
Dosimetry Comparison between Volumetric Modulated Arc Therapy with RapidArc and Fixed Field Dynamic IMRT for Local-Regionally Advanced Nasopharyngeal Carcinoma
2011-07-18 11:26:06BaominZhengXiaoxiaDongHaoWuYoujiaDuanShukuiHanYanSun
Bao-min Zheng, Xiao-xia Dong, Hao Wu, You-jia Duan, Shu-kui Han, Yan Sun
Key Laboratory of Carcinogenesis and Translational Research (Ministry of Education), Department of Radiotherapy, Peking University School of Oncology, Beijing Cancer Hospital & Institute, Beijing 100142, China
Dosimetry Comparison between Volumetric Modulated Arc Therapy with RapidArc and Fixed Field Dynamic IMRT for Local-Regionally Advanced Nasopharyngeal Carcinoma
Bao-min Zheng, Xiao-xia Dong, Hao Wu, You-jia Duan, Shu-kui Han, Yan Sun*
Key Laboratory of Carcinogenesis and Translational Research (Ministry of Education), Department of Radiotherapy, Peking University School of Oncology, Beijing Cancer Hospital & Institute, Beijing 100142, China
Objective: A dosimetric study was performed to evaluate the performance of volumetric modulated arc radiotherapy with RapidArc on locally advanced nasopharyngeal carcinoma (NPC).
Methods: The CT scan data sets of 20 patients of locally advanced NPC were selected randomly. The plans were managed using volumetric modulated arc with RapidArc and fixed nine-field coplanar dynamic intensity-modulated radiotherapy (IMRT) for these patients. The dosimetry of the planning target volumes (PTV), the organs at risk (OARs) and the healthy tissue were evaluated. The dose prescription was set to 70 Gy to the primary tumor and 60 Gy to the clinical target volumes (CTV) in 33 fractions. Each fraction applied daily, five fractions per week. The monitor unit (MU) values and the delivery time were scored to evaluate the expected treatment efficiency.
Results: Both techniques had reached clinical treatment’s requirement. The mean dose (Dmean), maximum dose (Dmax) and minimum dose (Dmin) in RapidArc and fixed field IMRT for PTV were 68.4±0.6 Gy, 74.8±0.9 Gy and 56.8±1.1 Gy; and 67.6±0.6 Gy, 73.8±0.4 Gy and 57.5±0.6 Gy (P<0.05), respectively. Homogeneity index was 78.85±1.29 in RapidArc and 80.34±0.54 (P<0.05) in IMRT. The conformity index (CI: 95%) was 0.78±0.01 for both techniques (P>0.05). Compared to IMRT, RapidArc allowed a reduction of Dmeanto the brain stem, mandible and optic nerves of 14.1% (P<0.05), 5.6% (P<0.05) and 12.2% (P<0.05), respectively. For the healthy tissue and the whole absorbed dose, Dmeanof RapidArc was reduced by 3.6% (P<0.05), and 3.7% (P<0.05), respectively. The Dmeanto the parotids, the spinal cord and the lens had no statistical difference among them. The mean MU values of RapidArc and IMRT were 550 and 1,379. The mean treatment time of RapidArc and IMRT was 165 s and 447 s. Compared to IMRT, the delivery time and the MU values of RapidArc were reduced by 63% and 60%, respectively.
Conclusion: For locally advanced NPC, both RapidArc and IMRT reached the clinic requirement. The target volume coverage was similar for the different techniques. The RapidArc technique showed some improvements in OARs and other tissue sparing while using reduced MUs and delivery time.
Volumetric modulated arc therapy; Intensity-modulated radiotherapy; Dosimetry; Target volume; Nasopharyngeal carcinoma
INTRODUCTION
Recently, nasopharyngeal carcinoma (NPC) patients more likely have received intensity-modulated radiotherapy (IMRT) than three dimensionals’ conformal radiotherapy (3D-CRT). The IMRT has got better dose distribution in target volume and lower dose for organs at risk (OARs), especially for the parotids[1-3]. But IMRT iiiiiiiiiiineeds complex plan management, more fixed fields and monitor units (MUs) especially for NPC which has large target volume, more OARs and more overlapping of target volume. All of the above may bring the prolonging of the treatment time (for example, 7–9 fixed-field dynamic IMRT needs about 7–10 minutes of treatment delivery) which may cause the increasing of the movement of the swallowing and the position shift during the treatment, so that the clinical efficacy may be reduced consequently.
Generally, the number of the fixed fields can increase the freedom of the plan management, and the development of the volumetric modulated arc therapytechnique brings the design of the treatment plan to a new stage which can produce various optimization methods based on the differences of the peak value optimization[4]. Nowadays, RapidArc was developed mainly by the optimization of the multi-leaf collimators shape, the change of the dose rate delivery and the rotation of the gantry[5-8]. It was based on the volumetric modulated arc therapy technique and can obtain the similar distribution of the fixed IMRT. The analytical anisotropic algorithm (AAA) system was used for dose calculation[9], and GLAaS[10]and PTW-729[11]methods were applied for quality control to ensure the accuracy and security in the clinical application[12].
Currently, multiple centers compared the dose distribution of the both techniques and generally suggested that volumetric modulated arc therapy with RapidArc was a rapid, safe and accurate radiotherapy technique for many tumors like gliomas, brain metastases and some lung tumors according to the preliminary results[13-17].
NPC needs large and complex target volume and has many OARs around, so that complicated fields’management was necessary. Therefore, in this study, RapidArc was compared at the reference of the fixed 9-field IMRT in dosimetry for locally advanced NPC.
MATERIALS AND METHODS
Patients’ Characteristics
Twenty cases of location CT scan data (layer 3 mm) was randomly selected from the locally advanced NPC patients who had received radiotherapy (RT) continuously in Radiotherapy Department, Beijing Cancer Hospital. The patients’ characteristics are shown in Table 1, and the clinical stage was according to the Stage of NPC (AJCC 2002) followed as below. Among these 20 patients, three patients had been diagnosed as T4 and six patients as N3. The gross tumor volume (GTV) was ranged from 51.4 cm3to 421.8 cm3and the median volume was 130.9±83.2 cm3.
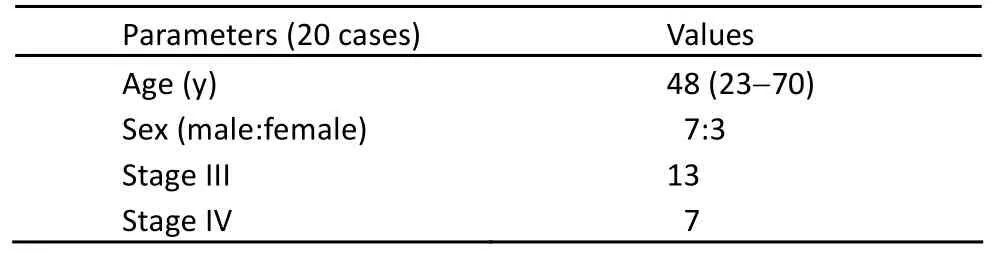
Table 1. Patients’ General and Clinical Characteristics
Treatment Plan Management
Two treatment plans were performed for each patient. RapidArc was compared to the fixed 9-field coplanar dynamic IMRT in dosimetry. The Eclipse system from the Varian Company (Denver, USA) was used for the two RT plans, with 6MV-X ray and 120 multi-leaf collimator in it. Considering the large target volume of the locally advanced NPC and complex OARs around, the double-arc plan was adopted for RapidArc and the coplanar fixed 9-field plan was selected for IMRT. Meantime, the AAA 8.6 edition system was applied for calculation.
The simultaneous boost plan was used and the dose prescribed as: GTV 70 Gy/33f, 95% planning target volume (PTV) 60 Gy/33f was generated by 5-mm outer margin of clinical target volume (CTV) and 5 mm apart from the skin at least.
The quality control of the plan was in accordance with the standard dose-volume histogram (DVH) of D98%and D2%which represent the doses of 98% and 2% PTV and they indicated the minimum and maximum doses of the plan respectively. The conformity index (CI) of the target volume is expressed as CI95%=(PTV60Gy/ VPTV)×(PTV60Gy/V60Gy)[18]. PTV60Gyrepresents the volume receiving the prescription dose 60 Gy in the target volume, VPTVstands for the volume of the PTV, V60Gyis in the name of the volume which has received the prescribed dose. The homogeneity index (HI) of the target volume is defined as HI=100×[1-(D5%-D95%)/ Dmean][15]. OARs, D33%, Dmean, D50%, and D66%were adopted to evaluate the dose distribution of both sides of the parotids. Dmeanand Dmax(the maximum dose which was defined as the dose received by less than 2 ml volume of the following OARs) were applied to evaluate the dose of the lens, spinal cord, mandible and optic nerves. For the healthy tissue, integrity absorption dose (DoseInt) was used as the evaluation standard accompanied by Dmeanand V10Gyat the same time. The time interval of the treatment delivery and the MU values of the techniques were also compared.
Statistical Analyses
The SPSS 13.0 (SPSS Inc., IL, USA) was applied for statistical data management and analysis, and doublesidet-test was employed to compare the difference between two treatment plans at statistically significant level ofP<0.05. The null hypothesis of no difference in dosimetry between study groups was tested with the use of the log-rank test at a two-sided level of significance of 0.05. Confidence intervals were calculated and study groups were compared by means of the log-rank test. All other hypothesis tests were two-sided at a significance level of 0.05.
RESULTS
Dosimetry Analysis of Target Volume
Table 2 shows the comparison of the dose distribution of the PTVs and the CI and HI of the target volumes. According to the clinical requirement, Dmeanand Dmaxof the PTV were lower while Dminwas slightly higher and statistically significant for IMRT. The CI95%of RapidArc and IMRT were both 0.78±0.07 (P>0.05). However, the HI for RapidArc and IMRT were 78.9±1.3 and 80.4±0.5, respectively (P<0.05).
Dosimetry Comparison of OARs and Healthy Tissues
Table 3 manifests the dose comparison of the OARs for the two plans. As we can see, the plans were similar in the mean dose of the spinal cord and had no differences at statistically significant levels (P<0.05). Withthe standard of the clinical treatment, the mean dose of RapidArc for the brain stem was really lower than that of IMRT; however, for the maximum dose, IMRT was indeed very low. The mean and maximum doses of the lens were similar in two plans and have no differences at statistically significant levels (P>0.05). For both sides of the optic nerves, the doses (except for the maximum dose of the right optic nerve) in RapidArc were less than that in IMRT, the differences were statistically significant atP<0.05 levels. The maximum doses for the mandible of the RapidArc and IMRT plans were similar in statistically significant level (P<0.05) with the mean doses less than 50 Gy for the both, while the former was lower at statistically significant levels (P<0.05) in the mean dose.

Table 2. PTV dose distribution comparison of two RT techniques
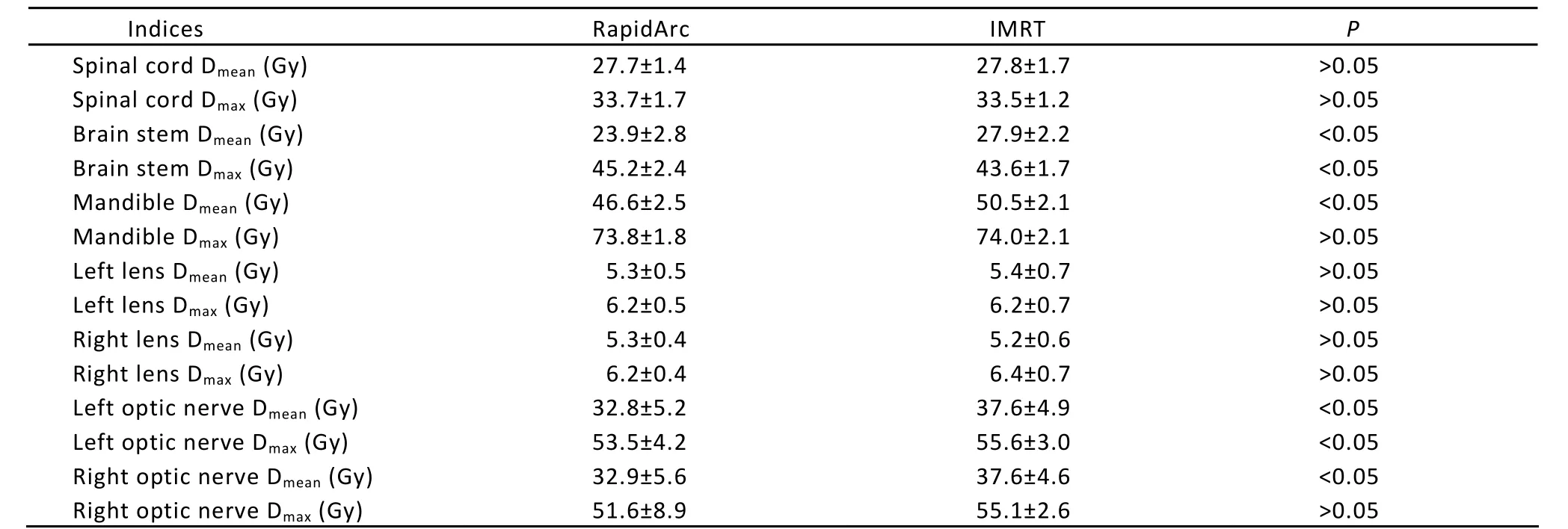
Table 3. Dose comparison of OARs for two plans
For both sides of the parotids, we performed detailed analysis in different volumes. The Dmean, D33%, D50%and D66%were all lower for IMRT. However, all of them above had no statistical differences between both sides of the parotids (Table 4). Figure 1 shows a demographic of the two different plans.
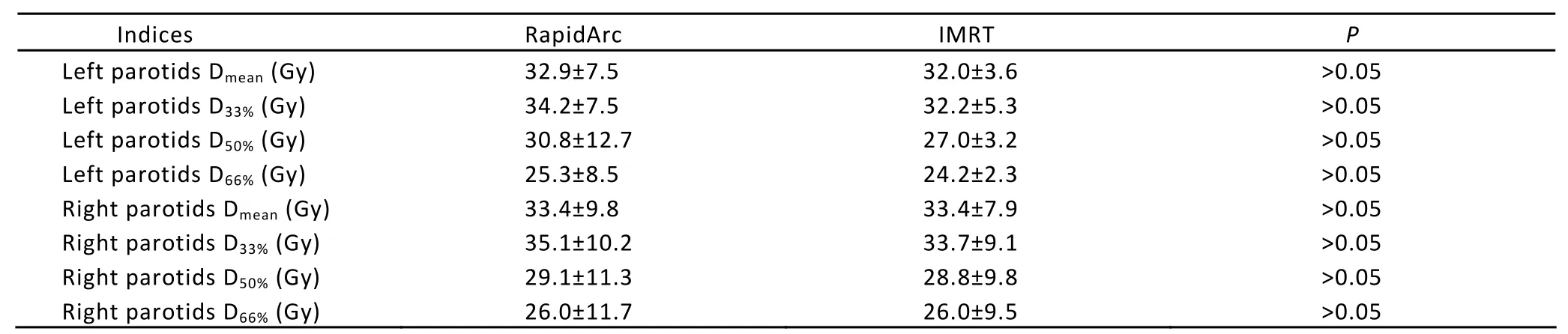
Table 4. Comparison of dose distribution for parotids
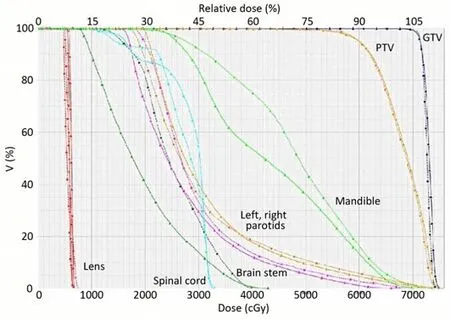
Figure 1. DVH for two treatment plans. The solid lines represent the doses of the different OARs and target volume in different volumes for RapidArc, and the dotted lines stand for those of IMRT. RapidArc appeared some priority in the mandible and the brain stem visually.
There was no clear definition of the radiation dose to the healthy tissue. But in principle, lower integrity absorption dose (DoseInt) and smaller radiation volume are better. The Dmeanand DoseInt were significantly lowered (P<0.05) for RapidArc. The radiation volume of 10 Gy was smaller for IMRT, but has no statistical significance (Table 5).
Comparison of MU Value and Treatment Time Interval
Figure 2 shows the MU values and time interval for the treatment plans. The mean MU value of RapidArc was 550, reduced by 60% compared to that of IMRT with the mean MU value of 1379. The mean treatment time of RapidArc was 165 s, reduced by 63% compared to that of IMRT with the mean time of 447 s.

Table 5. Dose comparison of the healthy tissue

Figure 2. The MU value and treatment time for the two plans.
DISCUSSION
As mentioned above, the treatment time interval is much shorter for RapidArc which may bring the promotion of the biologic effect. Although accuracy and repeatability of the RapidArc had been evaluated in some studies, there is no dose comparison for the two treatment plans in NPC patients currently.
In this research, the enrolled patients were satisfied with clinical treatment. The data of RapidArc implied that the dose distribution may be improved for some OARs and we can get more accurate plans, but this is not the point of the study. Moreover, in the program of the optimum, the weight for the target volume and the OARs were not clearly defined. Therefore, the dosimetry comparison for the two plans has its limitation.
The double-arc RapidArc was selected to guarantee the dose distribution due to a large targeting volume and lots of OARs for NPC patients. The reduction of the healthy tissue dose may decrease the risk of the secondary primary carcinoma, which needs follow up to clarify. The MU value was reduced by 60% meanly for RapidArc.
The result showed the 63% reduction of the mean treatment time can decrease the effect of the organ movement, and affect treatment effectiveness. In American Society for Therapeutic Radiology and Oncology (ASTRO) meeting in 2009, it was reported by Wang that the swallowing frequency was 3–19 times in one treatment fraction (11 minutes meanly in IMRT), the time interval was 4.8 secends for swallowing, and the shift of the target volume was 3.13–12.32 mm during the course. The data demonstrated that the position shift and the swallowing movement would inevitably lower the accuracy of the target volume because of the fairly long time interval for the treatment delivery of the head and neck cancer, thereby decreasing the clinical treatment effectiveness. Therefore, RapidArc can increase the accuracy of the radiotherapy and improve the effectiveness of the treatment by reducing the time interval of the delivery.
Furthermore, the reduction of the fraction treatment time may increase the biologic effect of radiotherapy. Shibamoto, et al.[19]showed that between two fractions of radiotherapy, sublethal repair occurred in 2–3 minutes or longer time, while using breast cancer cell strain EMT 6 and head and neck squamous cell strain SCCVn of micein vitro.
The previous data about RapidArc and fixed field IMRT showed that the treatment time interval was less than 2.5 minutes for RapidArc and about 7–9 minutes for the fixed field IMRT (7–9 fields generally). The superiority of RapidArc in this work was the obvious reduction of the MU value and the treatment time[20,21]. Therefore, we believe that RapidArc may promote the clinical result since it can reduce the shift of the patient location[20]and the influence of the swallowing movement on the OARs during the delivery.
To achieve satisfactory dose distribution, it will take more than 17 hours for the plan optimization to RapidArc for one locally advanced NPC while only 0.5–1 hour is needed for IMRT. Consequently, the calculation system for the RapidArc plan needs to be improved in future studies.
In conclusion, for the local advanced NPC, RapidArc can reach similar target conformity comparing to IMRT for target dose distribution and homogeneity, and IMRT is a little better than RapidArc. Compare to IMRT, though the parotids received higher dose for RapidArc, it would not damage parotids statistical significantly; brain stem, mandible and both sides of the optic nerves had better dose distribution in RapidArc plans; for the lens and spinal cord, the dose distribution was similar in both plans. Considering the mean dose of the healthy tissue and the integrity absorbed dose, RapidArc was superior to IMRT. The reduction of the treatment time and the MU value were notable for RapidArc.
Acknowledgement
Sincerely appreciate to Dr. Zheng Junxiu for the great help in the arrangement of the data and the modification of the writing for this article. Thanks again for her unselfish help.
REFERENCES
1. Kam KM, Chau RM, Suen J, et al. Intensity-modulated radiotherapy in nasopharyngeal carcinoma: dosimetric advantage over conventional plans and feasibility of dose escalation. Int J Radia Oncol Biol Phys 2003; 56: 145–57.
2. Chau RM, Teo PM, Kam MK, et al. Dosimetric comparison between 2-dimensional radiation therapy and intensity modulated radiation therapy in treatment of advanced T-stage nasopharyngeal carcinoma: to treat less or more in the planning organ-at-risk volume of the brainstem and spinal cord. Med Dosim 2007; 32:263-70.
3. Wu Q, Manning M, Schmidt-Ullrich R, et al. The potential for sparing of parotids and escalation of biologically effective dose with intensity-modulated radiation treatments of head-and-neck cancers: a treatment design study. Int J Rad Oncol Biol Phys 2000; 46:195-205.
4. Thieke C, Küfer KH, Monz M, et al. A new concept for interactive radiotherapy planning with multi-criteria optimization: First clinical evaluation. Radiother Oncol 2007; 85:292-8.
5. Ling CC, Zhang P, Archambault Y, et al. Commissioning and quality assurance of RapidArc radiotherapy delivery system. Int J Rad Oncol Biol Phys 2008; 72:575-81.
6. Berg M, Bangsgaard JP, Vogelius IS. Absorption measurements on a new cone beam CT and IMRT compatible tabletop for use in external radiotherapy. Phys Med Biol 2009; 54:319-28.
7. Otto K, Letter to the editor on ‘Single-Arc IMRT’? Phys Med Biol 2009; 54:L37-41.
8. Falk M, af Rosensch PM, Keall P, et al. Real-time dynamic MLC tracking for inversely optimized arc radiotherapy. Radiother Oncol 2010; 94:218-23.
9. Gagne IM, Ansbacher W, Zavgorodni S, et al. A Monte Carlo evaluation of RapidArc dose calculations for oropharynx radiotherapy. Phys Med Biol 2008; 53:7167-85
10. Nicolini G, Vanetti E, Clivio A, et al. The GLAaS algorithm for portal dosimetry and quality assurance of RapidArc, an intensity modulated rotational therapy. Radiat Oncol. 2008; 3:24.
11. Vanetti E, Nicolini G, Clivio A, et al. The impact of treatment couch modeling on RapidArc. Phys Med Biol. 2009; 54:157-66.
12. Korreman S, Medin J, Kjer Kristofferson F. Dosimetric verification of RapidArc treatment delivery. Acta Oncol 2009; 48: 185-91.
13. Otto K. Volumetric Modulated Arc therapy: IMRT in a single arc. Med Phys 2008; 35:310-7.
14. Shaffer R, Nichol AM, Vollans E, et al. A comparison of volumetric modulated arc therapy and conventional intensitymodulated radiotherapy for frontal and temporal high-grade gliomas. Int J Radiat Oncol Biol Phys 2010; 76:1177-84.
15. Lagerwaard FJ, Van Der Hoorn EA, Verbakel WF, et al. Wholebrain radiotherapy with simultaneous integrated boost to multiple brain metastases using volumetric modulated arc therapy. Int J Radiat Oncol Biol Phys 2009; 75:253-9.
16. Lagerwaard FJ, Meijer OW, Van Der Hoorn EA, et al. Volumetric modulated arc radiotherapy for vestibular schwannomas. Int J Rad Oncol Biol Phys 2009; 74:610-5.
17. Verbakel W, Senan S, Cuijpers JP, et al. Rapid delivery of stereotactic radiotherapy for peripheral lung tumors using volumetric intensity-modulated arcs. Radiother Oncol 2009;93:122-4.
18. Crijns W, Budiharto T, Defraene G, et al. IMRT-based optimization approaches for volumetric modulated single arc radiotherapy planning. Radiother Oncol 2010; 95:149-52.
19. Shibamoto Y, Ito M, Sugie C, et al. Reeovery from sublethal damage during iniermittent exposures in cultured tumor cells: imPlieations for dose modification in radiosurgery and imrt. Int J Radiat Oncol Biol Phys 2004; 59:1484-90.
20. Popescu CC, Olivotto IA, Beckham WA, et al. Volumertric modulated arc therapy improves dosimetry and reduces treatment time compared to conventional intensity- modulated radiotherapy of left-sided breast cancer and internal mammary nodes. Int J Radia Oncol Biol Phys 2010; 76:287-95.
21. Yoo S, Wu QJ, Lee WR, et al. Radiotherapy treatment plans with RapidArc for prostate cancer involving seminal vesicles and lymph node. Int J Radiat Oncol Biol Phys 2010; 76:935-42.
10.1007/s11670-011-0259-0
2011-03-16; Accepted: 2011-08-23
*Corresponding author.
E-mail: ysunemail@yahoo.com
?Chinese Anti-Cancer Association and Springer-Verlag Berlin Heidelberg 2011
 Chinese Journal of Cancer Research2011年4期
Chinese Journal of Cancer Research2011年4期
- Chinese Journal of Cancer Research的其它文章
- Prognostic Value of Promoter Hypermethylation of Retinoic Acid Receptor Beta (RARB) and CDKN2 (p16/MTS1) in Prostate Cancer
- Expression and Distribution Characteristics of Human Ortholog of Mammalian Enabled (hMena) in Glioma
- Changes of Serum Trace Elements, AFP, CEA, SF, T3, T4 and IGF-Ⅱ in Different Periods of Rat Liver Cancer
- Mast Cells in Adjacent Normal Colon Mucosa rather than Those in Invasive Margin are Related to Progression of Colon Cancer
- Wild-Type KRAS and BRAF Could Predict Response to Cetuximab in Chinese Colorectal Cancer Patients
- Hepatocellular Tumors: Immunohistochemical Analyses for Classification and Prognostication