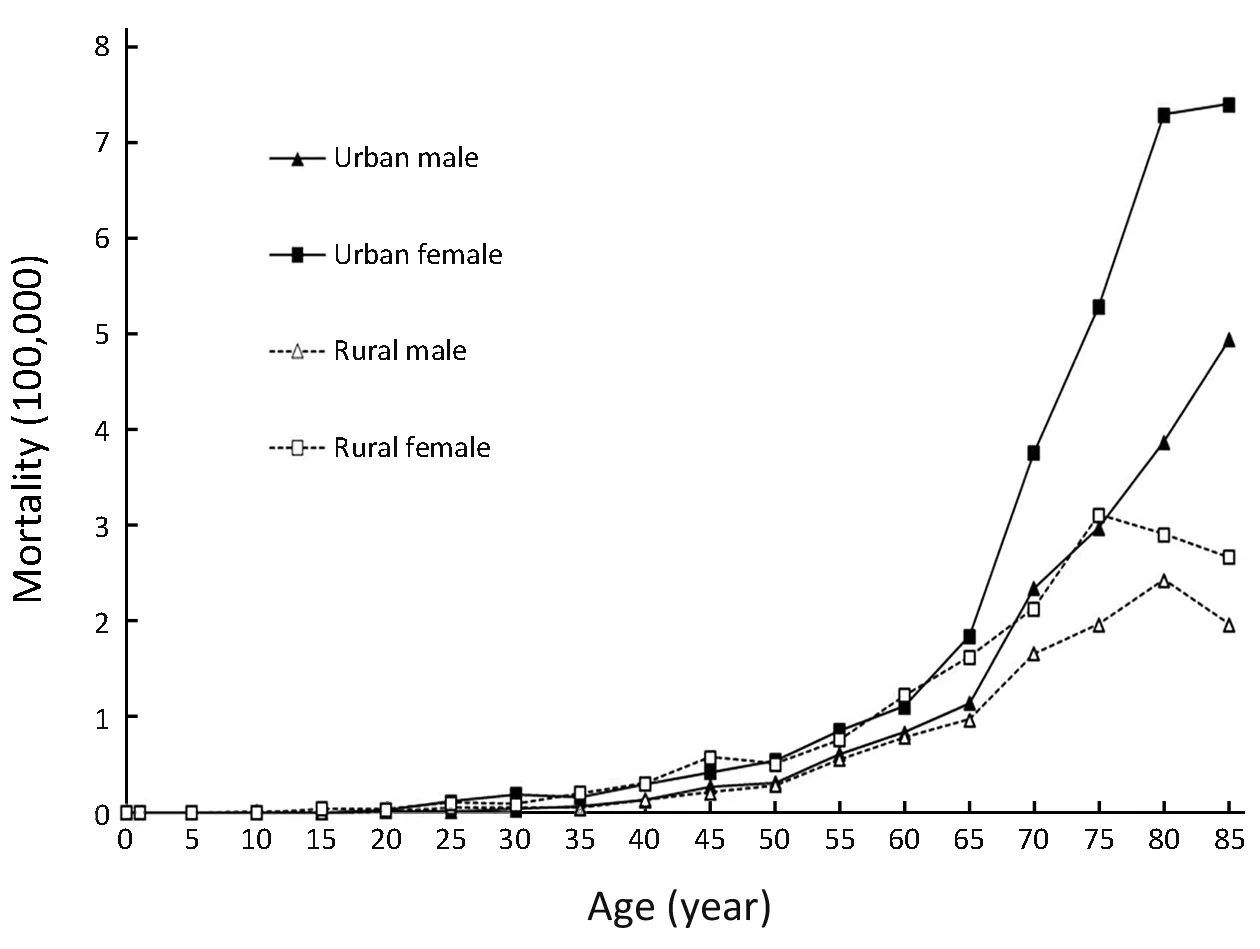
Figure 4 Age-specific mortality of thyroid cancer in urban and rural areas in China, 2008-2012.
Discussion
TC incidence was 7.56/100,000 in China during 2008-2012, ranking the 7th among the incidence rates of malignant tumors. The ASIRW in China was 5.52/100,000, higher than that in the globe of 4.0/100,000 and lower than that in Europe of 7.1/100,000 (2). However,TC mortality has always been relatively low. During 2008-2012, the mortality rate of TC was 0.52/100,000,ranking the 22nd among the mortality rates of malignant tumors in China and the rate was 0.32/100,000 adjusted by the world population, lower than the global average of 0.5/100,000 (2).

Figure 5 Age-specific mortality of thyroid cancer in different regions in China, 2008-2012.
TC incidence increased by 4.73 times from 2.40/100,000 in 2003 to 13.75/100,000 in 2012 with an average annual increase of 20%, while TC mortality only increased slightly, similar to studies in other countries. TC incidence increased from 4.9/100,000 in 1975 to 14.3/100,000 in 2009 in America (10). In South Korea, TC incidence increased by 23.6% annually from 1999 to 2008 in females(11). And there was only a slight increase in TC mortality except in South Korea. In view of the rapid increase in TC incidence worldwide, it is now recognized that the wide application of new imaging examination techniques hasgreatly increased the detection rate of thyroid microcarcinoma, and that excessive examination has also increased the detection rate of TC (12).

Table 4 Temporal trend of thyroid cancer mortality in China, 2003-2012
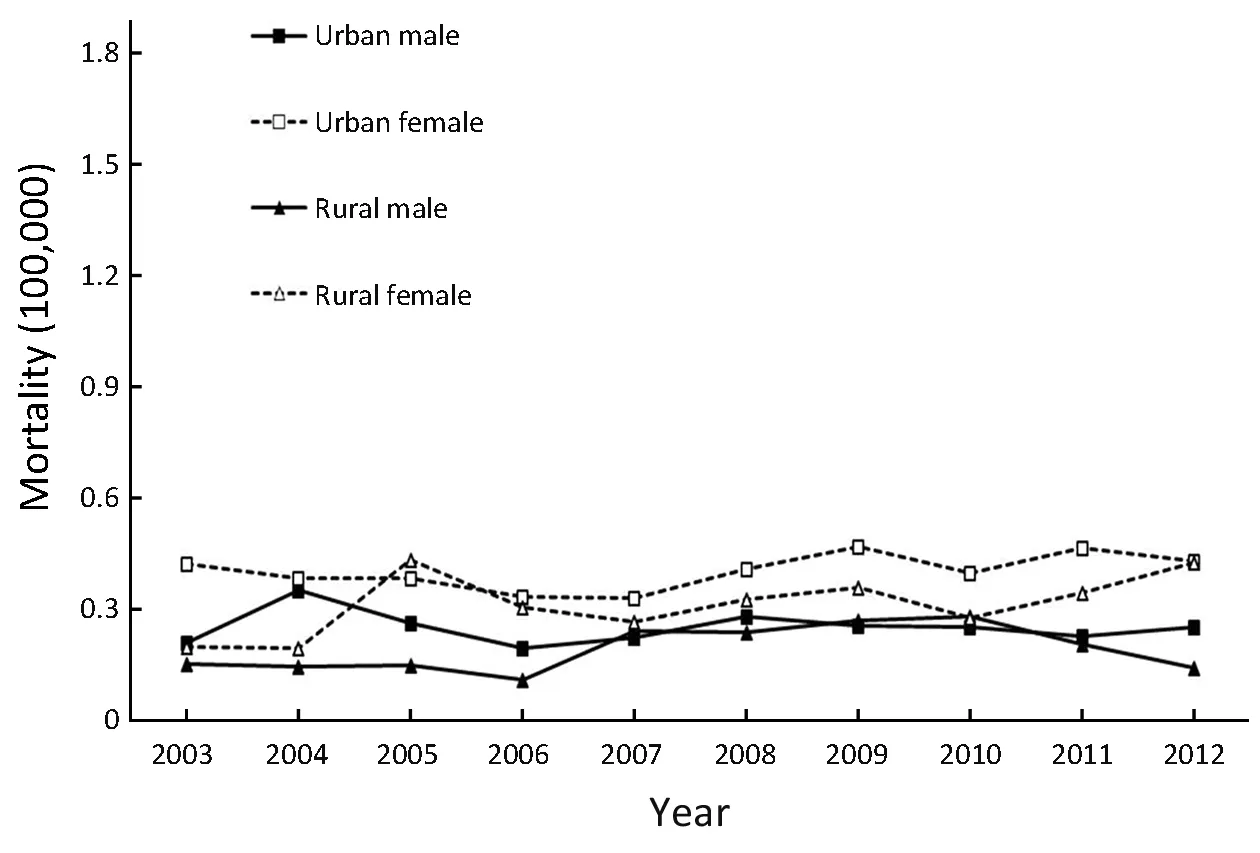
Figure 6 Temporal trend of age-standardized mortality (ASMRC)of thyroid cancer in China, 2003-2012.
Many risk factors have been identified for thyroid carcinoma. TC incidence is closely related to ionizing radiation (13,14), iodine intake (15-17), female hormones(13,18) and family factors. In addition, about 5% of patients with TC have a family history of thyroid carcinoma (12). Body mass index (BMI) is associated with the incidence of TC (19), and mental factors have a great impact on the development of TC by influencing endocrine function of thyroid gland (20).
During 2008-2012, TC incidence in China showed obvious differences in gender, age. The incidence of TC was higher in females than in males in China. The ratio of female to male was 3.21:1 in China, 3.14:1 in urban areas and 3.55:1 in rural areas. Multiple studies have shown that estrogen receptor (ER) is expressed in TC tissues, and estrogen itself may be a carcinogen, and the enhanced 2-hydroxylation in its metabolism is likely to be related to the occurrence of TC (13). The age-specific incidence of TC in Chinese females increased with age, reaching a peak at the age group of 50-54 years which is just right the female menopause. However, TC incidence decreased rapidly after menopause, suggesting that estrogen level plays a role in the development of TC (18).
TC incidence was relatively high in economically developed regions, such as in South Korea ((111.3/100,000 in females, 27.0/100,000 in males in 2010)) (21) and in North America (16.5/100,000), and relatively low in economically underdeveloped regions, such as Africa(1.1/100,000) (2). Our study showed that there was a higher incidence of TC in urban areas than in rural areas. We also found that TC incidence in developed eastern areas was the highest, followed by middle areas and western areas of underdeveloped in China. This is likely to be related to the availability and improvement of imaging examination techniques of thyroid gland in developed regions. In addition, there is a high incidence of TC in eastern coastal areas in China, which suggests that environmental factors such as diet are associated with TC incidence (13). There is a U-shaped relationship between diet iodine intake and the occurrence of thyroid diseases, that is, insufficient or excessive intake can lead to the increase of the incidence of thyroid carcinoma. Excessive iodine intake may be related to the growth of thyroid papillary cancer, and iodine deficiency may be related to the growth of follicular cancer(15-17).
Conclusions
TC showed an increasing dramatically trend of incidence rate in recent years. There are disparities of incidence rate in genders, age groups and different areas. Appropriate targeted prevention, early detection and treatment programs can be carried out to curb the rapid growth trend of TC and control the disease burden.
Acknowledgements
We gratefully acknowledge all the population-based cancer registries for the effort in data collection, data sorting, data verification and database creation. The authors take full responsibility for analyses and interpretation of these cancer registry data.
Footnote
Conflicts of Interest: The authors have no conflicts of interest to declare.
1.Chen W, Sun K, Zheng R, et al. Cancer incidence and mortality in China, 2014. Chin J Cancer Res 2018;30:1-12.
2.Ferlay J, Soerjomataram I, Ervik M, et al.GLOBOCAN 2012: Estimated Cancer Incidence,Mortality and Prevalence Worldwide in 2012 v1.0.IARC CancerBase No. 11. Internatioanl Agency for Research on Cancer, 2013. Available online: http://
Referencesglobocan.iarc.fr/Pages/online.aspx.
3.He J, Chen W. 2015 Chinese Cancer Resgistry Annual Report. Beijing: Tsinghua University Press,2017.
4.Li H, Du L, Zhu C, et al. Analysis of cancer incidence and mortality in Zhejiang Cancer Registries, 2013.Zhongguo Zhong Liu (in Chinese) 2017;26:8-17.
5.Parkin DM. The evolution of the population-based cancer registry. Nat Rev Cancer 2006;6:603-12.
6.Curade MP, Edwards B, Shin HR, et al. Cancer incidence in five continents. Volume IX. Lyon: IARC Sci Publ 2007;No.160.
7.Liu S, Yang L, Yuan Y, et al. Cancer incidence in Beijing, 2014. Chin J Cancer Res 2018;30:13-20.
8.Liu S, Chen Q, Guo L, et al. Incidence and mortality of lung cancer in China, 2008-2012. Chin J Cancer Res 2018;30:580-7.
9.Statistical Research and Applications Branch in National Cancer Institute, USA. Joinpoint software.Available online: https://surveillance.cancer.gov/joinpoint/
10.Davies L, Welch HG. Current thyroid cancer trends in the United States. JAMA Otolaryngol Head Neck Surg 2014;140:317-22.
11.Lee TJ, Kim S, Cho HJ, et al. The incidence of thyroid cancer is affected by the characteristics of a healthcare system. J Korean Med Sci 2012;27:1491-8.
12.Yang L, Wang N. Research advances in the epidemiology of thyroid cancer. Zhuonghua Yu Fang Yi Xue Za Zhi (in Chinese) 2014;48:744-8.
13.Dong F, Zhang B, Shan G. Distribution and risk factors of thyroid cancer in China. Zhongguo Ai Zheng Za Zhi (in Chinese) 2016;26:47-51.
14.Wang JX, Zhang LA, Li BX, et al. Cancer incidence and risk estimation among medical X-ray workers in China, 1950-1995. Health Phys 2002;82:455-66.
15.Yildiz SY, Berkem H, Yuksel BC, et al. The rising trend of papillary carcinoma in thyroidectomies: 14-years of experience in a referral center of Turkey.World J Surg Oncol 2014;12:34.
16.Conzo G, Avenia N, Bellastella G, et al. The role of surgery in the current management of differentiated thyroid cancer. Endocrine 2014;47:380-8.
17.Mishra A, Meherotra R. Head and neck cancer: global burden and regional trends in India. Asian Pac J Cancer Prev 2014;15:537-50.
18.Gong W, HU R, Luo S, et al. Analysis on incidence and mortality characteristics of thyroid cancer during 2007 to 2011 in Zhejiang Province. Zhejiang Yu Fang Yi Xue (in Chinese) 2014;26:433-7.
19.Kitahara CM, Gamborg M, Berrington de González A, et al. Childhood height and body mass index wereassociated with risk of adult thyroid cancer in a large cohort study. Cancer Res 2014;74:235-42.
20.Buchman L, Ashby S, Cannon BB, et al. Psychosocial distress in patients with thyroid cancer. Otolaryngol Head Neck Surg 2015;152:644-9.
21.Kweon SS, Shin MH, Chung IJ, et al. Thyroid cancer is the most common cancer in women, based on the data from population-based cancer registries, South Korea. Jpn J Clin Oncol 2013;43:1039-46.
 Chinese Journal of Cancer Research2019年1期
Chinese Journal of Cancer Research2019年1期
- Chinese Journal of Cancer Research的其它文章
- STIM1 expression is associated with osteosarcoma cell survival
- Prognostic implications of epidermal growth factor receptor variant III expression and nuclear translocation in Chinese human gliomas
- Risk-stratification model to select conversion surgery for advanced gastric cancer patients
- Metastatic patterns and surgical methods for lymph nodes No. 5 and No. 6 in proximal gastric cancer
- Prognostic value of 18F-fluorodeoxyglucose positron emission tomography using Deauville criteria in diffuse large B cell lymphoma treated with autologous hematopoietic stem cell transplantation
- Clinical features and outcomes of diffuse large B-cell lymphoma based on nodal or extranodal primary sites of origin: Analysis of 1,085 WHO classified cases in a single institution in China