
Family structure and support for the oldest old: A cross-sectional study in Dujiangyan, China
2015-12-06 11:20:56XiaohuiRenHongdaoMengChaojieLiuJinhuiWuBirongDongNingxiuLi
Xiaohui Ren, Hongdao Meng, Chaojie Liu, Jinhui Wu, Birong Dong, Ningxiu Li
1. Department of Health and Social Behavior, West China School of Public Health, Sichuan University, Sichuan, China
2. School of Aging Studies, University of South Florida, FL,USA
3. School of Public Health, La Trobe University, Bundoora,VIC, Australia
4. School of Health Management, Hubei University of Chinese Medicine, Hubei, China
5. Department of Geriatrics,West China Hospital, Sichuan University, Sichuan, China
Family structure and support for the oldest old: A cross-sectional study in Dujiangyan, China
Xiaohui Ren1, Hongdao Meng2, Chaojie Liu3,4, Jinhui Wu5, Birong Dong5, Ningxiu Li1
1. Department of Health and Social Behavior, West China School of Public Health, Sichuan University, Sichuan, China
2. School of Aging Studies, University of South Florida, FL,USA
3. School of Public Health, La Trobe University, Bundoora,VIC, Australia
4. School of Health Management, Hubei University of Chinese Medicine, Hubei, China
5. Department of Geriatrics,West China Hospital, Sichuan University, Sichuan, China
Objective:In China, adult children have traditionally provided support for their aged parents.This model of care is increasingly challenged by the decline of the extended family. Recently,China's decades-long one-child policy has eased. We examine the association of family size and composition with family support for nonagenarians and centenarians.Methods:Data were obtained through a questionnaire survey of 619 nonagenarians and centenarians in Dujiangyan and were analyzed by chi-square tests, Studentttests, and multivariate logistic regression models.Results:This study revealed that an increased number of offspring might provide financial support for older people, but this does not necessarily translate into physical and emotional care.Conclusion:It is clear that although alternative sources of support for older people are increasingly needed, in China the family will continue to play an important role in supporting older people.
Oldest old; family support; family structure; China
Introduction
The average age of the population in most nations is increasing: the number of 'oldest old'(≥80 years) exceeds the growth of the general aged population (≥60 years). Currently, the proportion of the oldest old as a subset of the aged population is about 14%, and is expected to reach 20% by 2050. In 2012 there were 343,000 centenarians globally, and by 2050 this will increase to 3.2 million [1]. China is the largest contributor: the number of people aged 80 years or over will reach 101 million in 2050,compared with 18 million in 2009, which will account for 25.6% of the world's population aged 80 years or over [2].
Although increased longevity is a testament to the improvements of health status of the Chinese people, any country with an increasing average age and an elderly population can anticipate societal challenges. Some 24% of aged Chinese experience certain degrees of disability [e.g.,instrumental activities of daily living (IADL)] and require regular supportive care [3]. Those of very advanced age are likelier to have disabilities and medical conditions, have poorer functioning in activities of daily living (ADL), and often need the greatest amount of support [4, 5].
Traditionally, adult children have provided support for their aged parents in China [6, 7].The family has always been the most important source of support for the aged, especially for those older than 80 years or who are frail or disabled [8, 9]. Some researchers believe the Chinese family-based aged care support is compatible with traditional Chinese culture: filial piety is a core Confucian value, which continues to influence and encourage intergenerational support despite the significant changes in society and in particular the economy over recent decades [10]. Those older than 80 years generally receive more support than others[11, 12].
However, the one-child family planning policy, implemented since the 1970s, has indelibly changed the family structure of China [13]. The total fertility rate in China fell from 5.81 live births per woman in 1970 to 1.68 in 2001 [14].If the current fertility trend continues, the number of workingage persons for every single elderly person is anticipated to reduce from 5.6 in 2010 to 1.6 in 2050 [15].
Chinese culture stresses a son's responsibility for supporting his parents in their old age, whereas the role of a daughter is attached to her husband as a wife, who is expected to assist her husband with his role as a son. Core cultural values such as these create concern and distress among those families without a son, especially in rural China, which may explain an increasing demand for relaxation of the family planning policy in recent years [16, 17].
Debates still exist in the literature with respect to the association between 'family size and structure' and aged care support. Zimmer and Kwong [18] conclude there is a direct proportional relationship between the increased probability of instrumental and financial support for older people and the number of surviving offspring. Research suggests that in China the likelihood and amount of financial support available to older people is associated with the number of living adult children [12], especially with the number of living sons[19]. Meanwhile, sick older people often depend on their adult daughters for emotional care [19, 20]. However, several other studies argue that the number of living children is associated neither with the availability of support nor with intensity of care for older people [21, 22].
It could be thefunctionof a family that is more important for the family-based aged care support. We acknowledge that assessment measurements of family support differ considerably. In some cases, they measure ceremonial giving or even cursory support, not necessarily appropriate response to the actual needs of older people [23, 24].
There is a paucity in the literature documenting the needs of nonagenarians and centenarians in terms of family support. Most existing studies recruited participants in their 60s.Although those older people who are still young can offer reciprocal services (such as child care for grandchildren),nonagenarians and centenarians can often offer very little for others, and consequently may be more sensitive to the influence of reductions in family size and changes in family structure. Some researchers believe that decreased family size may have a greater impact on the oldest old than on others [18, 25].Therefore, a study focusing on nonagenarians and centenarians can provide a unique insight into the role of the family in aged care.
We attempted to answer three questions using a large cross-sectional survey database established in Dujiangyan in China, with 619 nonagenarian and centenarian participants:
? whether a larger family facilitates improved supportive care of older people;
? whether gender expectations and cultural norms influence the support for aged parents; and
? whether the size and structure of the family are related to the type of family support.
Methods
Research setting
The research data used for this study were collected in Dujiangyan (local population of 657,900 in 2010), a satellite city of Chengdu, the capital of Sichuan province (southwest China). The local population has low levels of mobility.In 2010, there was a small net loss of population in the area:7.83% of the total population moved to the area and 8.02%moved away to other localities. These rates are very low compared with those in Chengdu in general (27.03% settling and 18.62% departing). The economic development of Dujiangyan ranks in the middle of the range of all cities in China, with aper capitadisposable income in 2011 of RMB 16,193 in urban areas and RMB 8645 in rural areas [26, 27].
The aged population of Dujiangyan is rapidly growing.It has a high proportion of nonagenarians and centenarians:2.3% of the population were older than 90 years in 2005,which rose to 2.5% in 2010, almost twice as high as the national average (1.5%) [28, 29].
Participants
Data for this research came from the Project of Longevity and Aging Study (PLAS) conducted in Dujiangyan in 2005 [30].All participants were aged 90 years or older (confirmed by the local government). The PLAS was approved by the Research Ethics Committee of Sichuan University. Written informed consent was obtained from the participants or the family members on behalf the participants.
In Dujiangyan, most households (86.35%) have only one child; however, households with a resident nonagenarian or centenarian are likelier to have a dispersed family and family structure, which provided a good opportunity for us to examine the relationship between family structure (number and sex of children) and family support. People older than 90 years are likelier to be widowed, minimizing the confounding influence of spouses who are usually the primary means of family support.
The local statistics bureau in Dujiangyan identified 1401 old persons aged 90 years or older in 2005. The PLAS investigators interviewed 875 persons aged 90 years or older across 21 townships using a structured questionnaire. Only those able to complete a 30-min face-to-face interview were eligible to participate in the study, and they were usually interviewed in the presence of at least one family member. Interviews were arranged either in a public place (such as a hospital or school)or in the homes of the participants. The interviewers were all local professionals, able to communicate with the participants in their local dialect.
The interviewers had medical backgrounds. They assessed the cognitive function of the participants using the 30-item Mini-Mental State Evaluation (MMSE). Some 233 respondents deemed to have poor cognitive functions – that is, below the cut-off points (see later for the details) – were excluded from this study. An additional 23 respondents were excluded because they reported having no living children at the time of the study. This resulted in a final sample of 619, representing 71% of the respondents and 44% of the entire nonagenarian and centenarian population of Dujiangyang.
Measures
Family supportwas defined as physical care, financial support,and emotional care provided by the adult children to their old parents. Physical care was examined with the following question: "Do your children assist you with your daily activities?"Financial support was explored with the following question:"Do you depend on financial support from your children?"Emotional care was investigated with the following question:"Do your children often talk to you?" The answers to all of those questions were recorded with dichotomous responses:yes or no.
Family structurewas categorized according to the number and composition of adult children, and grouped into five categories: family with one son, family with one daughter, family with two or more sons, family with two or more daughters, and family with both sons and daughters.
Previous research has demonstrated that family support from adult children is also determined by other factors, including the needs of older people, the satisfaction with family life,the living arrangement, and the support available from other sources [18, 31–33].
Health needsof the respondents were measured by the ADL and the IADL [34, 35]. The ADL and IADL scores were added for the purpose of analysis [36]. A higher score indicates poorer physical functioning. Cognitive ability of the respondents was measured by the MMSE [37]. The MMSE scores range from 0 to 30. A higher score indicates better cognitive ability. Because educational attainment has been shown to affect MMSE scores in the Chinese population, for the determination of poor cognitive functioning, we applied a cut-off point of 10 for the illiterate and 13 for others as recommended by Zhang et al. [38] and Dong et al. [39].
The living arrangements of the respondentswere investigated with the following question: "Whom do your reside with?" The responses were as follows: children, no one, in institutional care, others.Family satisfactionwas investigated by the following question: "Are you satisfied with your current family life?" The responses were as follows: highly satisfied,satisfied, moderately satisfied, not satisfied.
Sociodemographic characteristicsmeasured in this study included age, sex, marital status, educational attainment,occupation (before retirement), religious belief (yes or no),residency (urban vs. rural), and annual household incomeper capita.
We did not directly measure support from a source other than a child because such support was rare and usually equally distributed within a community. Indeed, fewer than 9% of older people Chinese had ever received any institutional support from a source that was not a child in the 1990s: the intent of such support is fundamentally to assist those who are childless [18]. This may be compounded by distributive inequalities of aged care resources and services across communities in China [18, 33]. Consequently, we used residency (urban vs. rural) and previous occupation (i.e., before retirement) as proxy indicators of support from communities.
Statistical analysis
Our survey revealed that family support was available to the nonagenarian and centenarian participants regardless of their physical and financial conditions. Therefore, the analyses were not restricted to those with functional limitations.
Family support (physical care, financial support, and emotional care) served as dependent variables in the analyses. The associations between family support and independent variables, including family structure, family satisfaction, health needs, and sociodemographic characteristics, were determined through chi-square tests (Fisher exact tests if appropriate) for categorical variables (such as sex) or Studentttests for continuous variables (such as the MMSE score).
We performed multivariate logistic regression analyses to determine whether the family structure is associated with family support when other influencing variables are controlled for.Collinearity of independent variables can seriously jeopardize the predictive ability of a regression model [40]; however, no significant collinearity among the independent variables was found in this study.
All statistical analyses were conducted with SPSS( version 18).
Results
Respondent characteristics
The respondents had an average age of 95.3 years (range 90–106 years) – 65.4% of the respondents were women – and had lived in their local community for an average of 87.8 years,with 84.2% spending more than 80 years in their community. Almost 91% resided in rural areas. Most were illiterate(70.4%) and engaged in farming (85.9%) before retirement.Only 12% of the respondents had a living spouse. Fewer than one quarter (24.1%) admitted having a religious belief: those that did were predominantly women (79.2%) and expressed their faith as Buddhist. Only 24.4% of the respondents were satisfied with their household income. Less than half of the respondents (48.1%) expressed high satisfaction with their family life (Table 1).
Family structure
The respondents had on average 3.5 living children, of whom 1.8 were sons and 1.7 were daughters. The vast majority (85%)resided with their children, 7.1% lived alone, and 0.5% lived in institutional care.
Family support
Approximately 27% of the respondents were completely independent, more than 63% received physical care from their children, 4.2% received physical care from their grandchildren. In terms of financial independence, 84.2% were financially supported by their adult children, and 5.3% stated their only source of income was a pension. Men were likelier than women to depend on pensions (12.6% vs. 1.5%,p<0.01). In terms of interaction, 65.1% stated their adult children often talk to them.
Determinants of family support
The bivariate analyses identified sex, marital status, religious belief, community support, physical and mental health, family size, family structure, living arrangement, and family satisfaction as determinants of family support from children (Table 2).
Family structure remained a significant factor predicting financial support after all other relevant variables had been controlled for in the logistic regression models (Table 3). Those respondents having two or more sons and having both sons and daughters had a higher probability of receiving financial support than those with only one son (odds ratio 8.29,p<0.01 vs. odds ratio 2.39,p<0.05). There were no significant differences in financial support between those respondents with only one son and those with one or more daughters. Havingmore children, regardless of sex, was not associated with physical care and emotional care. The greatest predictor of physical care was the living arrangements. Those respondents residing with their children were likelier to receive physical care from their children (odd ratio 8.15,p<0.01).

Table 1. Characteristics of respondents (n=619)
The respondents who expressed dissatisfaction with their family life were less likely to obtain financial care and emotional care than those highly satisfied with their family life(odds ratio 0.27,p<0.01 vs. odds ratio 0.29,p<0.01). Family satisfaction did not have a significant association with physical care support from adult children.
Health needs were associated with family support. Those respondents having a higher ADL/IADL score were slightly likelier to receive physical care (odds ratio 1.06,p<0.01).
The two proxy indicators of community support were significant determinants of financial support. Rural respondents and those who engaged in farming were likelier to have financial support from their children (odds ratio 2.31,p<0.05 vs.odds ratio 3.75,p<0.01). Neither proxy indicator was a signifi-cant predictor of physical care and emotional care.
Female respondents and those with a living spouse were less likely to receive physical care from their adult children.Respondents reporting a religious belief were less likely to obtain financial support from their children.
Discussion
The immediate family unit is the major source of support for Chinese nonagenarians and centenarians in Dujiangyan. Our study demonstrated that family size and the sex of adult children are associated with the provision of financial support for nonagenarians and centenarians.
Having more sons increases the chances of nonagenarians and centenarians receiving financial support. This finding is consistent with the findings of studies conducted elsewhere in China [18, 19, 41]. Older people in China retain a strong belief and expectations according to the traditional role of the son [41].
Our study did not show family size and the sex of adult children are associated with the provision of physical support for nonagenarians and centenarians. Because most of them reside with one of their children's family, the roles of other children in physical care may have become weak [18].
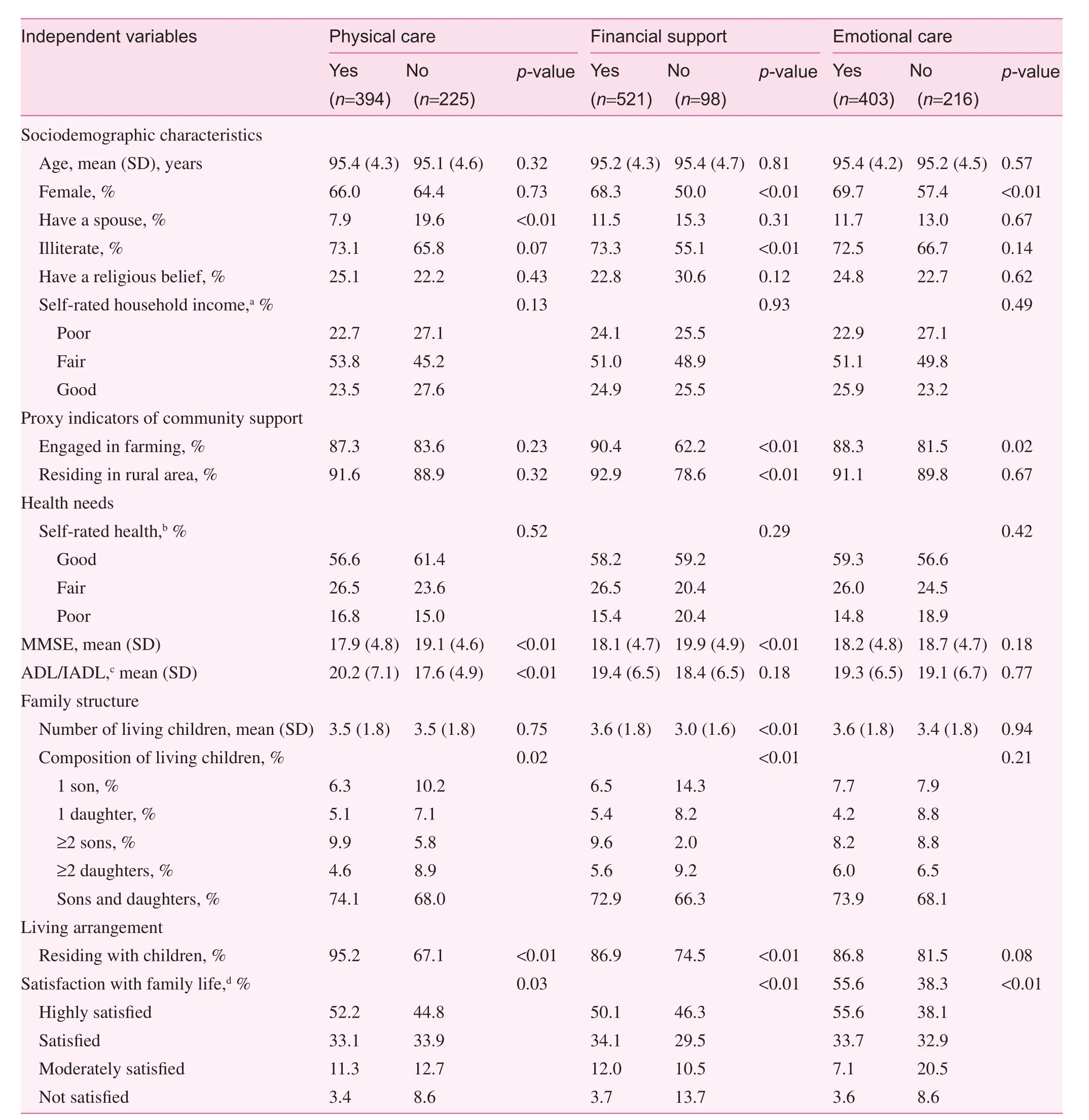
Table 2. Factors associated with family support from the children: bivariate analyses
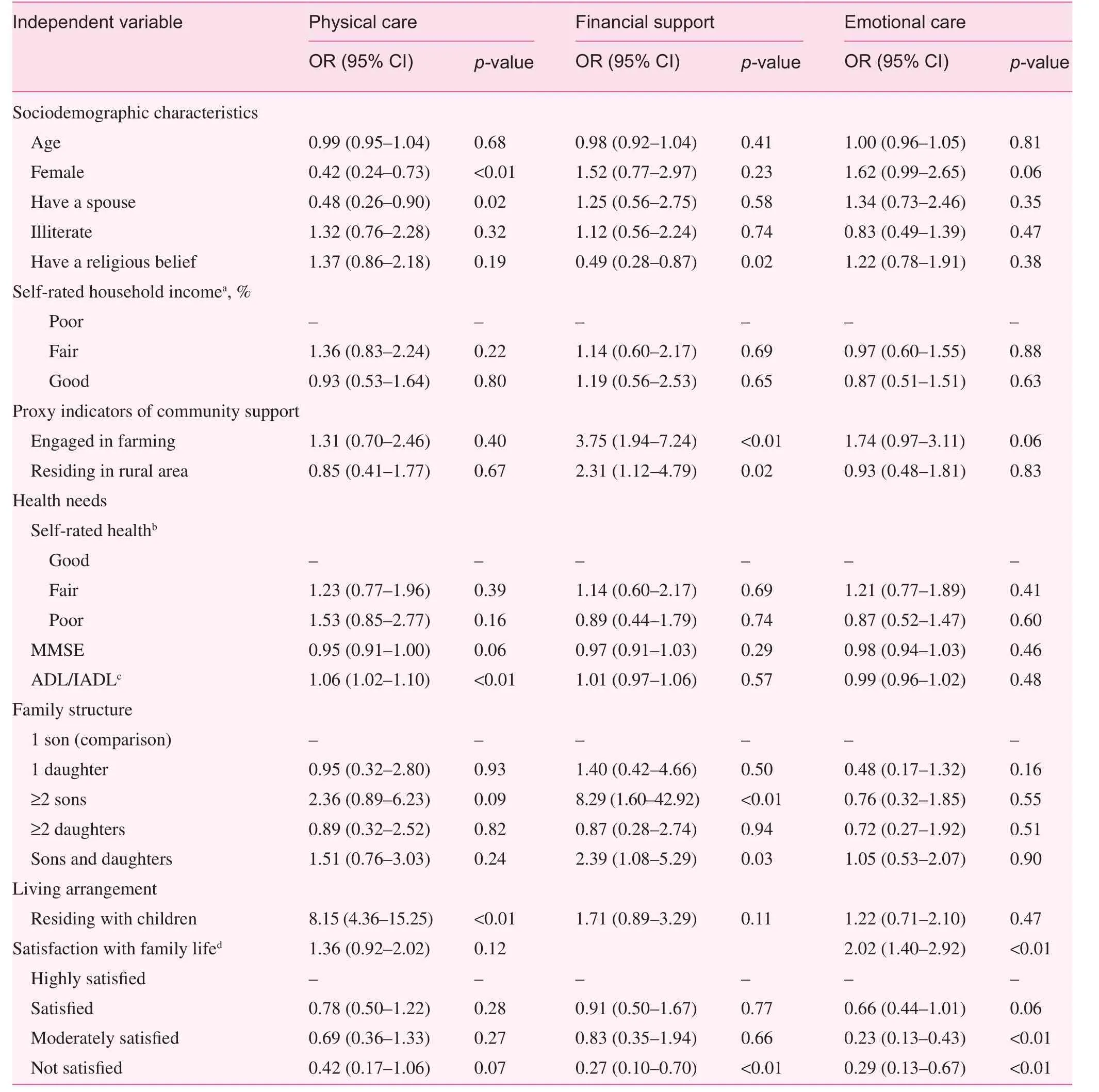
Table 3. Determinants of family support: multivariate logistic regression models
Emotional care remains a serious concern. We found that what matters most to these nonagenarians and centenarians is emotional care. Emotional care was a far greater factor in satisfaction with family life than physical care or financial support. Most nonagenarians and centenarians are widowed and need to share their worries with their children. However, more offspring, regardless of their sex, had no direct relation with the provision of emotional care.
Adult daughters have started to play an increasingly important role in supporting their elderly parents [42]. Evidence from this study shows that nonagenarians and centenarians with one or more daughters enjoyed a level of physical, financial, and emotional support similar to that of nonagenarians and centenarians with only one son. Another study found that the older elderly residing with a daughter enjoy better emotional health than those residing with a son [43]. In urban China, married daughters provide more financial support to parents than do married sons, which may be primarily explained by daughters'resources [44].
Limitation
This is a cross-sectional study. Therefore, no causal relations between variables can or should be assumed. The data used in this study do not allow us to estimate the volume of support and the burden of support, and this might underestimate the role of family size [18]. In addition, as the participants of this study were limited to Dujiangyan and aged 90 years or older,the findings of this study may not be generalizable to the general elderly population of China.
Policy implications
Owing to the diminishing size of the extended family, it is unlikely that the 'traditional family' would be able to sustain its historical, substantial, and primary role in supporting older people. The multiple and alternative sources of support for older people have to be considered. Over the past several decades, China has developed a multitier welfare system.Despite some progress in universal coverage of social security programs in recent years [45], they are far from sufficient to ease the financial burden on extended families. Old-age pensions continue to be largely linked to employment under a payas-you-go financial arrangement funded through enterprises.
Because large enterprises are usually located in urban areas,rural residents have much lower levels of welfare entitlements than their urban counterparts [18, 46, 47]. To fundamentally alleviate high financial dependence on a large family, the level of monetary subsidies, especially for farmers, should be continuously improved.
Coresidence of an adult child and his or her old parents,one of the most important mechanisms through which family support for older people is maintained, is expected to decline[18]. For married older elderly, coresidence doses not bring additional benefits to their psychological well-being [48].Many elderly people refuse coresidence arrangements simply because of fear of disrespect from their coresident children[6].
Although institutional aged care is developing rapidly in China [49], it is unlikely to be able to meet the soaring demands. The Dujiangyan Local Government has developed a plan for aged care facilities with 6170-bed capacity by 2020,but this can support only 3% of the aged population (≥65 years)[48, 50]. The quality of aged care services provided by the current facilities has also attracted much concern [49].
In line with the international trend of building 'aged care in the community' and 'aged care by the community,' China has implemented a family-centered community service system [51]. However, this is still in its infancy and is restricted largely to urban communities [52]. This model needs more policy support and resources [53, 54].
Although financial and physical support may become available from sources other than the family, the primacy of the family with respect to emotional care and well-being cannot be substituted. Yet, empirical evidence shows that coresidence does not necessarily prevent elderly people from feeling lonely[20]. Conversations between older people and their adult children have become less frequent because of the increasingly fast pace of working and social lives.
Family support has been and will continue to provide primary support for older people. The relaxation of the family planning policy will increase the chance of there being is at least one living child when parents become older. On the other hand, it might be overly optimistic to attempt to rely on increased family size for supporting the rapidly expanding populations of older people. Zimmer and Kwong [18], through a simulation study, concluded that the impact of family size reduction is limited and not as dramatic as many anticipated.
Conflict of interest
The authors declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
1. Department of Economic and Social Affairs. Population division:population ageing and development 2012. United Nations, New York. 2012. www.unpopulation.org. Accessed 15 April 2015.
2. Department of Economic and Social affairs. World population ageing 2009. Geneva: United Nations; 2009.
3. Strauss J, Smith JP, Lei XY, Yang Z, Park A, Zhao YH, et al.Health outcomes and socio-economic status among the elderly in China: evidence from the CHARLS pilot. IZA discussion paper no. 5152, Institute for the Study of Labor 2010. Available from: www.iza.org/en/webcontent/publications/papers/viewAbstract?dp_id=5152. Accessed 15 April 2015.
4. Yue JR, Dong BR, Huang CQ, Wu HM, Gao LL. Cognitive impairment and medical illness in Chinese nonagenarians and centenarians. J Am Geriatr Soc 2009;57(4):734–6.
5. Dellara FT, Paola S, Stacy LA, Thomas TP. Disentangling the roles of disability and morbidity in survival to exceptional old age. Arch Intern Med 2008;168(3):277–83.
6. Du P. Change of living arrangements of the elder in Beijing.Popul Sci Chin 1998;(2):36–41. [in Chinese]
7. Sereny M. Living arrangements of older adults in China: the interplay among preferences, realities, and health. Res Aging 2011;33(2):172–204.
8. Zimmer Z. Health and living arrangement transitions among China's oldest-old. Res Aging 2005;27(5):526–55.
9. Flaherty JH, Liu ML, Ding L, Dong BR, Ding QF, Li X, et al.China: The aging giant. J Am Geriatr Soc 2007;55(8):1295–300.
10. Lin JP, Yi CC. Filial norms and intergenerational support to aging parents in China and Taiwan. Int J Soc Welfare 2011;20(S1):S109–20.
11. Zuo DM, Wu Z, Li SZ. Age and intergenerational exchange among older parents in rural China. Int J Soc Welfare 2011;20(S1):S30–46.
12. Lee YJ, Xiao Z. Children's support for elderly parents in urban and rural China: results from a national survey. J Cross Cult Gerontol 1998;13(1):39–62.
13. Hussain A. Demographic transition in China and its implications.World Dev 2002;30(10):1823–34.
14. Wu CP, Wang L, Miao RF. Scanning the choice of national population of China from world population during a hundred years(1950~2050). Popul Res 2003;27(4):6–12. [in Chinese]
15. He W, Manisha S, Zhang KT, Guo P. Health and health care of the older population in urban and rural China: 2000. Washington,DC: US Government Printing Office; 2007.
16. Hu AG. Why it needs to adjust family planning policy. Population and Development. 2008;(1):42–5.
17. Guo XB, Yin J. Rethink of family planning policy in China. Theory Monthly 2005;(11):68–74. [in Chinese]
18. Zimmer Z, Kwong J. Family size and support of older adults in urban and rural China: Current effects and future implications.Demography 2003;40(1):23–44.
19. Chen W, Du X. Influential factors of the oldest old care and their life status in China. Popul Sci Chin 2002;(6):49–55. [in Chinese]
20. Wang LH, Schneider JW. Types of home care for the elderly and family relations of the care giving. Soc Res 2000;(4):27–41. [in Chinese]
21. Xia CL, Ma FL. The role of the number of children in family support for the elderly. Popul Res 1995;19(1):6–12. [in Chinese]
22. Xie GH. Living arrangements of the elderly and children's caregiving behaviors. Society. 2009;29:149–67. [in Chinese]
23. Ryan AK, Willits FK. Family ties, physical health, and psychological well-being. J Aging Health 2007;19(6):907–20.
24. Zhang YT, Goza FW. Who will care for the elderly in China? A review of the problems caused by China's one-child policy and their potential solutions. J Aging Stud 2006;20(2):151–64.
25. Guo ZG, Zhang KD. Retesting the role of the number of children in family support for the elderly. Popul Res 1996;20(2):7–15. [in Chinese]
26. Chengdu Statistic Bureau. Chengdu statistical yearbook 2011.Beijing: China Statistics Press; 2011. [in Chinese]
27. Dujiangyan Statistic Bureau. 2011 National economy and social development in Dujiangyan. Dujiangyan Government, Dujiangyan. 2012. http://tjj.djy.gov.cn/html/tongjigongbao/201203/27-248.html. Accessed 15 April 2015. [in Chinese]
28. The Sixth National Census Office of Dujiangyan. Main population data in the six national census in Dujiangyan. 2011. http://tjj.djy.gov.cn/html/tongjixinxi/201109/13-217.html. Accessed 15 April 2015. [in Chinese]
29. State Statistical Bureau. Tabulation on the 2010 population census of the People's Republic of China. Beijing: China Statistical Publishing House; 2012. [in Chinese]
30. Flaherty JH, Dong B, Wu H, Zhang Y, Guralnik JM, Malmstrom TK, et al. Observational study of 1-year mortality rates before and after a major earthquake among Chinese nonagenarians.J Geront A Biol Sci Med Sci 2011;66A(3):355–61.
31. Kim SY, Sok SR. Relationships among the perceived health status, family support and life satisfaction of older Korean adults.Int J Nurs Pract 2012;18(4):325–31.
32. Leung JCB. Family support for the elderly in China. J Aging Soc Policy 1997;9(3):87–101.
33. Zhang T, Chen Y. Meeting the needs of elderly people in China.Br Med J 2006;333(7564):363–4.
34. Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. Studies of illness in the aged. The index of ADL: a standardized measure of biological and psychosocial function. J Am Med Assoc 1963;185:914–9.
35. Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist 1969;9(3):179–86.
36. LaPlante MP. The classic measure of disability in activities of daily living is biased by age but an expanded IADL/ADL measure is not. J Geront B Psychol Sci Soc Sci 2010;65B(6):720–32.
37. Folstein MF, Folstein SE, McHugh PR. Mini-mental state. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975;12(3):189–98.
38. Zhang ZX, Hong X, Li H, Zhao JH, Huang JB, Wei J, et al. The Mini-Mental State Examination in the Chinese residents population aged 55 years and over in the urban and rural areas of Beijing. Chin J Neurol 1999;32:149–53.
39. Dong MJ, Peng B, Lin XT, Zhao J, Zhou YR, Wang RH. The prevalence of dementia in the People's Republic of China:a systematic analysis of 1980–2004 studies. Age Ageing 2007;36(6):619–24.
40. Leamer EE. Multicollinearity: a Baysian interpretation. Rev Econ Stat 1973;55(3):371–80.
41. Li JX, Yu XJ, Wang GZ, Liu HY. Desires and practice for old-age support in China. Population Econ 2004;(5):7–39. [in Chinese]
42. Tang C, Ma CH, Shi JQ. Ethic and fairness of daughter's supporting to her parents' family: gender study on intergenerational family relation in rural areas of eastern Zhejiang province. Soc Stud 2009;24:18–36. [in Chinese]
43. Chen F, Short SE. Household context and subjective well-being among the oldest old in China. J Fam Issues 2008;29(10):1379–1403.
44. Xie Y, Zhu HY. Do sons or daughters give more money to parents in urban China? J Marriage Fam 2009;71(2):174–86. [in Chinese]
45. Yan QC. Current situation and prospects for social security system for the elderly in China. China National Conditions and Strength 2012;(9):9–12. [in Chinese]
46. Ye ZR, Long YS. Disparity of social security for the older between urban and rural areas: a case of Chengdu. Rural Economy 2012;(2):75–8. [in Chinese]
47. Jiang M. The obstruction of public policy system: rural social pension insurance in western of Fujian. Journal of Beijing University of Aeronautics and Astronautics (Social Science Edition)2012;25(1):6–9, 35.
48. Wang J, Chen T, Han B. Does co-residence with adult children associate with better psychological well-being among the oldest old in China? Aging Ment Health 2014;18(2):232–9.
49. Feng ZL, Zhan HJ, Feng XT, Liu CH, Sun MY, Mor V. An industry in the making: the emergence of institutional elder care in urban China. J Am Geriatr Soc 2011;59(4):738–44.
50. Chengdu Government Office. Distribution of facilities for the aged plan in Chengdu 2011–2020. Chengdu Government,Chengdu. 2012. www.sc.gov.cn/10462/10705/10709/2012/1/16/10222797.shtml. Accessed 15 April 2015. [in Chinese].
51. Wu B, Carter MW, Goins RT, Cheng C. Emerging services for community-based long-term care in urban China: a systematic analysis of Shanghai's community-based agencies. J Aging Soc Policy 2005;17(4):37–60.
52. Chen Z, Yu J, Song YT, Chui DH. Aging Beijing: Challenges and strategies of health care for the elderly. Ageing Res Rev 2010;9S:S2–5.
53. Brownie S, Horstmanshof L. Creating the conditions for selffulfillment for aged care residents. Nurs Ethics 2012;19(6):777–86.
54. Low LF, Yap M, Brodaty H. A systematic review of different models of home and community care services for older persons.BMC Health Serv Res 2011;11(1):93–107.
Ningxiu Li, MD Department of Health and Social Behavior, West China School of Public Health, Sichuan University, No. 16, Section 3, Renmin South Road, Chengdu, Sichuan 610041, China
Tel.: +86-28-5501646
E-mail: liningxiu@163.com
15 July 2015;
Accepted 4 August 2015
 Family Medicine and Community Health2015年4期
Family Medicine and Community Health2015年4期
- Family Medicine and Community Health的其它文章
- Current situation of AIDS prevention and control with traditional Chinese medicine and relevant policies in China
- A new paradigm for assessment of infant feeding deviation
- Exploration and practice of general practitioner responsibility system in an urban community of Shanghai
- Guest Editors' Prof le
- China's General Practice Conference highlights review
- The role of a community health service in the prevention of violence against women