
Exploration and practice of general practitioner responsibility system in an urban community of Shanghai
2015-12-06 11:20:57YanWuYanpingZhaoXiaoxiaHuangJunyanWangHuilinXuHualinSu
Yan Wu, Yanping Zhao, Xiaoxia Huang, Junyan Wang, Huilin Xu, Hualin Su
Exploration and practice of general practitioner responsibility system in an urban community of Shanghai
Yan Wu, Yanping Zhao, Xiaoxia Huang, Junyan Wang, Huilin Xu, Hualin Su
Objective:The Minhang district of Shanghai was selected as the subject and its public health management model was investigated.Methods:Minhang became a pilot location for the implementation of the general practitioner responsibility system (GPRS) in 2011. Since then, the management model of public health services in the district has gradually merged with the GPRS through a series of actions: the adjustment of organizations and the coordination mechanism in community public health services, the integration of basic public health services and clinic practice, the establishment of an informationized Internet service platform, comprehensive budgeting management of public health service programs, and performance assessment management of health workers.Results:By the end of 2014, the number of residents who had a contractual relationship with a general practitioner (GP) in Minhang had reached 1.4367 million and all of them had family health records. Compared with 2010, both the rate of maternal management and the rate of children management stayed at high level (≥96%), the rate of hypertension management increased (40.73%vs. 28.70%), the rate of blood pressure control increased (82.13% vs. 77.51%), the incidence of diabetes decreased (21.93% vs. 37.85%), the rate of effective control of blood glucose for diabetic patients increased (82.43% vs. 62.77%), and the rate of child health management increased(99.79% vs. 91.54%).Conclusion:The GPRS has helped to create a better community health environment. However, the development of this system is limited by several factors, including the following: the shortage of GPs, most GPs do not have good public health service skills and a correct public health concept, unclear division of different services, and imperfect department coordination.
General practitioner; Center for Disease Control; Minhang; Shanghai
Introduction
This article is a translation from Chinese.Please refer to reference [1] to access the original source. The general practitioner responsibility system (GPRS) is a security system for the community and takes the family as a unit to provide health services to individuals. This system is based on service commitment and the use of a community health care center as an agent. In 2011, the GPRS started to be implemented in the Minhang district of Shanghai.In 2012, it was upgraded to be a local government project. This project made the general practitioner (GP) be the provider of community public health services. The community health system started to have two functions:providing a basic medical service and providing a basic public health service. This change is an irresistible trend of the development of the GPRS and also ensures the community health service's quality and efficiency [2]. The new guiding ideology of Chinese health reform – "stress should be placed on prevention" – is fully expressed by the GPRS. However, there are some problems in the changing process: not all medical workers realized treatment and prevention should be a single concept; there is a shortage of professional personnel; there are low average public health professional skills; mandatory work is hard to accomplish systematically; and the performance appraisal system is poor. Therefore, how to establish a better organizational structure and improve service content,processes, and the performance evaluation system are becoming problems that need to be addressed urgently. In this study we analyzed the GPRS in Minhang.
Basic information regarding Minhang
Minhang is located in the southwest of Shanghai and covers an area of 371.76 km2. It has three residential districts, nine towns, and one municipal-level industrial zone. Three integrated health care organizations, three specialized hospitals,five health professional institutions, 13 community health service centers, 57 community health service stations, and 97 village clinics are located in this area. Up to the end of 2013,2568 health technicians worked in the community health service centers in this district, including 914 medical practitioners, 141 licensed (assistant) doctors, 1062 registered nurses,200 pharmacists, 114 test technicians, and 137 support workers. The 13 community health service centers employed 403 GPs and 594 medical assistants. Minhang has been rapidly urbanized in recent years. In 2014, the actual population was 2.6047 million and the registered population was 1.0176 million. The number of people who were over sixty years old was 314,100 which accounts for 12.06%, students were 134,700 (5.17%). Life expectancy was 83.46 years. The aged people burden coefficient reached 23.97%. In this district, children, elderly people, people with chronic disease,and pregnant women accounted for large proportions of the population, and these people need extra health support. This means the demand for health services is high. Therefore, it is hard to administer health institutions in this district.
Exploration of the GPRS in community public health services
In 2012, a GPRS service agreement was introduced in Minhang. Residents could choose a GP they like and enter into a contractual relationship with him/her. The GPRS stipulates one GP per 600 family units or one GP per 2500 residents of this district. To adapt to the new system, optimization of the management of community public health services, service content, and performance assessment system is indispensable.
The management of the GPRS in community public health needs to be improved
Organizational structure:The community GPRS was primarily constructed but further development was needed. The major institutions of this system are the Public Health Management Center (PHMC), the GP Management Center (GPMC),and the Public Health Outsourcing Management Center (PHOMC). Additionally, a GP assistant system was established whereby one GP was accompanied by one to three assistants.See Table 1 for more details.
Collaborative mechanism:The community PHMC was administered by the local Health and Family Planning Commission (HFPC) and local public health professional institutions such as the Center for Disease Control, the Woman and Child Care Center, the Mental Illness Prevention Center, and the Dental Disease Prevention Center. The PHMC received tasks, training, guidance, quality control, and performance assessment from them. Then tasks were handed over to the GPMC. GP teams received tasks from the GPMC and also have the right to outsource the workload that they cannot handle to the PHOMC. However, GP teams were responsible for the quality control and evaluation of this part of the work. The PHOMC could also take the tasks which cannot be done by GP teams, such as disease surveillance and workplace intervention. The PHMC provides training, guidance, quality control,and performance assessment to GP teams and the PHOMC.The results of the assessments for GP teams were fed back to the GPMC directly, and for the PHOMC they were fed back to the PHMC. The performance salary was decided by the assessment result (Fig. 1).
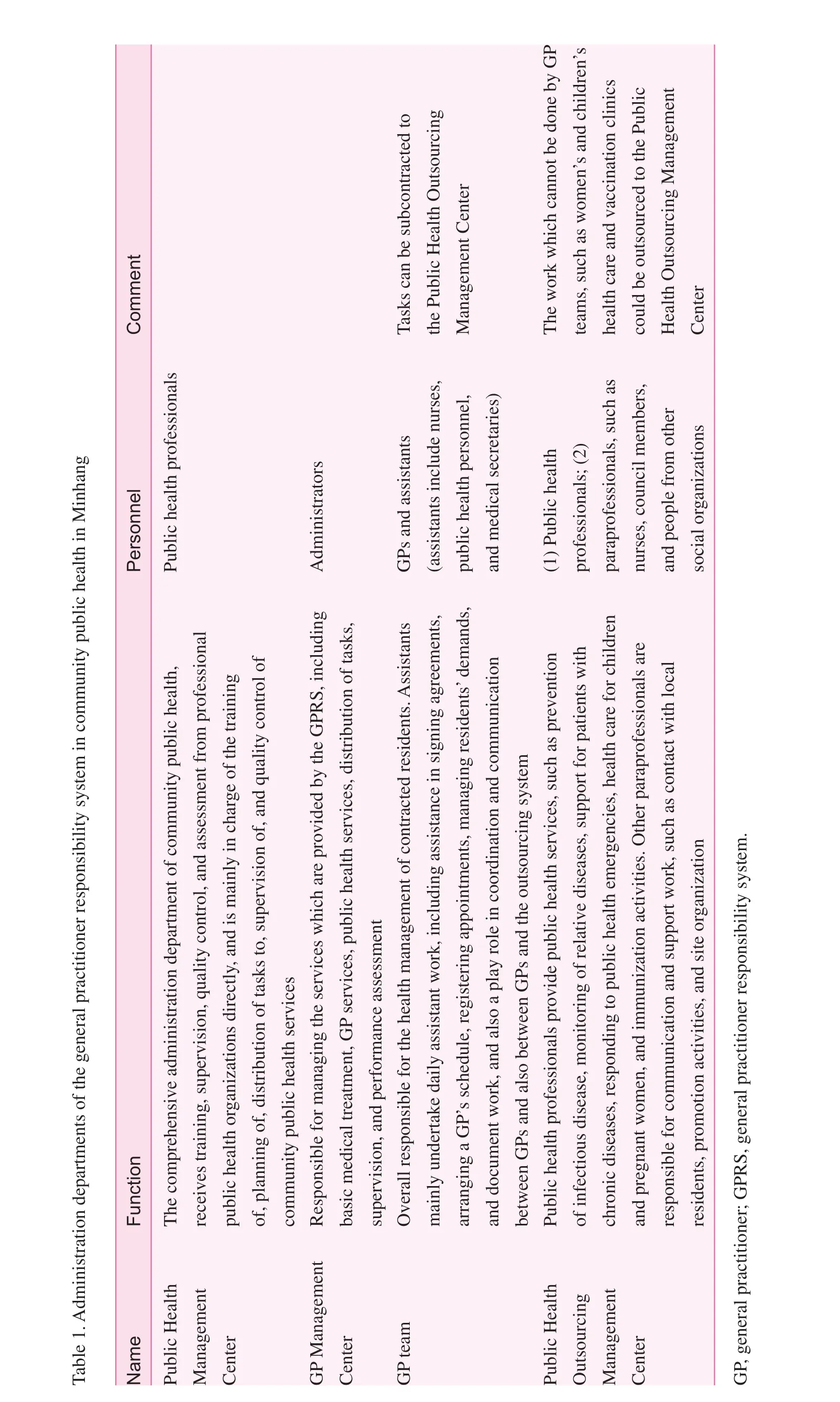
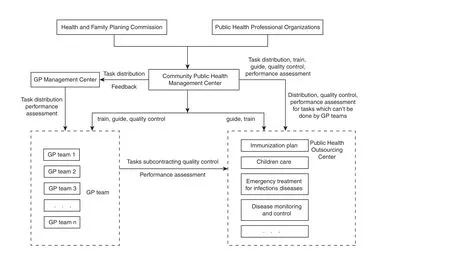
Fig. 1. Collaborative mechanism of the community health care system in Minhang. GP, general practitioner.
Basic public health services which are closely related to clinical practice are provided
In the past, GPs in China provided only basic medical services, such as diagnosis and treatment of disease. In this pilot study, disease prevention, rehabilitation, maintenance of health records, and health promotion were all included in the GPs' daily work [3]. "Guidance for the Promotion of GP Responsibility System," which was published by the Shanghai HFPC indicated that the purpose of implementing the GP system is to maintain and improve residents' health.It is the GP's responsibility to provide basic public health services which are closely related to clinical practice [4].In 2012, the HFPC in Minhang created "Working Plan for Minhang GP Services." According to this working plan, 10 health services were provided to residents who signed health contracts: basic medical treatment, public health services,health management for special groups, a family sickbed, a clinical two-way referral pathway, etc. Additionally, six public health services were required to be provided to local residents: (1) establishment and management of local residents'electronic health records; (2) health management for patients with diabetes and hypertension; (3) health management for people at high risk of lung cancer, liver cancer, stomach cancer, colorectal cancer, breast cancer, and cervical cancer;(5) the carrying out of health education activities and community health counseling; and (6) free health checks for certain people.
The transition of the public health services model in Minhang is a gradual progress. The first step is to make GP teams be responsible for the management of electronic health records, health management for people with chronic diseases such as hypertension and diabetes, early detection of cancer,and health management for special groups.
Adding health services which are closely related to clinical practice to GPs' daily work could significantly enhance residents' trust in the GPRS. On the other hand, it could also improve the contiguity and comprehensive character of the community health service.
Constructing an Internet information platform
Minhang started to build an Internet information platform and apply it in the transition of the GP service model in 2006. The establishment of a health information network and an information exchange platform has already been completed [5].GPs can use the GP management platform and the GP support platform to perform part of their daily work. The main functions of the GP management platform are the management of electronic health records and electronic medical records.Moreover, budgeting, implementation of programs, service subcontracting, quality control, and review of performance can also be achieved through the use of this platform. In addition,the GP support platform can help GPs achieve another 16 tasks:management of family archives, basic medical services, family sickbed, medical assistants, nursing center, rehabilitation center, chronic disease management, early detection of cancer,health for pregnant women, health for children, immunization,health education, epidemic disease, quality monitoring, residents' health, and 3G cell phone GP. Information technology has significantly increased the management efficiency of GPs'daily work, especially in service subcontracting, quality control, assessment, and performance management.
Pursuing comprehensive budget management
Comprehensive budget management is a detailed projection about all estimated income and expenses. It always starts with an evaluation of the organization itself. Rational application of resources is its purpose. It could help in the coordination and organization of activities, and the predetermined plan development goals can be completed in a timely manner.
Comprehensive budget management is becoming one of the prerequisites for constantly expanding and sustainable development. A large number of organizations are using it to standardize finance management and improve internal control mechanisms.Its effect and driving force are drawing increasing attention [6].
In 2012, a new performance budgeting mechanism was implemented in Minhang. The local government took the opportunity of having general control of basic public health funding to introduce a new policy: every resident could have access to government subsidization of public health services –60–65 yuan annually. The total expected expenditure is calculated as the unit cost (60–65 yuan) times the quality times divided by the quantity. The final results are allocated after a second comprehensive check. Each year, if the ratio between actual spending and expected costs is 95% or more and 105%or less, this means the actual cost of public health services reached the previous expectation. If the ratio is less than 95%,the fund for the project at the upper level will decrease by 1%.If the ratio is greater than 105%, the first 5% is paid fully, but 20% of the second 5% is removed. Only 40% of the third 5%will be paid, and so on. In the budget system, the budget plan is made granularly down to each GP team. The preliminary budget is based on the expected expenditure of each department. After research and debate, the HFPC will adjust the budget plan before its final approval. However, funds will not be issued at one time. Assessments are held each quarter by the professional organizations; merit pay is determined by the results of these assessments. The advantage of comprehensive budgeting management is that the budget is set on the basis of the minimum accounting units. This had helped to strengthen the functions of GP teams. Additionally, as a public welfare service, its fairness was well developed.
Performance assessment system was implemented for GPs, medical assistants, and public health workers
There are two components of the performance assessment system: performance assessment for basic charges and performance assessment for service quantity. The merit pay consists of two parts: the first is calculated as the basic cost for each person times the total number of people times the rate for each service times the quality of each service times the occupancy of medical resources times the satisfaction of community residents; the second is calculated as the sum of the product of the service quality and the cost for each service,times the quality of the services times the occupancy of medical resources times the satisfaction of community residents.Medical workers receive the first part of the merit pay annually and the second part monthly. The performance assessment system ensures that health service quality, quantity, and residents' satisfaction are related to GPs' salaries. This initiative significantly increased medical workers' enthusiasm. It plays a crucial role in the quality and quantity of improvements in community public health services.
Initial effects (2010–2014)
Build electronic health records for local residents
Up to 2014, 1.4367 million local residents had established a contractual relationships with local GPs. All of them already had their own electronic health record. GPs could use the Internet information platform to collect health information,health risk factors, and medical records for residents and their families. This provides information support for the health management of future residents and other relevant services.
Health services for special groups improved gradually
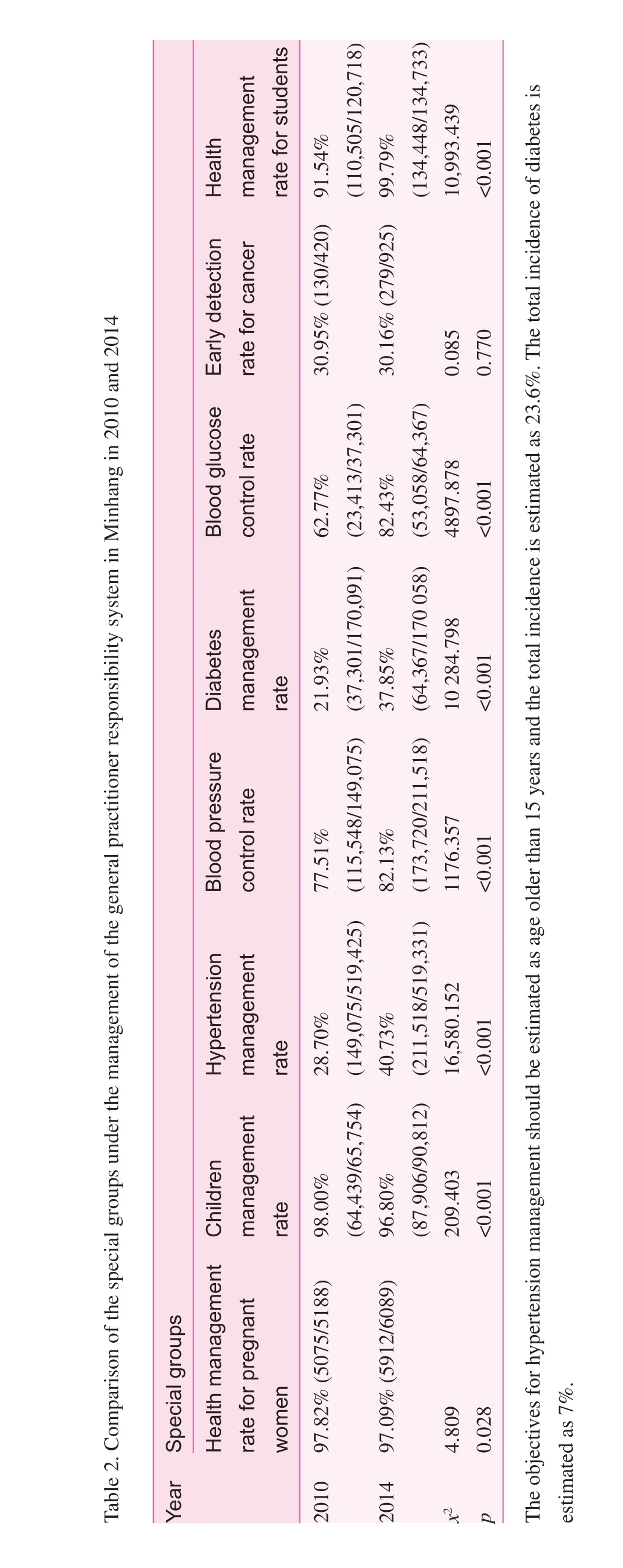
Women's and children's health:Compared with 2010, the health management rate for pregnant women and that for children dropped slightly (p<0.05, Table 2). This may due to the increased immigrant population. It is hard to manage pregnant women and children in a changing population.
Management of chronic disease:The new service model requires GP teams to provide outpatient services, group medical visits, and follow-up examinations to local residents who have chronic disease directly. There were obvious improvements in service efficiency and effect. Compared with 2010,the rates of hypertension management and diabetes management increased (p<0.001, Table 2). Before 2010, activities for the early detection of cancer were launched. Through outpatient clinics, health examinations, and health education, which are mainly provided by GP teams, the detection rate of stomach cancer, colorectal cancer, liver cancer, lung cancer, cervical cancer, and breast cancer has remained above 30%.
Health management for children:Since 2010, each childcare facility, primary school, and high school in Minhang has been staffed by one GP. With the help of an electronic information platform, the establishment and maintenance of an electronic health record for each child, the monitoring and management of common diseases for children, health education,and health promotion have already been achieved. The health management rate for children increased from 91.94% in 2010 to 99.79% in 2014 (p<0.001, Table 2).
Discussion
With the development of community health services, the 'six in one' public health service model has operated for many years.It has played an important role in community public health services, especially in control and prevention of infectious diseases, immunization programs, health education, and occupational and environmental health promotion. However, with population aging and the changing of the disease spectrum,the incidence of chronic diseases such as hypertension, diabetes, and cancer tends to rise. This is one important factor that affects population health and quality of life and is also the reason for an increasing health burden. The traditional community public health management model fails to take into account the heavy burden of current community health work, especially in chronic disease screening, treatment, follow-up management,and health education. The Chinese health reform makes the transition of the GP service system inevitable. This transition results in a regrouping of the original management framework and professional staff structure. The service manager, provider,content, and model all need to be adjusted. Experience has been accumulated but further exploration is needed.
A better coordination mechanism is needed
Shanghai has six major public health service projects. Basic public health services have 12 categories and 42 subcategories. At present it is difficult for GP teams to perform those tasks fully alone. This means strong support from other relevant departments is necessary. The efficiency and quality of public health services depend on the coordination mechanism between relevant departments. The GPMC, PHOMC,and PHOC were created to exercise corresponding functions.However, lack of relevant regulatory documents and overlapping functions have made it clear that the coordination mechanism should be further improved.
Shortage of GPs, poor service skills, and incomplete conceptual change are the main limiting conditions
There are 403 GPs working in Minhang. According to the standard that there should be one GP per 600 households or one GP per 2500 residents, Minhang still needs another 1300 GPs.The shortage limits the development of the GPRS. Moreover,as the direct service provider, GP teams need to thoroughly change the traditional concept and actively try to adapt to the new service model. According to an investigation of GPs in Shanghai, only 26% of GPs believed that public health services should be provided by them [7]. Most GPs are still used to the traditional service model (treatment of diseases and prevention of diseases were done by different departments) and do not have enough initiative for the new service system.
Additionally, lack of relevant public health service knowledge also limits the development of the GPRS. Most GPs majored in clinical medicine. They have limited experience and knowledge of public health services [8]. How to train them to improve their service abilities is one of the most significant problems [9].
The public health service programs should be planed more scientifically and reasonably
The services which should be provided by the GP team should be defined more clearly. After many years of exploration and development, tremendous progress has been made in integrating community public health services and GP systems. However, a large number of GPs are still not clear of their duties. The vague definition acts as a barrier in the implementation of the GPRS[10]. Otherwise, GPs cannot complete some mandatory work;for example, perform a multitude of monitoring tasks. How to assign tasks clearly is becoming a top priority. Residents should know what should be done by GP, what should be done by the outsourcing team, and what should be done by experienced specialists. Additionally, there should be more publicity to help local residents understand and accept public health services [11].
Comprehensive budgeting management and the Internet information platform provide reasons and technology support for the development of the GPRS
Information platforms help to record the results of performance assessment in an accurate and timely fashion. The integration of comprehensive budget management and performance management promotes and stimulates the development of the GPRS [12]. The real-time collection of performance appraisal data has ensured the data are real, accurate, and timely. This has helped to make the performance assessment fair and equitable and also to stimulate work enthusiasm of community health workers. However, some GPs prefer a higher-benefit, less demand, and low service quantity medical service. Therefore, how to use comprehensive budgeting management to improve the public health service system and make GPs focus not only on the service which generates high income is becoming more and more important. Making local residents really enjoy the benefits of GP system reform is the ultimate goal.
Conflict of interest
The authors declare no conflict of interest.
Funding
General program of Shanghai Health and Family Planning Committee; Shanghai Hospital Management Research Foundation Bureau level topic (2014032) – Research for General Practitioner Responsibility System, Outsourcing of Public Health Service and Service Coordination Mechanism.
1. Wu Y, Zhao YP, Huang XX, Wang JY, Xu HL, Su HL. Exploration and practice of general practitioner responsibility system in an urban community of Shanghai. Chin Gen Pract 2015;18(13):1504–9. In Chinese.
2. Xiao F, Wu XL, Zhao DY. Family doctor responsibility system:new exploration of basic health service model. China Mark 2012;19(29):84–90. In Chinese.
3. Wu HY, Zhang WD, Wu Q, Li P. Management of suburban community health services within a family doctor-based community healthcare system. Chin Gen Pract 2014;17(1):22–4. In Chinese.
4. Shanghai Health. Shanghai: guidance for popularizing family doctor system in Shanghai. Shanghai Health and Family Planning Commission. Available from: http://www.hs.sh.cn/website/b/103321.shtml.
5. Yang JL, Jin L, He ML, Bao Y. The role and significance of informatization in family doctor system. Chin Gen Pract 2014;20(17):2409–11. In Chinese.
6. Su YM. Application of comprehensive budgeting management in medical units. Mod Med J China 2013;11(15):95–6.In Chinese.
7. Bao Y, Du XL, Zhang A, Liang Y, Xu T. Cognitive analysis and policy advice for family doctors in Shanghai – based on family doctor system. Chin Gen Pract 2012;10(5):665–6. In Chinese.
8. Xu HP, Zhang J. Application and exploration of family doctor system in community public health service. Jiangsu Health Care 2013;15(1):36–7. In Chinese.
9. Gao F, Jin HL, Yu HD, Wang YQ, Wang LL. Investigation and analysis on the demands of family doctor public health services in the residents in suburb of Shanghai. Chin Rural Health Serv Adm 2013;29(33):280–2. In Chinese.
10. Tang Y, Huang FP. Policy recommendations for the development of Shanghai family doctor system. Chin Health Resour 2012;15(5):417. In Chinese.
11. Sun L, Zang LZ, Zhang P, Zhao HL, Zhao WY, Tao AJ, et al.Survey on the basic health conditions of residents signing with general practitioners in Huacao Town of Minhang District. Chin J Dis Control Prev 2012;16(8):731–2. In Chinese.
12. Tan LL, Jin L, Zhang JW, Ni HJ, Yang JL, Bao Y. The framework construction of performance evaluation indexes in family doctor system. Chin Gen Pract 2014;31(17):3673–8. In Chinese.
Center for Disease Control, Minhang, Shanghai 201105, China
Yanping Zhao, BSc Center for Disease Control, Minhang, Shanghai 201105, China
E-mail: zhaoyanping63@yeah.net
15 August 2015;
Accepted 16 October 2015
 Family Medicine and Community Health2015年4期
Family Medicine and Community Health2015年4期
- Family Medicine and Community Health的其它文章
- Current situation of AIDS prevention and control with traditional Chinese medicine and relevant policies in China
- A new paradigm for assessment of infant feeding deviation
- Family structure and support for the oldest old: A cross-sectional study in Dujiangyan, China
- Guest Editors' Prof le
- China's General Practice Conference highlights review
- The role of a community health service in the prevention of violence against women