
Clinical Study on Puncturing Houxi (SI 3) Toward Hegu (LI 4) plus Lumbar Movement for Acute Lumbar Sprain
2013-07-18 11:57:17ZhouJinghuiWuYaochiSunYijunZhangJunfeng
Zhou Jing-hui, Wu Yao-chi, Sun Yi-jun, Zhang Jun-feng
Department of Acupuncture, Tuina and Traumatology, No.6 People’s Hospital Affiliated to Shanghai Jiaotong University, Shanghai 200233, China
Clinical Study on Puncturing Houxi (SI 3) Toward Hegu (LI 4) plus Lumbar Movement for Acute Lumbar Sprain
Zhou Jing-hui, Wu Yao-chi, Sun Yi-jun, Zhang Jun-feng
Department of Acupuncture, Tuina and Traumatology, No.6 People’s Hospital Affiliated to Shanghai Jiaotong University, Shanghai 200233, China
Objective: To observe the therapeutic efficacy of puncturing Houxi (SI 3) toward Hegu (LI 4) plus lumbar movement in treating acute lumbar sprain.
Methods: A total of 212 patients with acute lumbar sprain were randomized into two groups. There were 106 subjects in the observation group who were treated with puncturing Houxi (SI 3) toward Hegu (LI 4) plus lumbar movement; the other 106 patients in the control group were treated with puncturing Houxi (SI 3) toward Hegu (LI 4) alone. Therapeutic efficacy was evaluated after 2 treatment courses.
Results: The total effective rate was 95.3% in the observation group versus 88.7% in the control group, and the difference was statistically insignificant between the two groups (P>0.05). However, in comparing the treatment times for achieving recovery and effectiveness, differences between the two groups were statistically significant (bothP<0.05), indicating that integrated use of acupuncture and exercise is faster in realizing therapeutic effectiveness.
Conclusion: By selecting fewer acupoints, puncturing Houxi (SI 3) toward Hegu (LI 4) is effective in treating acute lumbar sprain, and with the help of lumbar movement, it can achieve even better treatment effect.
Point-through-point Method; Acupuncture Therapy; Electroacupuncture; Low Back Pain; Lumbar Sprain; Sprains and Strains
Acute lumbar sprain refers to acute injury to soft tissues, such as muscles, fascia, and ligaments, when overstretched by external forces. It is often caused by over-loading, improper posture and movement, sudden fall, over-lifting, insufficient preparation before exercise, or over-stretching. When it happens, the sufferer will experience lumbar stiffness immediately, as well as inability to bend and turn and extreme pain, which may seriously affect the patient’s life and work. Acute lumbar sprain is one of the typical indications of acupuncture-moxibustion therapy[1-3], but the treatment protocols vary. We treated acute lumbar sprain with puncturing Houxi (SI 3) toward Hegu (LI 4) plus lumbar exercise, and conducted a comparative study by setting up a control group treated with point-through-point method alone from July 2008 to December 2010, and now report it as follows.
1 Clinical Data
1.1 Diagnostic criteria
It was referred to the diagnostic criteria of acute lumbar sprain inShanghai Diagnostic and Therapeutic Guidelines of Traditional Chinese Diseases and Syndromes[4]. Subject is often a young adult and there is a history of lumbar sprain; excessive pain on one side or both sides of the waist, with limited motion, inability to roll over, sit up or walk, and compulsive posture to reduce pain; lumbar and buttocks muscle spasm, causing muscular nodes and tenderness points in the injured area, and altered spine curvature.
1.2 Inclusion criteria
Conforming to the diagnostic criteria of acute lumbar sprain, with a course of disease within 3 d; aged 25-60 years, with no gender predilection; other treatments were ceased during this treatment duration; patients who were willing to participate in the study, and signed the informed consent form.
1.3 Exclusion criteria
Lumbar intervertebral disc herniation, and acute lumbar sprain but coupled with lumbar spondylolisthesis, spinal lesions, sacroiliac joint or hip joint diseases, or peripheral vascular disease; patients with systemic immune diseases, or other chronic or acute infectious diseases being treated by glucotorticoid, which might influence the evaluation of treatment effect.
1.4 General data
A total of 212 eligible subjects were recruited from the outpatients of the Department of Acupuncture, Tuina and Traumatology, No.6 People’s Hospital Affiliated to Shanghai Jiaotong University from July 2008 to December 2010. They were randomized into 2 groups by their visiting sequence, i.e. the observation group and the control group. Of the 106 cases in the observation group, there were 60 males and 46 females, aged 28-48 years (40 on average), and with a disease duration ranged from 60 min to 3 d (disease duration of 1 d occupying 82%). Of the 106 subjects in the control group, there were 50 males and 56 females, aged 25-50 years (averaged 41), and with a disease duration ranged from 30 min to 3 d (disease duration of 1 d occupying 80%).
The clinical processes of the two groups are shown in Fig.1.
2 Treatment Methods
2.1 Observation group
Acupoints: Bilateral Houxi (SI 3) and Waiguan (TE 5).
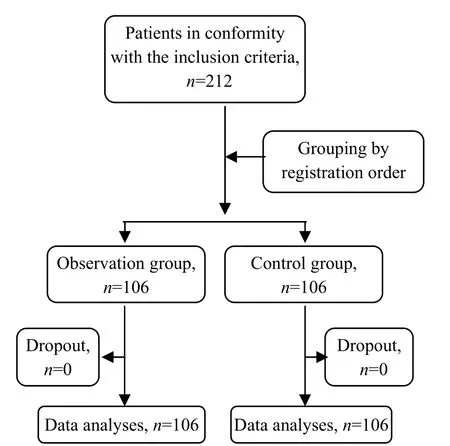
Fig.1 Clinical processes of the two groups
Operation: The patient was standing by treatment bed, with palms facing downward supporting on the bed naturally. After standard sterilization with 75% alcohol cotton, a filiform needle of 0.35 mm in diameter and 40 mm in length was perpendicularly punctured into Houxi (SI 3) towards Hegu (LI 4) by depth of 1.2 cun. Mild reducing manipulation of lifting-thrusting was performed for continuous 1 min after the qi arrival. Local distending feeling was required to spread to the whole hand. Afterwards, the physician stood behind the patient with two hands supporting the patient’s lower back, and asked him to rotate his waist, small circle to big circle and slow to fast, within the endurance of the patient. If the patient was feared of pain and didn’t dare to move, the doctor should take the active role and help the patient to move till he felt his lumbar muscles relaxed enough for active movement. Lumbar exercise should take 3 min. During exercise, physician could help the patient with his force in order to rotate in a bigger circle. Finally, the patient was asked to take a prone position and put his hands over his head. Han’s Acupoint Nerve Stimulator was used with one probe sticking to Waiguan (TE 5) and the other clipping to the needle in Houxi (SI 3) point. Acupuncture pattern was selected with continuous wave and frequency of 40 Hz and currency of 2 mA, and the total electroacupuncture stimulation lasted 20 min. The treatment was given once a day, 3 times of treatment as an observation course, with a-day interval between each two courses, and 2 observation courses were conducted in total.
Pay attention that the patient should be watched during the whole treatment in prevention of falling or fainting from needling. If the patient cannot bear theintensity of the point-through-point needling with a standing position, he can be seated to receive acupuncture stimulation and then stand up to move his waist when his lumbar muscles are relaxed.
2.2 Control group
3 Therapeutic Efficacy
3.1 Criteria of therapeutic efficacy
It was referred to the effect evaluation criteria of acute lumbar sprain inShanghai Diagnostic and Therapeutic Guidelines of Traditional Chinese Diseases and Syndromes[4].
Recovery: Lower back pain is relieved, and spine can move normally.
Improved: Lower back pain is reduced, and spine movement is substantially normal.
Invalid: Lower back pain and movement are not improved.
3.2 Statistical analyses
The SPSS 11.0 was adopted for statistical analyses. Measurement data were compared by usingt-test and enumeration data were by Ridit analysis.
3.3 Treatment result
3.3.1 Comparison of therapeutic efficacy
It was showed in table 1. After 2 treatment courses, the total effective rate was 95.3% in the observation group versus 88.7% in the control group, and the difference was statistically insignificant between the two groups (P>0.05).

Table 1. Comparison of clinical efficacy (case)
3.3.2 Comparison of the treatment course
Of the recovered cases, treatment times ranged from 1 time to 3 times (averaged on 2 times) in the observation group and from 2 times to 6 times (averaged on 4 times) in the control group. Statistical analysis showedt=2.203 andP<0.05, which indicated that the difference in treatment times between the two groups was statistically significant. Of the improved cases, treatment times ranged from 1 to 4 (averaged on 2.5) in the observation group and from 3 to 6 (averaged at 4.5) in the control group. Statistical analysis showedt=2.753 andP<0.05, indicating that the difference in treatment times between the two groups was statistically significant. It showed that acute lumbar sprain responded faster to acupuncture plus lumbar exercise.
4 Experiences
Acute lumbar sprain belongs to the scope of lumbago in Chinese medicine, and is usually caused by sudden force, and subsequent damage to lumbar meridians and collaterals, qi and blood stagnation, blockage of meridians, manifested by pain and inability to move lower back. Houxi (SI 3) functions to dredge and activate tendons and collaterals, activate qi flow and kill pain, soothe and refresh mind, relieve convulsion, clear heat and expel external pathogens. Among which, the function of dredging and activating tendons and collaterals is the most significant[5-6]. Houxi (SI 3) communicates with the Governor Vessel and is one of the Confluent Points of the Eight Extraordinary Meridians and also the Shu-Stream point (Shu-Stream points are in charge of joint pain and heaviness feeling) of the Small Intestine Meridian of Hand Taiyang. The Hand and Foot Taiyang Meridians connect with each other. Since meridians can be used to treat the diseases occurring in their pathways, so the involving symptoms of the Governor Vessel and Foot Taiyang Meridian can all be treated by selecting Houxi (SI 3)[7-9]. During the process of puncturing Houxi (SI 3) toward Hegu (LI 4), the needle body runs through Yaotongdian (EX-UE 7, two points for lower back pain) inside muscles, objectively playing a multiple-acupoint functions by needling only one acupoint and approaching therapeutic efficacy swiftly.
With acupuncture, proper lower back movement can effectively relieve muscle spasm in lower back, dredge meridians and collaterals, unblock the path of qi and blood, correct the micro-dislocation of small joints, and replace the tendons and ligaments in sprains[10]. During retaining of the needle, electrical stimulation, combined with needling stimulation, reaches proper stimulation quantity and extends the acupuncture effect. Continuous wave can resist the impulse transmission of sensory nerve and motor nerve, and is thus used for killing pain, tranquilization, relieving muscular and vascular spasms, etc.
Generally speaking, puncturing Houxi (SI 3) toward Hegu (LI 4) has accurate efficacy in treating acute lumbar sprain, and its simple operation, efficiency and satisfactory long-term efficacy have all proved in the previous studies[11]. More significant analgesic effect can be achieved if the patient keeps standing and tries to squat and rotate waist for enhancing the activation of meridian qi during acupuncture treatment[12-13].
[1] Qi LZ, Huang QF, Huang Y. Indication spectrum reflected by modern Chinese medicine journals. Shanghai Zhenjiu Zazhi, 2006, 25(11): 46-50.
[2] Zhang L. Treatment of 34 cases of acute lumbar sprain with electroacupuncture plus cupping therapy. J Acupunct Tuina Sci, 2009, 7(4): 235-236.
[3] Wu YC, Zhang JF, Li SS, Zhou JH, Zhang SH, Sun YJ. Clinical therapeutic effect of electroacupuncture on acute lumbar sprain and infrared thermography research. Shanghai Zhenjiu Zazhi, 2010, 29(1): 716-718.
[4] Shanghai Municipal Health Bureau. Shanghai Diagnostic and Therapeutic Guidelines of Traditional Chinese Medicine. 2nd Edition. Shanghai: Publishing House of Shanghai University of Traditional Chinese Medicine, 2003: 392-392.
[5] Wu YC, Wang CM, Zhang BM. Clinical observation on the treatment of acute lumbar sprain by electroacupuncture of point Houxi. Shanghai Zhenjiu Zazhi, 2005, 24(12): 22-24.
[6] Liu WH, Du YH. Therapeutic observation of needling three hand yang meridian acupoints to treat postapoplectic finger. J Acupunct Tuina Sci, 2007, 5(5): 301-303.
[7] Jia SY. Needling Houxi (SI 3) for acute lumbar sprain: clinical analysis of 328 cases. Linchuang He Shiyan Yixue Zazhi, 2009, 8(3): 124.
[8] Wu YC, Zhang JF, Wang CM, Wang JX. Clinical study of tuina for stiff neck. J Acupunct Tuina Sci, 2009, 7(4): 225-227.
[9] Yang L, Pei JC. Function and clinical applications of Houxi (SI 3). Zhongyiyao Xuekan, 2004, 22(4): 726, 745.
[10] Zhang QM, Fang M. Current status of tuina therapy in treating acute lumbar sprain. Jingyaotong Zazhi, 2003, 24(4): 248-250.
[11] Zhang BM, Wu YC, Wang CM. 58 cases of acute lumbar sprain treated by needling Houxi (SI 3). Zhongguo Linchuang Kangfu, 2004, 8(2): 321-322.
[12] Li L, Yao L, Han LB. Observation on the clinical efficacy of balancing acupuncture plus kinesiltherapy for post-stroke shoulder-hand syndrome. Shanghai Zhenjiu Zazhi, 2011, 30(9): 607-608.
[13] Liu FC. Clinical observation on scalp acupuncture plus motortherapy for post-stroke depression. Shanghai Zhenjiu Zazhi, 2011, 30(1): 733-734.
Translator: Hong Jue
Received Date: November 20, 2012
R246.2
A
in the control group
the same point-through-point needling treatment as those in the observation group but were not asked to do lumbar movement.
Author: Zhou Jing-hui, M.M., attending physician. E-mail: 18930173736@189.cn
Wu Yao-chi, professor, doctoral supervisor. E-mail: wuyaochi@online.sh.cn
 Journal of Acupuncture and Tuina Science2013年1期
Journal of Acupuncture and Tuina Science2013年1期
- Journal of Acupuncture and Tuina Science的其它文章
- Acupuncture-moxibustion Theories of Wang Shu-he
- Treatment of Tolosa-Hunt Syndrome with Acupuncture: A Case Report
- Research Progress of Acupuncture Analgesia for Labor
- Therapeutic Effect of Warm Needling Therapy Combined with Rehabilitation Therapy for Brachial Plexus Injury after Surgery
- Electroacupuncture in Treating Depression: A Randomized Controlled Study
- Study on the Relation Between MRI Findings and Acupuncture Effect in Trigeminal Neuralgia Patients