
Ureteral Stent Fragmentation:a Case Report andReview of Literature
2013-11-18 13:33:04JiruiNiuZhigangJiShiRongQuanzongMaoHuaFanandXiaoHe
Chinese Medical Sciences Journal 2013年2期
Ji-rui Niu,Zhi-gang Ji*,Shi Rong,Quan-zong Mao,Hua Fan,and Xiao He
Department of Urology,Peking Union Medical College Hospital,Chinese Academy of Medical Sciences &Peking Union Medical College,Beijing 100730,China
SINCE the introduction of double J stents in 1978,ureteral stents have become an integral tool in treating ureteral obstruction from calculi and other causes.1Owing to the widespread usage of indwelling ureteral catheters,a number of possible complications such as migration,infection,pyelonephritis,breakage,encrustation,stone formation,and ureteral stents fragmentation have been noted.2Of all the complications,ureteral stent fragmentation was sporadically reported and believed to be rare.3Here we present a case of fragmentation of a new type of double J stent,which was used to provide free drainage to the bladder after balloon dilation.
CASE DESCRIPTION
A 25-year-old man was admitted for obstruction at the left ureteropelvic junction.He had undergone extracorporeal shock wave lithotripsy for left renal calculi 4 years before and the same treatment again 10 months before in other hospitals.He was diagnosed as left ureteropelvic junction obstruction upon admission into Peking Union Medical College Hospital on November 30th,2010 and therefore treated with cystoscopic-guided balloon dilation on December 3rd.A new type of double J stent was placed to the right place during that procedure,as confirmed in a kidney,ureter,and bladder (KUB) X-ray (Fig.1).The double J stent was removed in February,2011.Computed tomography urography conducted in May demonstrated an obstruction at the left ureteropelvic junction and a“ureteral stone”,which was suspected to be a part of the double J stent.KUB demonstrated a fragmented ureteral stent that looked like a regular metallic body (Fig.2).Dismembered pyeloplasty was performed on July 25th.
The“ureteral stone”was confirmed to be the fragmentation of the double J stent.The patient recovered after the pyeloplasty.

Figure 1.Kidney,ureter,and bladder (KUB) X-ray displays the location of double J stent after surgery.
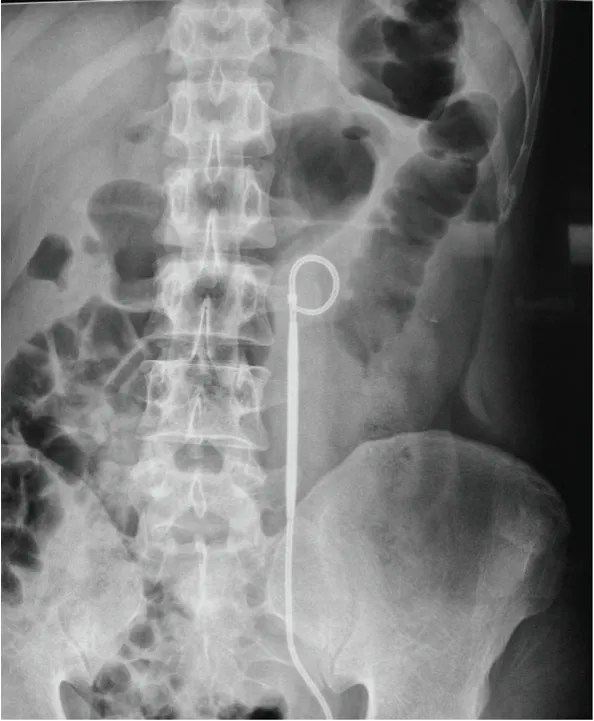
Figure 2.KUB X-ray displays the location of the foreign body in left.
DISCUSSION
Ureteral stents have a diverse role in the management of calculi,genitourinary reconstruction,renal transplantation,genitourinary tumor,genitourinary trauma,and obstructive uropathy.Since the introduction of the double J ureteral stent,improvements have been made in stent composition and design,but complications including stent migration,encrustation,fragmentation,occlusion,and stone formation were encountered frequently.The rate of ureteral stent fragmentation ranges between 0.3% and 10%.4,5el-Faqihet al4reviewed 290 patients who had stent-related complications;they found encrustation in 76%,stent migration in 3.7%,infection in 6.7%,and fragmentation in 0.3%.
Different mechanisms have been proposed to explain the occurrence of ureteral stents fragmentation.Breakage of a stent has been attributed to the hostility of the urine.Interaction with urine and extensive inflammatory reactionin situmay be important in the initiation and promotion of degradation.6The other factor linked with stent fragmentation is stent material.There is no consensus on what is the ideal material for ureteral stents.Silicone stents may be more advantageous than polyurethane stents for the lower risk of calcification and prolonged maintenance of tensile strength up to 20 months.7The resonance metallic ureteral stent has been introduced for managing the ureteral obstruction of extrinsic etiology,which could indwell for a period up to 12 months.8Another factor associated with stent fragmentation is kinking.It was suggested that fragmentation may occur at a site previously kinked before stent insertion.Thus kinking during stent insertion must be avoided.However,these theories can not explain why some fragmentations happen early after stent indwelling.In the study by Zismanet al,3mechanical testing and fractography clearly showed that the stent material changed from ductile to brittle during exposure to a specific environment.The same phenomenon was observed in the study by Richter et al.9In the present case,the stent had fragmented into two pieces about 3 months after placement of the ureteral stent.
The clinical presentation of ureteral stent fragmentation may vary,may be asymptomatic,or with septic,irritative,and hemorrhagic symptoms.According to Ilkeret al,6it is quite common to find abundant leukocytes in urine with or without any infection,which may be derived at least in part from depolymerization of biomaterials by release of lysosomal enzymes.Klicileret al7reported one patient admitted to their clinic for right flank pain,intermittent hematuria,and fever.The patient in the present case was asymptomatic,and admitted to treat the left ureteropelvic junction obstruction.
Management of stents-related complications requires coordinated use of the latest lithotripsy,endourological techniques,or open surgery.Removal of the fragmented stent may be challenging,since a combined approach is often required,including cystoscopy,ureteroscopy,and percutaneous nephroscopy.LeRoyet al10treated 3 patients with fractured polyethylene-polyurethane stents,3 with calcified silicone stents,and 7 with migrated silicone stents through a percutaneous approach.They recommended this method over the retrograde approach for patients with ureteral strictures,or fragmented or calcified stent remnants in the renal pelvis.
Due to the location of the fragmentation and the structure of the ureter,it was difficult to retrieve the stent completely using a retrograde ureteroscopic procedure in the present case;thus open surgery was chosen.Using this method,we finally removed the stent completely and cured the obstruction at pelvic junction with dismembered pyeloplasty.
Several measures are recommended to prevent complications associated with stent placement.Accurate length and optimum placement of stents could minimize stent migration.Timely cystoscopic removal or exchange of ureteral stents could minimize the risk of calcification and fragmentation.Early exchange of ureteral stents may be prudent in patients prone to stone formation.Prophylactic antibiotic therapy may decrease the risk of infected stone encrustation.Patients should be reminded of possible problems caused by the ureteral stent indwelling for a prolonged period of time.Moreover,a computerized registry of stent placement may be used to alert the urologist when the stent must be removed.7
Spontaneous breakage of indwelling stents is an unusual complication with very low incidence,and close follow-up is necessary to prevent serious results.The fragmentation of the stent in the present case was found after surgery and the patient was closely followed up.
1.Joshi HB,Okeke A,Newns N,et al.Characterization of urinary symptoms in patients with ureteral stents.Urology 2002;59∶511-6.
2.Slaton JW,Kropp KA.Proximal ureteral stent migration∶an avoidable complication? J Urol 1996;155∶58-61.
3.Zisman A,Siegel YI,Siegmann A,et al.Spontaneous ureteral stent fragmentation.J Urol 1995;153∶718-21.
4.el-Faqih SR,Shamsuddin AB,Chakrabarti A,et al.Polyurethane internal stents in treatment of stone patients∶morbidity related indwelling times.J Urol 1991;146∶1487-91.
5.Monga M,Klein E,Casta?eda-Zú?iga WR,et al.The forgotten indwelling ureteral stent∶a urological dilemma.J Urology 1995;153∶1817-9.
6.Ilker Y,Türkeri L,Dillio?lugil O,et al.Spontaneous fracture of indwelling ureteral stents in patients treated with extracorporeal shock wave lithotripsy∶two case reports.Int Urol Nephrol 1996;28∶15-9.
7.Kliciler M,Erdemir F,Bedir S,et al.Spontaneous ureteral stent fragmentation∶a case report and review of the literature.Kaohsiung J Med Sci 2006;22∶363-6.
8.Liatsikos E,Kallidonis P,Kyriazis I,et al.Ureteral obstruction∶is the full metallic double-pigtail stent the way to go?Eur Urol 2010;57∶480-6.
9.Richter S,Ringel A,Shalev M,et al.The indwelling ureteric stent∶a ‘friendly’ procedure with unfriendly high morbidity.BJU Int 2000;85∶408-11.
10.LeRoy AJ,Williams HJ Jr,Segura JW,et al.Indwelling ureteral stents∶percutaneous management of complications.Radiology 1986;158∶219-22.
 Chinese Medical Sciences Journal2013年2期
Chinese Medical Sciences Journal2013年2期
- Chinese Medical Sciences Journal的其它文章
- Unsuspected Gallbladder Cancer During or After Laparoscopic Cholecystectomy
- Blood Lead Levels During Pregnancy and Its Influencing Factors in Nanjing,China
- Physiological Testosterone Retards Cardiomyocyte Aging in Tfm Mice via Androgen Receptor-independent Pathway△
- Introduction of Management of Prostate Cancer:a Multidisciplinary Approach
- Chinese Herbal Medicine in Treatment of Polyhydramnios: a Meta-analysis and Systematic Review△
- Open Surgical Insertion of Tenkchoff Straight Catheter Without Guide Wire