
Liquid Chromatography-tandem Mass Spectrometry for Analysis of Acylcarnitines in Dried Blood Specimens Collected at Autopsy from Neonatal Intensive Care Unit
2010-11-22 02:36:26WenjunTuFangDaiXinyuWangYingLiandJamesJianHo
Chinese Medical Sciences Journal 2010年2期
Wen-jun Tu,Fang Dai,Xin-yu Wang,Ying Li,and James Jian Ho*
1Center for Clinical Laboratory Development,Chinese Academy of Medical Sciences &Peking Union Medical College,Beijing 102206,China
2Department of Pediatrics,Beijing Haidian Maternal &Child Health Hospital,Beijing 100080,China
INBORN errors of metabolism (IEMs) are a group of highly heterogeneous inherited diseases.Their birth prevalence was estimated at the range between 1/784 and 1/2 555.1Although relatively rare in the population in neonatal intensive care unit (NICU),these disorders are being increasingly identified and are responsible for significant morbidity and mortality.2For most of these disorders,the early symptoms and signs are non-specific.Patients presenting symptoms and signs are often at a life-threatening status and may die before diagnostic tests and management.Deaths probably attributable to metabolic disorders in NICU are usually undiagnosed at present because of technical constraints.As a solution to this problem,the application of liquid chromatography-tandem mass spectrometry (LC-MS/MS) in amino acid and acylcarnitine analysis of dried blood spots of newborns is quickly gaining worldwide support as the method of choice for the screening of IEMs.3-5This technology is also used for analysis of acylcarnitines in dried postmortem blood specimens collected at autopsy.6In the present study,we investigated the feasibility of analyzing acylcarnitine in dried postmortem blood specimens with LC-MS/MS.
MATERIALS AND METHODS
Blood specimens
All specimens used in this study were collected between October 1,2008 and September 30,2009.Four types of specimens were included:26 dried postmortem blood specimens prepared by applying 25 μL of blood,collected at autopsy or as soon as possible after death,to S&S Grade 903 filter paper;8 urine specimens collected when available;100 dried blood specimens from healthy newborns obtained at routine newborn screening;and 20 dried blood specimens from older (>30 days) patients with IEMs.The postmortem blood specimens were received from the NICU,Beijing Haidian Maternal &Child Health Hospital;the blood specimens from healthy newborns and IEM patients were obtained from Center for Clinical Laboratory Department,Chinese Academy of Medical Sciences &Peking Union Medical College.Written informed consents were signed by the children’s parents before collection of specimens.
Solvents,reagents,and internal standards
Reagents used in this study included high performance liquid chromatography (HPLC)-grade solvents,methanol,acetonitrile,n-butanol,and acetyl chloride.Butanolic HCl(3 mol/L) was prepared withn-butanol and acetyl chloride in the proportion of 9∶1 (v/v).Purity of the nitrogen used was 99.999%.One 96-well filter plate and one 96-well polypropylene plate were purchased from Agilent (CA,USA).The 20 isotopic internal standards were purchased from Cambridge Isotope Laboratories (MA,USA).These internal standards were diluted with methanol to prepare the working calibration solution,which was then stored at 4°C.
Sample preparation
From each dried blood filter-paper sample,a disc of 3 mm in diameter was punched and placed on a 96-well filter plate.Altogether 300 μL of methanol containing the amino acid and acylcarnitine isotopic internal standards was added into each well.After 30 minutes at room temperature,the amino acid and acylcarnitine in blood filter-paper were extracted and diverted into a 96-well polypropylene plate.All wells were dried at 50°C under nitrogen flow and to each 50 μL butanolic HCl was added with an Eppendorf pipette (Hamburg,Germany).The plate was then covered by a Teflon membrane (Beijing,china) and heated to 65°C for exactly 15 minutes.After drying with 50°C nitrogen evaporators,100 μL of 80% acetonitrile was added to each well and the plate was covered by an aluminum membrane prior to run in spectrometer and chromatograph.
Liquid chromatography-tandem mass spectrometry(LC-MS/MS)
The equipment applied in this study were an API 3000 tandem mass spectrometer (Applied Biosystems,CA,USA)and an Agilent 1100 high performance liquid chromatograph.
Sample at a volume of 20 μL were injected at 2-minute intervals in a flowing stream of 80% acetonitrile.Quaternary pump flow rate was set at 30 μL/min.These scanning models were used for each examination.For amino acids,the neutral loss scan (mass to charge ratio,m/z:102) was used with the scanning range ofm/zbeing 140-280.For acylcarnitines,the precursor scan of the production (m/z:85)was used with the scanning range ofm/zbeing 210-502.For glycine,ornithine,arginine,and citrulline,multiple reaction monitoring was used.
Resultsfrom a mass spectrometer were displayed in a mass spectrum in which the horizontal axis represented them/zand the vertical axis represented the quantity of ions.With the addition of internal standards that are chemically the same as the molecules of interest but different by 3 or more mass units,the concentration of individual metabolites can be measured and quantified.Our laboratory routinely calculate the concentrations of more than 65 metabolites and metabolite concentration ratios (molar ratios)when analyzing acylcarnitines and amino acids.
Result processing
The LC-MS/MS methodology used in this study was transferred from Pediatrix Inc (formerly known as NeoGen screening Inc).The levels of amino acids and acylcarnitines were automatically calculated using ChemoView1.2 software based on the assigned values of the isotopic internal standards.In addition to the analytical results from LC-MS/MS,the diagnosis of the disorder was further confirmed by gas chromatography-mass,other laboratory tests,and routine autopsy results.
RESULTS
General information
The 26 infants died included 15 males and 11 females,the median age being 3 days (range,1-27 days).The median gestation was 36 weeks (range,31-40 weeks);median birth weight 2 440 g (range,1 390-4 100 g).The most frequent first diagnoses were septicemia (6,23.1%),respiratory distress syndrome (5,19.2%),and very low birth weight (5,19.2%).
Based on the 26 postmortem blood specimens,5 cases(19.2%) were diagnosed with IEMs,including 3 methylmalonic acidemia (MMA),1 maple syrup urine disease(MSUD),and 1 isovaleric acidemia (IVA).Medical information of the five patients is shown in Table 1.
Analysis of control specimens
Figure 1 displays the tandem mass spectra of amino acids and acylcarnitines obtained during typical analyses of dried blood from healthy newborns.As shown in the acylcarnitine profiles in Figure 2,the concentration of C3 obviously increased in patients with MMA.Tandem mass spectra from postmortem blood specimens were predominantly characterized by increased free carnitine and short-chain acylcarnitines,e.g.,C2,C3,C4,and C5,as well as hydroxybutyryl carnitines.
Amino acid disorders
In nearly all postmortem blood specimens,we observed nonspecific,generalized large increases of most amino acids in amino acid profiles,similar as the one in Figure 3A.It was thought that those increases were not generally diagnostic for amino acidopathies.However,one exception was observed in which leucine-isoleucine rose to an extremely high level (Fig.3B).That specimen was diagnosed as MSUD.
Table 1.Medical information of the 5 patients with inborn errors of metabolism
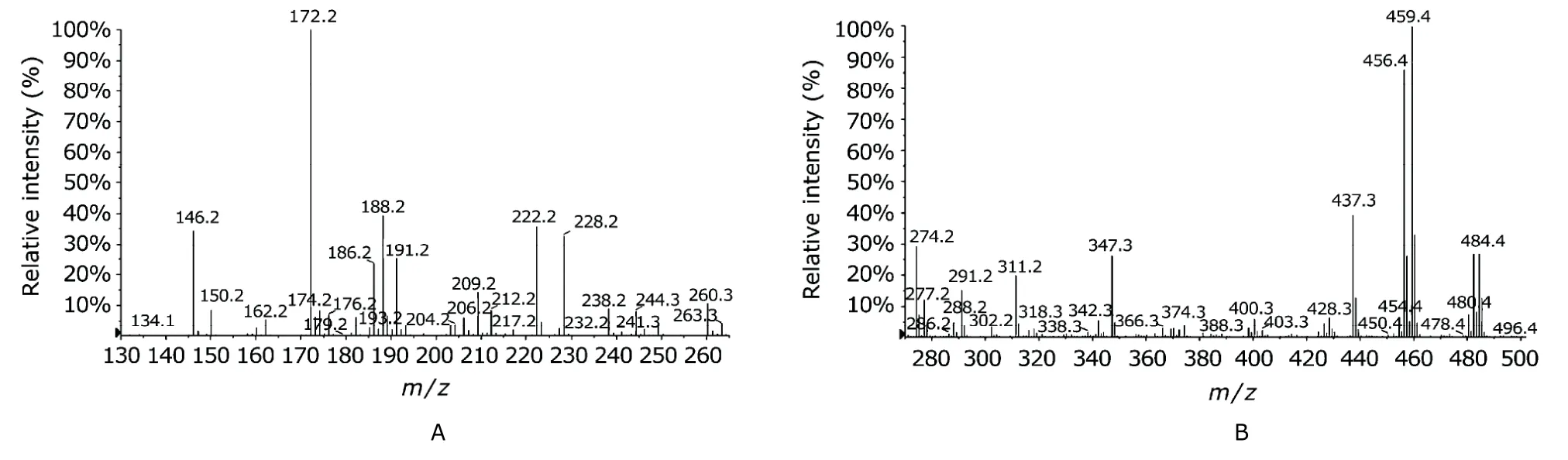
Figure 1.Acylcarnitine profiles (A) and amino acid profiles (B) of a dried blood specimen from a healthy newborn.m/z:mass to charge ratio.
Organic acid disorders
A substantial increase of C3,C3/C16,and C3/C2 was observed in three postmortem blood specimens.Based on the acylcarnitine profile,MMA was suspected (Fig.4A),yet the increase of C3 was not direct evidence of MMA or cobalamin deficiency.Analysis of urine,if available,would be required for confirmation of the exact metabolic disorder.The urine specimens of these three patients were collected and analyzed with gas chromatography mass spectrometry(GC-MS).Many postmortem specimens revealed increased concentrations of C3,C2,and C16,but the ratios of C3/C2 and C3/C16 were normal,hence a normal result.These two ratios are critical for reducing false-positive postmortem results.
One patient was suspected of having IVA.Substantial increase of C5 and C5/C2 ratio was observed (Fig.4B).It is important to note that without additional confirmation,we could not decide upon the specific type of disorder because C5 might be either isovalerylcarnitine or 2-methylbutyrylcarnitine.Analysis of urine with GC-MS was also required when available.
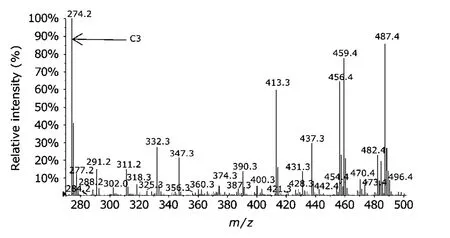
Figure 2.Acylcarnitine profiles of a dried blood specimen from an older patient with methylmalonic acidemia.
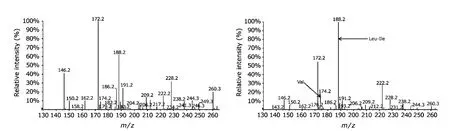
Figure 3.Amino acid profiles of a normal postmortem dried blood specimen (A) and a specimen from a dead infant suspected of maple syrup urine disease (B).
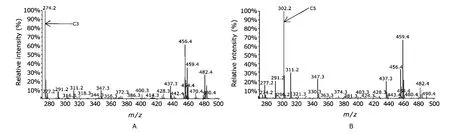
Figure 4.Postmortem acylcarnitine profiles of dried blood specimens from newborns diagnosed with methylmalonic acidemia (A) or isovaleric acidemia (B).
DISCUSSION
Blood specimens were used in the present study since the preparation is relatively simple,and because they are additionally advantageous in allowing DNA extraction for genetic testing.The analysis process in this study is very similar to approaches used in newborn screening,but the results produced are quite different.Analyzing the results of LC-MS/MS requires both the experience in visual interpretation of results and the assistance of automated computer interpretation using many of other parameters.
In our NICU,19.2% of the deaths were caused by IEMs,basically the same as the result reported by Zhang et al.7The incidence was similar to the reported 16.1% incidence of respiratory distress syndrome,the 17.4% incidence of serious asphyxia,both the latter two being common in NICU.8Given the specific target population of Haidian Maternal &Child Health Hospital,the proportion of IEMs in deaths may be higher than that in a larger population.A multicenter approach would be recommended to integrate more information from NICUs of other hospitals for a better understanding of the incidence of IEMs.With a larger body of specimens,the data would be more solid to demonstrate the percentage of deaths from a specific metabolic disorder in all-cause deaths in NICU.
Many patients with IEM present overwhelming symptoms in the first days of life.9,10Patients appear normal at birth,but gradually begin to have feeding difficulties together with vomiting,and progress to lethargy,coma,and death.The sooner clinical symptoms present,the higher the mortality.All of the 5 cases observed in our study died at less than 7 days.Our findings include organic acidemias(3 with MMA and 1 with IVA) and amino acid disorders (1 with MSUD),but no fatty acid oxidation (FAO) disorders.FAO disorders,for example,medium chain acyl-CoA dehydrogenase deficiency,short chain hydroxy acyl-CoA dehydrogenase deficiency,can also cause deaths in NICUs.10,11Although our study did not include all kinds of disorders,combining the results from other research,12we have reason to suspect that FAO disorders might be rare and organic academias are more common in our region.
In screening postmortem specimens for metabolic disorders,we can provide benefits to future early screening.Parents may be offered genetic counseling and family planning according to the screening result.6It is also conducive to improvement of pediatrician practice and public health service because the number of deaths in NICUs attributable to IEMs may begin to be assessed.It is hoped that screening inborn errors of metabolism by LC-MS/MS can be considered for routine use in NICUs autopsy.
Given the objective conditions allowed,our study has some limitation.First,the sample was small and all the specimens were from one center.Second,confirmatory testing of many metabolic disorders were not performed because molecular analyses,enzyme assays,and cell culture studies,which are required for that purpose,are not available in our laboratory.Third,confirmatory testing(urine sample analysis with GC-MS) is not provided in our laboratory.
In conclusion,the importance of developing a routine method for postmortem metabolic screening cannot be overestimated in the investigation of death in NICUs,and LC-MS/MS is an appropriate choice.Even though IEMs are considered to be relatively infrequent cause of neonatal death,its incidence might be actually higher than what is usually estimated,even as frequent as respiratory distress syndrome in some NICUs.Metabolic autopsy is therefore recommended for deaths in NICUs.
1.Campeau PM,Scriver CR,Mitchell JJ.A 25-year longitudinal analysis of treatment efficacy in inborn errors of metabolism.Mol Genet Metab 2008;95:11-6.
2.Jouvet P,Touati G,Lesage F,et al.Impact of inborn errors of metabolism on admission and mortality in a pediatric intensive care unit.Eur J Pediatr 2007;166:461-5.
3.Frazier DM,Millington DS,McCandless SE,et al.The tandem mass spectrometry newborn screening experience in North Carolina:1997-2005.J Inherit Metab Dis 2006;29:76-85.
4.Yoon HR,Lee KR,Kang S,et al.Screening of newborns and high-risk group of children for inborn metabolic disorders using tandem mass spectrometry in South Korea:a three-year report.Clin Chim Acta 2005;354:167-80.
5.Schulze A,Lindner M,Kohlmüller D,et al.Expanded newborn screening for inborn errors of metabolism by electrospray ionization-tandem mass spectrometry:results,outcome,and implications.Pediatrics 2003;111:1399-406.
6.Chace DH,DiPerna JC,Mitchell BL,et al.Electrospray tandem mass spectrometry for analysis of acylcarnitines in dried postmortem blood specimens collected at autopsy from infants with unexplained cause of death.Clin Chem 2001;47:1166-82.
7.Zhang W,Ma YL,Ma JR,et al.Clinical features and analysis of inherited metabolic diseases in neonatal intensive care unit.Chin J Med 2006;41:29-31.
8.Kang W,Liu DP,Chen YH,et al.Analysis of neonatal death in NICU during the latest 5 years.Chin Pediatr Emergency Med 2009;16:454-5.
9.Sniderman LC,Lambert M,Giguère R,et al.Outcome of individuals with low-moderate methylmalonic aciduria detected through a neonatal screening program.J Pediatr 1999;134:675-80.
10.Ding JH,Roe CR,Iafolla AK,et al.Diagnosis of medium chain acyl-CoA dehydrogenase deficiency in children dying suddenly without explanation by mutation analysis in post-mortem fixed tissue.N Engl J Med 1991;325:61-2.
11.Wilcken B,Haas M,Joy P,et al.Outcome of neonatal screening for medium-chain acyl-CoA dehydrogenase deficiency in Australia:a cohort study.Lancet 2007;369:37-42.
12.Han LS,Ye J,Qiu WJ,et al.Selective screening for inborn errors of metabolism on clinical patients using tandem mass spectrometry in China:a four-year report.J Inherit Metab Dis 2007;30:507-14.
 Chinese Medical Sciences Journal2010年2期
Chinese Medical Sciences Journal2010年2期
- Chinese Medical Sciences Journal的其它文章
- Pure Mucinous Carcinoma of the Breast:a Clinicopathologic Analysis with 56 Patients
- D-Tyr-tRNATyr Deacylase,a New Role in Alzheimer’sassociated Disease in SAMP8 Mice△
- Antagomir Dependent MicroRNA-205 Reduction Enhances Adhesion Ability of Human Corneal Epithelial Keratinocytes△
- Nectin-like Molecule 1 Inhibits the Migration and Invasion of U251 Glioma Cells by Regulating the Expression of An Extracellular Matrix Protein Osteopontin△
- A Second Protein Marker of Caveolae:Caveolin-2△
- Role of Acetylated p53 in Regulating the Expression of map2 in Retinoic Acid-induced P19 Cells△