
Study on the Relation Between MRI Findings and Acupuncture Effect in Trigeminal Neuralgia Patients
2013-07-18 11:57:17BaoHongLiJingZhuLequnYuanJunXuKaiwen
Bao Hong, Li Jing, Zhu Le-qun, Yuan Jun, Xu Kai-wen
1 Department of Medical Imaging, Yueyang Hospital of Integrated Traditional Chinese and Western Medicine Affiliated to Shanghai University of Traditional Chinese Medicine, Shanghai 200437, China
2 Department of Acupuncture & Moxibustion, Yueyang Hospital of Integrated Traditional Chinese and Western Medicine Affiliated to Shanghai University of Traditional Chinese Medicine, Shanghai 200437, China
Study on the Relation Between MRI Findings and Acupuncture Effect in Trigeminal Neuralgia Patients
Bao Hong1, Li Jing2, Zhu Le-qun1, Yuan Jun1, Xu Kai-wen2
1 Department of Medical Imaging, Yueyang Hospital of Integrated Traditional Chinese and Western Medicine Affiliated to Shanghai University of Traditional Chinese Medicine, Shanghai 200437, China
2 Department of Acupuncture & Moxibustion, Yueyang Hospital of Integrated Traditional Chinese and Western Medicine Affiliated to Shanghai University of Traditional Chinese Medicine, Shanghai 200437, China
Objective: To observe the relationship between acupuncture and MRI (Magnetic Resonance Imaging)findings in patients with trigeminal neuralgia (TN).
Methods: A total of 32 idiopathic TN patients who completed acupuncture treatment protocol were recruited in this trial. The relationship between acupuncture effect and MRI findings were analyzed by using MRI-B-FFE (Balanced Fast Field Echo) technique to record MRI information, such as the distance from the brainstem to the contact point of offending vessels and trigeminal nerve, the contact angle of offending vessels and trigeminal nerve, and the ratio of the diameter of the contact vessel to trigeminal nerve width.
Results: After acupuncture treatment, 9 cases got marked effect, 19 got improvement, and 4 got no effect. Acupuncture effect was neither associated with the distance from the brainstem to the contact point of the offending vessel and trigeminal nerve (P>0.05) nor the ratio of the diameter of the offending vessel to trigeminal nerve width (P>0.05); however, it was indeed associated with the running course of the offending vessels (P<0.05).
Conclusion: The bigger the angle between the offending vessels and trigeminal nerve, the poorer the acupuncture effect. The B-FFE technique can be used for screening acupuncture-indicated TN patients.
TrigeminalNeuralgia; Magnetic Resonance Imaging; Acupuncture Analgesia; Acupuncture-moxibustion Therapy; Warm Needling Therapy
The theory on microvascular compression and idiopathic trigeminal neuralgia (TN) has been extensively recognized. In order to screen acupuncture-indicated patients and predict the expected acupuncture effect, it is of great significance to study the association between acupuncture effect and Magnetic Resonance Imaging (MRI) findings on the trigeminal nerve and peripheral blood vessels. Little work has been done in this regard. We conducted a clinical study using the MRI B-FFE technique. The study is summarized as follows.
1 Materials and Methods
1.1 General material
A total of 32 idiopathic TN patients were recruited. These patients had completed the acupuncture treatment protocol as well as curative effect evaluation between December 2008 and January 2012. In addition, they allhave complete imaging findings. Of the 32 cases, there are 12 males and 20 females. They were aged from 38 to 80 years old, with a mean age of 60. Eleven cases suffered from pain on the right side, 21 on the left side. Their disease duration ranged from 0.5 to 6.5 years, with an average duration of 3 years.
1.2 Image data
1.2.1 MRI technique
The Intera 1.0T superconducting MRI system manufactured by Philips was used with head coils.
Standard MRI technique: Spin Echo (SE) pulse sequence T1-weighted axis, sagittal view scan and Turbo Spin Echo (TSE) pulse sequence T2-weighted axis scan.
Scan parameters are as follows: T1-weighted, TE 13 ms, TR 431 ms, 90° inverting pulse, Field of View (FOV) 230 mm × 230 mm, matrix 512 × 512, 5 mm slice thickness, 1 mm distance, 18 slices in total. T2-weighted, TE 120 ms, TR 4464 ms, 90° inverting pulse, FOV 230 mm × 230 mm, matrix 512 × 512, 5 mm slice thickness, 1 mm distance, 18 slices in total.
B-FFE technique: Conduct axial scan along the running course of the trigeminal nerve in the pontocerebellar angle, using the positioning of the head sagittal view.
Scan parameters are as follows: TE 3.9 ms, TR 7.8 ms, 50° inverting pulse, FOV 150 mm × 150 mm, matrix 256 × 256, 2 mm slice thickness, 1 mm distance (i.e., 1 mm overlap), 24 slices in total, and model reconstructed. Patients with tumor-induced TN patients were given enhancement scan after the intravenous injection of 0.1 mmol/(kg.bw) of Gd DTPA, immediately followed by T1-weighted axial contrast scan.
1.2.2 Image analysis
A senior radiology doctor was arranged to analyze the MRI findings using the Centricity DICOM Viewer 3.1.1 version software made by GE Company. First, exclude tumor-induced or secondary TN cases. Then select the contact slice between the trigeminal nerve and offending vessel proximal to the brainstem to measure the following indexes: the shortest distance from the brainstem to the contact point between the offending vessel and trigeminal nerve (Fig.1); the contact angle between the offending vessel and trigeminal nerve (Fig.2), acute or included angle >45° or <45°; the contact vessel and trigeminal nerve width (Fig.3) and calculate the ratio, i.e., diameter of the contact vessel/trigeminal nerve width.
1.3 Acupuncture treatment protocol
1.3.1 Acupoints
Major acupoints: Bilateral Hegu (LI 4), Wangu (GB 12), Luxi (TE 19), Chimai (TE 18), Tinggong (SI 19), Quanliao (SI 18) and trigger points on the affected side.
Adjunct acupoints: Combine with Yangbai (GB 14), Cuanzhu (BL 2) and Taiyang (EX-HN 5) for pain along the ophthalmic nerve; combine with Xiaguan (ST 7), Shangyingxiang (EX-HN 8) and Yingxiang (LI 20) for pain along the maxillary nerve; and combine with Jiache (ST 6), Dicang (ST 4) and Jiachengjiang (EX-HN 17) for pain along the mandibular nerve.
1.3.2 Operation
Ask the patient to take a supine position and sterilize the area to be needled. Then puncture the above points using needles of 0.28 mm in diameter and 50 mm in length. Upon arrival of qi, conduct 1-min even reinforcing-reducing manipulation by twirling/rotating for each point. Apply warm needling therapy to major points [Wangu (GB 12), Luxi (TE 19), Chimai (TE 18) and trigger points] and 1-2 adjunct acupoints for 2 cones (attaching approximately 0.5 g of moxa wool to the needle handle). Withdraw the needles after 20 min.
The above treatment was conducted once every other day, 3 times a week. Two weeks of treatment made up one course of treatment. The curative effect was evaluated after two courses of treatment.
1.4 Curative effect criteria
The curative effects were evaluated by a senior acupuncturist who was not involved in the treatment.
Measurement and evaluation were made before and after treatment using the Huskisson Visual Analogue Scale (VAS). The pain relief rate was calculated as well.
This measure consists of a 10 cm vernier scale, containing 10 scales on one side. One end is marked“0” (meaning no pain) and the other end is marked“10” (meaning intolerable and lacerating pain). During clinical measurement, expose the side without scales to the patients and ask them to mark a corresponding position to indicate their pain intensity. After this, the acupuncturist scored the patients’ pain according to the position.
0: No pain.
0-3: Mild pain.
4-7: Moderate pain.
8-10: Intense pain.
Pain relief rate (PRR) = (Pain score of before treatment - Pain score of after treatment)/Pain score of before treatment × 100%.
Marked effect: Absence of pain, reduced frequency of pain episodes, PRR is 75%-100%.
Improvement: Reduced frequency of pain episodes, PRR is 25%-74%.
Failure: Unrelieved pain, unreduced frequency of pain episodes, PRR is <25%.
1.5 Statistical method
The SPSS 18.0 version software was used for statistical analysis, nonparameter test for non-normal data comparison, Levene test for independent samplevariance equation andt-test for mean equation.P<0.05 indicates a statistical significance.
2 Outcome Analysis
2.1 Clinical efficacy
Of 32 cases, 9 cases obtained marked effect, 19 obtained improvement and 4 obtained no effect. The imaging findings of the 4 failure cases were not included in this study.
2.2 Image findings
The B-FFE images of all 28 idiopathic TN cases in this study visualized a clear intersection between small blood vessels and the trigeminal nerve in two or more slices.
As for the B-FFE images in 9 cases with marked acupuncture effect, the maximum and minimum distances from the affected-side offending vessel to the brainstem was 8.77 mm and 0.89 mm respectively (average distance: 3.26 mm). As for the B-FFE images in 19 cases with improvement, the maximum and minimum distances from the affected-side offending vessel to the brainstem was 7.20 mm and 0.73 mm respectively (average distance: 2.90 mm). There were no statistical significances between the two groups (t=0.399,P>0.05), indicating that acupuncture effect was not associated with the shortest distance from the brainstem to the contact point between the trigeminal nerve and offending vessels (Fig. 1).
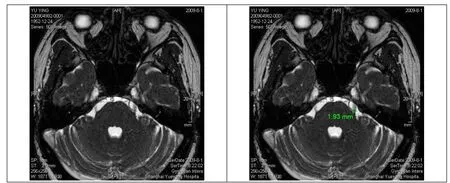
Fig.1 Measurement of the shortest distance from the brainstem to the contact point between offending vessels and trigeminal nerve (1.93 mm in this case)
As for the B-FFE images in 9 cases with marked acupuncture effect, the included angle between the affected-side trigeminal nerve and offending vessel in 3 cases >45° and the included angle between the trigeminal nerve and blood vessel in 6 cases < 45°. As for the B-FFE images in 19 cases with improvement, the included angle between the affected-side trigeminal nerve and offending vessel in 12 cases >45° and the included angle between the trigeminal nerve and blood vessel in 7 cases <45°. There were statistical significances between the two groups (t=2.66,P<0.05), indicating that acupuncture effect is associated with the running course of vessels. The bigger the included angle between the trigeminal nerve and offending vessel, the poorer the acupuncture effect (Fig.2).
As for the B-FFE images in 9 cases with marked acupuncture effect, the maximum and minimum ratios between the affected-side offending vessel and trigeminal nerve width were 1.07 and 0.31 respectively (average ratio: 0.53). As for the B-FFE images in 19 cases with improvement, the maximum and minimum ratios between the affected-side offending vessel and trigeminal nerve width were 1.0 and 0.21 respectively (average ratio: 0.38). There were no statistical differences between the two groups (t=1.08,P>0.05), indicating that acupuncture effect was not associated with the ratio of the diameter of offending vessel to the trigeminal nerve width (Fig.3).
3 Discussion
TN can be idiopathic or secondary[1]. Acupuncture is not indicated for secondary TN, since it is often triggered by a tumor encapsulating in the pontocerebellar angle or compressing the ipsolateral trigeminal nerve. However, majority TN cases are idiopathic and can be dealt with acupuncture. Regarding the etiology and pathogenesis of TN, it’s now generally believed that microvasculature of the trigeminal nerve is compressed. Such a compression can result in local demyelination and progressivedegeneration, causing the “shutting off” among adjacent nerve fibers and thus triggering pain episodes[2-4].
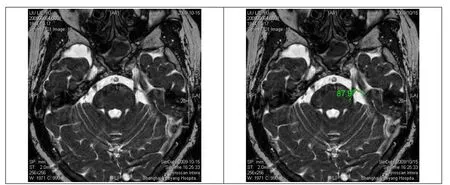
Fig.2 Measurement of the angle between the offending vessel and trigeminal nerve (87.9° in this case)
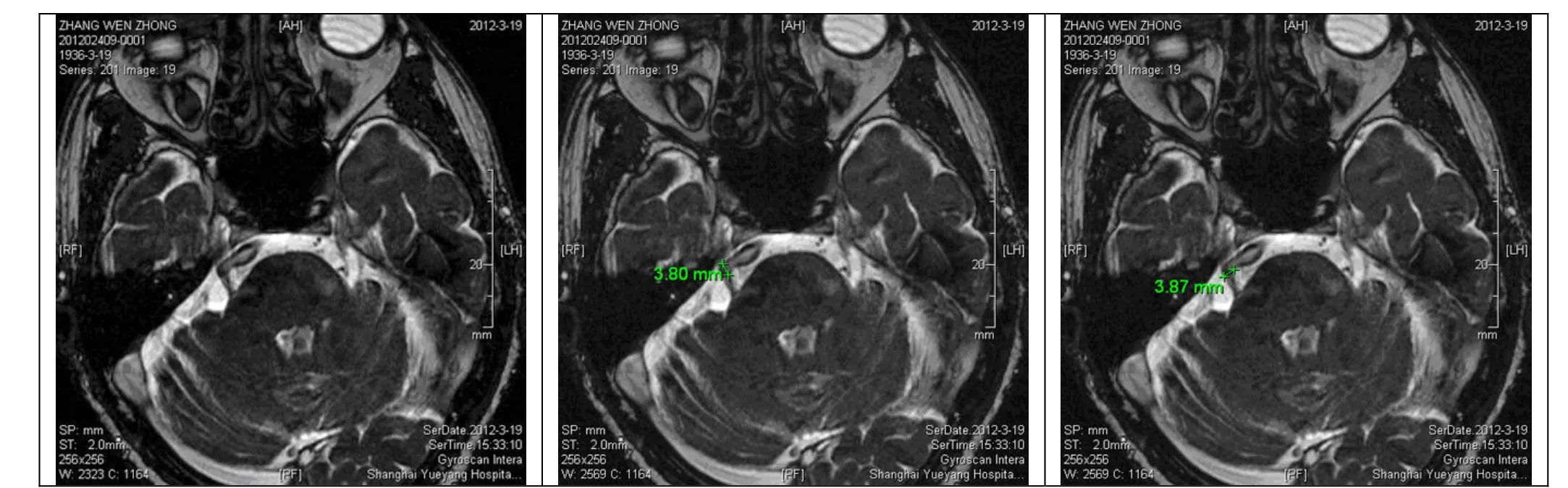
Fig.3 Measurement of the ratio between the offending vessel and trigeminal nerve width (3.80/3.87=0.98 in this case)
Acupuncture is the main Chinese medical therapy for idiopathic TN[5-11]. Prior to acupuncture treatment, it is necessary to rule out secondary TN using MRI. However, routine cranial MRI may overlook small tumors and fail to visualize the correlation between the trigeminal nerve and offending vessels. It is therefore extremely important to employ appropriate MRI technique. The new B-FFE sequence technique of MRI used in this clinical study allows a routine cranial MRI sequence test first and then B-FFE sequence test in the pontocerebellar angle. The findings visualized a relationship between capillary vessels and nerves on the affected side of all recruited cases. Previous studies have suggested that the B-FFE technique has distinctive advantages in visualizing the relationship between the trigeminal nerve and its surrounding tissues in the pontocerebellar area[12-14]: it can simultaneously present the images showing how trigeminal nerve are related to their small peripheral vessels[12], make an early detection of lesion in the pontocerebellar angle[13-14](the smallest tumor detected by this technique was sized 4 mm × 10 mm × 12 mm) and exclude secondary TN that cannot be managed by acupuncture. As a mature technique developed in recent years, the B-FFE image is associated with the T2/T1 ratio. After the signal was collected each time, a balanced gradient was used for slice selection, phase encoding and frequency encoding. This allows a complete compensation for fluid dephasing effect and produces images with increased signal in both flowing and static liquids. The transverse magnetization of static tissue reached maximal phase reunion before each excitation, providing strong signal amplitude for rapid data acquisition and causing unique contrast between liquid and solid tissues. A great deal of work has been done in visualizing offending vessels by various MRI techniques. Currently scholars from both home and abroad are using 3D technique to illustrate capillary vessels; however, the 3D technique is often time-consuming and difficult to operate. In addition, it may produce an unstable signal to noise ratio of the reconstructed image, fail to simultaneously visualize blood vessels and trigeminal nerve and miss diagnosingvessels with a slow and small flow rate[15-18]. The TR in B-FFE technique lasted a short period of time. Take this study for example, the TR was only 7.8 ms, slice thickness and distance were 2 mm and negative 1 mm respectively, i.e., 1 mm overlap, 24 slices in total can be done in 92 s. This high-resolution efficient and time-saving technique can produce well-contrasted images. We have obtained satisfactory results in evaluating the association between the trigeminal nerve and offending vessels using the B-FFE technique.
In Chinese medicine, TN falls under the category of“head-wind”, “brain-wind”, “facial wind pain” or“supra-orbital bone pain”. It is often associated with weather changes or occasional contraction of wind, and mainly caused by disharmony between qi and blood due to wind-cold attack. Contributing factors include wind, fire, phlegm, stasis and deficiency. This condition usually begins with wind or wind-fire. Over time, it may gradually mix with phlegm, stasis or deficiency. The principles of acupuncture treatment are to dispel wind, remove toxins and dredge meridian qi in the local area. Local and distal points were combined in this study. As a result, patients obtained positive effects after standard acupuncture treatment[19-20]: marked effect in 9 cases, improvement in 19 cases and failure in 4 cases. Research findings on association between imaging data and acupuncture effect have shown that acupuncture effect are neither associated with the shortest distance from the brainstem to the contact point of offending vessels and trigeminal nerve nor the ratio of the diameter of the offending vessel to the trigeminal nerve width; however, it was indeed associated with the running course of the offending vessels. The bigger the angle between the offending vessel and trigeminal nerve, the poorer the acupuncture effect. Researchers have found[4]that pain is often associated with a shorter distance from the brainstem to the contact point between the offending vessel and trigeminal nerve. This is not associated with the diameter of compressing vessels but associated with the included angle between the vessel and nerve: pain is susceptible to a bigger included angle. It is evident that the generation of pain is different from the mechanism of pain relief by acupuncture. Acupuncture relieves pain mainly by dredging meridians. TN is mainly triggered by vascular compression (close to the brainstem) and the so-called“shutting off” effect. The thinness or thickness of offending vessels are not associated with pain or acupuncture effect. However, a bigger included angle between the vessel and trigeminal nerve allows vascular pulsation conducting towards nerves, resulting in demyelination. Although acupuncture can alleviate pain, it may not prevent demyelination. As a result, a bigger included angle between the vessel and trigeminal nerve may easily cause pain and a poorer acupuncture effect. Only 4 cases got no effect in this study. This needs further study since we did not make comparison with the failure group.
In summary, MRI is essential before acupuncture treatment for trigeminal neuralgia. It is reliable to select simple and rapid B-FFE sequence to observe the association between the trigeminal nerve and offending vessel, since it can help to exclude secondary TN and also predict acupuncture effect, thus offering basis for TN patients to choose appropriate treatment protocol. Consequently, the B-FFE sequence is now used as a normal test for TN patients in our hospital.
[1] Feng DE, Wang J, Su GH. Trigeminal Neuralgia. Beijing: People’s Medical Publishing House, 2004: 75-228.
[2] Truini A, Galeotti F, Cruccu G. New insight into trigeminal neuralgia. J Headache Pain, 2005, 6(4): 237-239.
[3] Leal PR, Hermier M, Froment JC, Souza MA, Cristino-Filho G, Sindou M. Preoperative demonstration of the neurovascular compression characteristics with special emphasis on the degree of compression, using high-resolution magnetic resonance imaging: a prospective study, with comparison to surgical findings, in 100 consecutive patients who underwent microvascular decompression for trigeminal neuralgia. Acta Neurochir, 2010, 152(5): 817-825.
[4] Tang L, Chai WM, Song Q, Ling HW, Miao F, Chen KM. MRI analysis of vascular compressive trigeminal neuralgia. Zhonghua Fangshe Xue Zazhi, 2006, 40(12): 1250-1253.
[5] Huang WX. Observations on the efficacy of acupuncture at Dong’s extraordinary points as main treatment for trigeminal neuralgia. Shanghai Zhenjiu Zazhi, 2012, 31(9): 582-583.
[6] Qiao GW, Sun PH. Clinical observation on treatment of primary trigeminal neuralgia by point penetrating injection plus ear pressing. J Acupunct Tuina Sci, 2007, 5(4): 221-223.
[7] Xu SW, Hu WQ. Observations on the efficacy of electroacupuncture plus mild moxibustion in treating trigeminal neuralgia. Shanghai Zhenjiu Zazhi, 2010, 29(2): 97-98.
[8] Han ZC. Treatment of 32 cases of primary trigeminal neuralgia by acupuncture plus moxibustion with warming needle on Xiaguan (ST 7). J Acupunct Tuina Sci, 2007, 5(4): 255-256.
[9] Wu ZQ, Liu JC, Su X. Clinical observations on acupuncture plus direct current drug introduction for the treatment oftrigeminal neuralgia. Shanghai Zhenjiu Zazhi, 2010, 29(8): 509-510.
[10] Wu ZQ, Liu JC, Su X. Clinical observation on trigeminal neuralgia treated by acupuncture plus electrophoresis. J Acupunct Tuina Sci, 2011, 9(2): 95-97.
[11] Lu ZQ. Observations on the efficacy of scalp acupuncture plus body acupuncture in treating trigeminal neuralgia. Shanghai Zhenjiu Zazhi, 2008, 27(10): 12-13.
[12] Ma ZX, Li M, Chen XH, Ding SS, Yuan J. The diagnostic value for pontocerebellar angle diseases by B-FFE sequence MRI. Zhongguo Yan Er Bi Hou Ke Zazhi, 2004, 4(4): 232-233.
[13] Bao H, Ding YS, Xue F, Zhou ZM, Yuan J. The diagnosis of epidermoids of the pontocerebellar angle with balanced fast field echo. Zhonghua Fangshe Xue Zazhi, 2004, 38(11): 1185-1188.
[14] Bao H, Ding YS, Yuan J, Li M. MRI diagnosis of small epidermoids in the pontocerebellar angle: preliminary study. Shiyong Fangshe Xue Zazhi, 2007, 34(4): 437-440.
[15] Akimoto H, Nagaoka T, Nariai T, Takada Y, Ohno K, Yoshino N. Preoperative evaluation of neurovascular compression in patients with trigeminal neuralgia by use of three-dimensional reconstruction from two types of high-resolution magnetic resonance imaging. Neurosurgery, 2002, 51(4): 956-961.
[16] Chávez GD, De Salles AA, Solberg TD, Pedroso A, Espinoza D, Villablanca P. Three-dimensional fast imaging employing steady-state acquisition magnetic resonance imaging for stereotactic radiosurgery of trigeminal neuralgia. Neurosurgery, 2005, 56(3): E628.
[17] Gong LG, Liu YY, Xiao XL, Lian L. Application of high-resolution 3D-FIESTA and MR virtual endoscopy in vascular compressive trigeminal neuralgia and hemifacial spasm. Zhongguo Yixue Yingxiang Jishu, 2008, 24 (3): 350-353.
[18] Zhou Z, Yang ZY, Liu JL, Mao LJ, Li SR, Chu JP, Meng QF. The study and diagnostic value of MRI sequences in patients with trigeminal neuralgia. Zhonghua Fangshe Xue Zazhi, 2012, 46(1): 37-39.
[19] Jiao Y, Li JK, Luo HP, Zhou ZY, Ding DG, Wei D, Zhang JL. Clinical study of acupuncture in treating trigeminal neuralgia. Zhongguo Zhongyi Jizheng, 2008, 17(3): 323-325.
[20] Li J, Hou WG, Hong YF, Li HH, Qin LF. Clinical observation on warm needling plus Chinese herbal medicine for the treatment of trigeminal neuralgia. Shanghai Zhenjiu Zazhi, 2009, 28(6): 316-318.
Translator: Han Chou-ping
R246.6
A
Date: October 8, 2012
Author: Bao Hong, chief physician. E-mail: baohong_32@yahoo.com.cn
 Journal of Acupuncture and Tuina Science2013年1期
Journal of Acupuncture and Tuina Science2013年1期
- Journal of Acupuncture and Tuina Science的其它文章
- Acupuncture-moxibustion Theories of Wang Shu-he
- Treatment of Tolosa-Hunt Syndrome with Acupuncture: A Case Report
- Research Progress of Acupuncture Analgesia for Labor
- Clinical Study on Puncturing Houxi (SI 3) Toward Hegu (LI 4) plus Lumbar Movement for Acute Lumbar Sprain
- Therapeutic Effect of Warm Needling Therapy Combined with Rehabilitation Therapy for Brachial Plexus Injury after Surgery
- Electroacupuncture in Treating Depression: A Randomized Controlled Study