
Preoperative controlling nutritional status as an optimal prognostic nutritional index to predict the outcome for colorectal cancer
2024-03-07 08:46:40LiXiangLiuHaoWangBoGaoTingTingXuQingGangYuanShiZhenZhouChaoDingJiMiaoWenXianGuan
Li-Xiang Liu,Hao Wang,Bo Gao,Ting-Ting Xu,Qing-Gang Yuan,Shi-Zhen Zhou,Chao Ding,Ji Miao,Wen-Xian Guan
Abstract BACKGROUND The controlling nutritional status (CONUT) score effectively reflects a patient’s nutritional status,which is closely related to cancer prognosis.This study investigated the relationship between the CONUT score and prognosis after radical surgery for colorectal cancer,and compared the predictive ability of the CONUT score with other indexes.AIM To analyze the predictive performance of the CONUT score for the survival rate of colorectal cancer patients who underwent potentially curative resection.METHODS This retrospective analysis included 217 patients with newly diagnosed colorectal.The CONUT score was calculated based on the serum albumin level,total lymphocyte count,and total cholesterol level.The cutoff value of the CONUT score for predicting prognosis was 4 according to the Youden Index by the receiver operating characteristic curve.The associations between the CONUT score and the prognosis were performed using Kaplan-Meier curves and Cox regression analysis.RESULTS Using the cutoff value of the CONUT score,patients were stratified into CONUT low (n=189) and CONUT high groups (n=28).The CONUT high group had worse overall survival (OS) (P=0.013) and relapse-free survival (RFS) (P=0.015).The predictive performance of CONUT was superior to the modified Glasgow prognostic score,the prognostic nutritional index,and the neutrophil-to-lymphocyte ratio.Meanwhile,the predictive performances of CONUT+tumor node metastasis (TNM) stage for 3-year OS [area under the receiver operating characteristics curve (AUC)=0.803] and 3-year RFS (AUC=0.752) were no less than skeletal muscle mass index (SMI)+TNM stage.The CONUT score was negatively correlated with SMI (P < 0.01).CONCLUSION As a nutritional indicator,the CONUT score could predict long-term outcomes after radical surgery for colorectal cancer,and its predictive ability was superior to other indexes.The correlation between the CONUT score and skeletal muscle may be one of the factors that play a predictive role.
Key Words: Controlling nutritional status;Colorectal cancer;Prognostic marker;Sarcopenia;Skeletal muscle
lNTRODUCTlON
Colorectal cancer is the third most common cancer in the world and ranks second in cancer-related deaths despite improvements in treatment[1,2].Therefore,identifying effective tools in prognostic prediction for colorectal cancer is warranted.Especially after radical colorectal cancer surgery.Early risk stratification contributes to individualized treatment and overall prognosis.
Several studies have shown that a decline in nutritional status hinders recovery after surgery,thus leading to poor prognosis[3,4].The decline of nutritional status leads to the disorder of net protein balance in the body,when protein synthesis is insufficient to compensate for protein decomposition,thus affecting the muscle content of the body[5].Sarcopenia occurs when the muscle content is reduced and has been confirmed as an independent risk factor for multiple cancers in several studies[6-9].Currently,sarcopenia is mainly diagnosed by analyzing computed tomography (CT) images of the third vertebral slice.However,the CT method of skeletal muscle measurement has many drawbacks,including high expense,radiation exposure,and sophisticated manipulation,which largely restricts its wide application.Therefore,a series of nutrition-related scoring tools,such as controlling nutritional status (CONUT),modified Glasgow prognostic score (mGPS),prognostic nutritional index (PNI),neutrophil-to-lymphocyte ratio (NLR),and others have been developed to replace muscle measurement depending on serological indicators.Moreover,studies have shown that these nutrition-related scores can be used to evaluate the prognosis of patients with colorectal cancer[10-13].However,their predictive performance varies between studies.Therefore,we need a convenient and relatively accurate nutrition-related scoring tool to evaluate the prognosis of patients with colorectal cancer.
A new nutritional scoring tool proposed in recent years,the CONUT score has been proven effective in assessing the nutritional status of patients[14].The calculation of the CONUT score is based on serum albumin level,total peripheral lymphocyte counts,and total cholesterol level as previously described[15].These serum indicators are readily available and convenient for clinical evaluation.According to recent studies,the CONUT score can be used to predict the outcome of a variety of cancers including gastric cancer[16],urinary system cancer[17],and lung cancer[18].Although the predictive value of the CONUT score for the long-term prognosis of colorectal cancer after radical surgery has been reported,the mechanism of the CONUT score’s predictive power remains unclear.At the same time,compared with other nutrition-related scoring tools that rely on serological indicators,the accuracy of its predictive power has not been clearly reported.
This study aimed to analyze the predictive performance of the CONUT score for the survival rate of colorectal cancer patients who underwent potentially curative resection.Meanwhile,we also compared the prognostic ability of the CONUT score with other nutritional scoring systems in predicting the long-term outcome after radical surgery for colorectal cancer and explored the mechanism of the CONUT score’s predictive power.
MATERlALS AND METHODS
Patients
A database comprised of 373 patients newly diagnosed with colorectal cancer who underwent surgery in Nanjing Drum Tower Hospital or General Hospital of Eastern Theater Command between January 2015 and January 2019 was analyzed retrospectively.Patients with pre-operative neoadjuvant chemotherapy,absent of pre-operative CT images,tumor node metastasis (TNM) stage IV,incomplete medical records,or lost during routine follow-up were excluded.This observational study was approved by the Clinical Research Ethics Committee of Nanjing Drum Tower Hospital and General Hospital of Eastern Theater Command.Written informed consent was obtained.
Laboratory tests were based on fasting blood collected on the morning of the first day of admission.American Joint Committee on Cancer stage was assessed according to the eighth version of the TNM staging system.Comorbidities included tuberculosis,hepatitis,diabetes,hypertension,coronary heart disease,hyperlipidemia,and other chronic diseases.Postoperative complications were defined as intestinal obstruction,intestinal paralysis,anastomotic leakage,abdominal infection,and other setbacks during the perioperative period.
The CONUT score
The CONUT score was calculated as previously described and illustrated in Table 1[14].The CONUT is assessed using serum albumin,lymphocyte counts,and total cholesterol.A CONUT score ≥ 5 was considered a state of moderate to severe malnutrition.
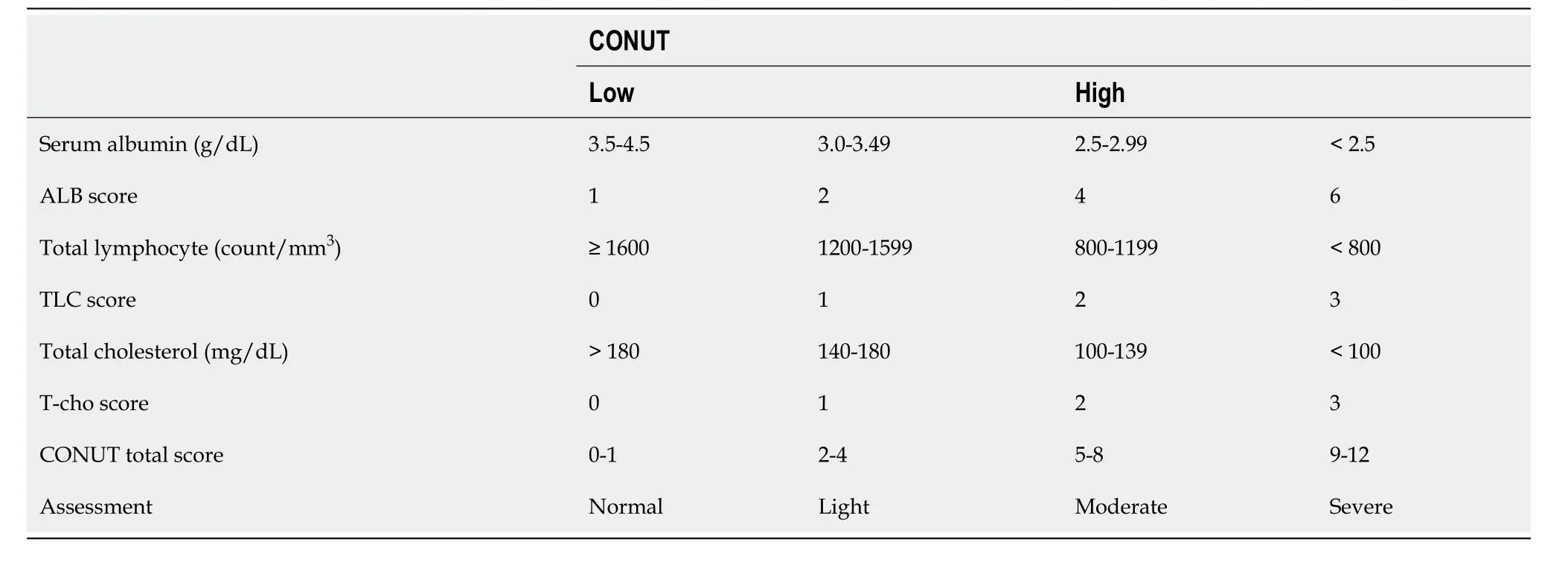
Table 1 Definition of the controlling nutritional status
Skeletal muscle mass index
The skeletal muscle area (SMA) was measured using ImageJ software to measure the areas of the psoas major,paraspinal muscles,transverse abdominis,external oblique,internal oblique,and rectus abdominis in the cross-section of the third lumbar vertebrae on CT[19] (Figure 1).The skeletal muscle mass index (SMI) was calculated by dividing SMA (cm2) by the square of height (m).Sarcopenia was defined as SMI < 40.8 (cm2/m2) in men and SMI < 34.9 (cm2/m2) in women[8].
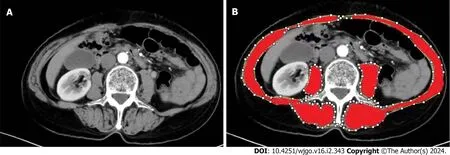
Figure 1 The measurement of skeletal muscle area.A: The third lumbar vertebra on CT;B: The regions marked in red are the skeletal muscles,including the psoas major,paraspinal,transverse abdominis,external oblique,internal oblique,and rectus abdominis.
Other nutritional scoring systems
The NLR was calculated as the ratio of pre-operative neutrophil and lymphocyte counts[12].The mGPS was scored using pre-operative C-reactive protein (CRP) and albumin levels.Patients were divided into three categories by mGPS: 0 (CRP ≤ 10 mg/L and albumin ≥ 35 g/L),1 (CRP >10 mg/L or albumin < 35 g/L),and 2 (CRP > 10 mg/L and albumin < 35 g/L)[10].The PNI was calculated based on preoperative albumin and lymphocyte counts: 10 × albumin (g/dL)+0.005 × total lymphocyte counts (per mm3)[20].The scores listed above are nutritional evaluation systems considered useful in cancer prognostic risk stratification[10-13].
Follow up
Patients who underwent colorectal cancer surgery and were discharged from the hospital were followed by telephone every three months.Regular return and follow-up at the hospital were also required.The primary endpoint was death from all causes of illness.The secondary endpoint was medically proven recurrence.
Statistical analysis
IBM SPSS Statistics for Windows,Version 26.0 (Armonk,NY: IBM Corp) was used for statistical analysis.The correlations between parameters were examined using Pearson's or Spearman's correlation coefficient when appropriate.Differences between groups were assessed byχ2test or analysis of variance.The Kaplan-Meier curve was used to analyze 3-year overall survival (OS) and 3-year relapse-free survival (RFS).Cox proportional hazards models were utilized to identify variables with significant independent associations with OS and RFS.The time-dependent receiver operating characteristic (ROC) curve was used to evaluate the accuracy of prognosis prediction and was compared using the DeLong test between different scores.P< 0.05 was considered significantly different.
RESULTS
Clinical characteristics
Among the 217 patients with colorectal cancer,92 (42.4%) were men and 125 (57.6%) were women,with a mean age of 58.4 years (range 24-88).Based on the time-dependent ROC,the best cutoff value of the CONUT score for predicting 3-year OS was 4.Therefore,patients were divided into CONUT low (CONUT ≤ 4) (n=189,87.1%) and CONUT high groups (CONUT ≥ 5) (n=28,12.9%).Characteristics were compared between the two groups.
The age,sex,tumor site,rates of comorbidities,pre-operative white blood cell count,platelet count,serum carcinoembryonic antigen,and carbohydrate antigen 19-9 levels between the two groups were not significantly different.Patients in the CONUT HIGH group showed a later tumor TNM stage (P=0.044),had a higher incidence of postoperative complication rates (P=0.044),higher CRP levels,and lower body mass index,hemoglobin,albumin,and cholesterol levels.The incidence of sarcopenia in the CONUT HIGH group was also higher (Table 2).
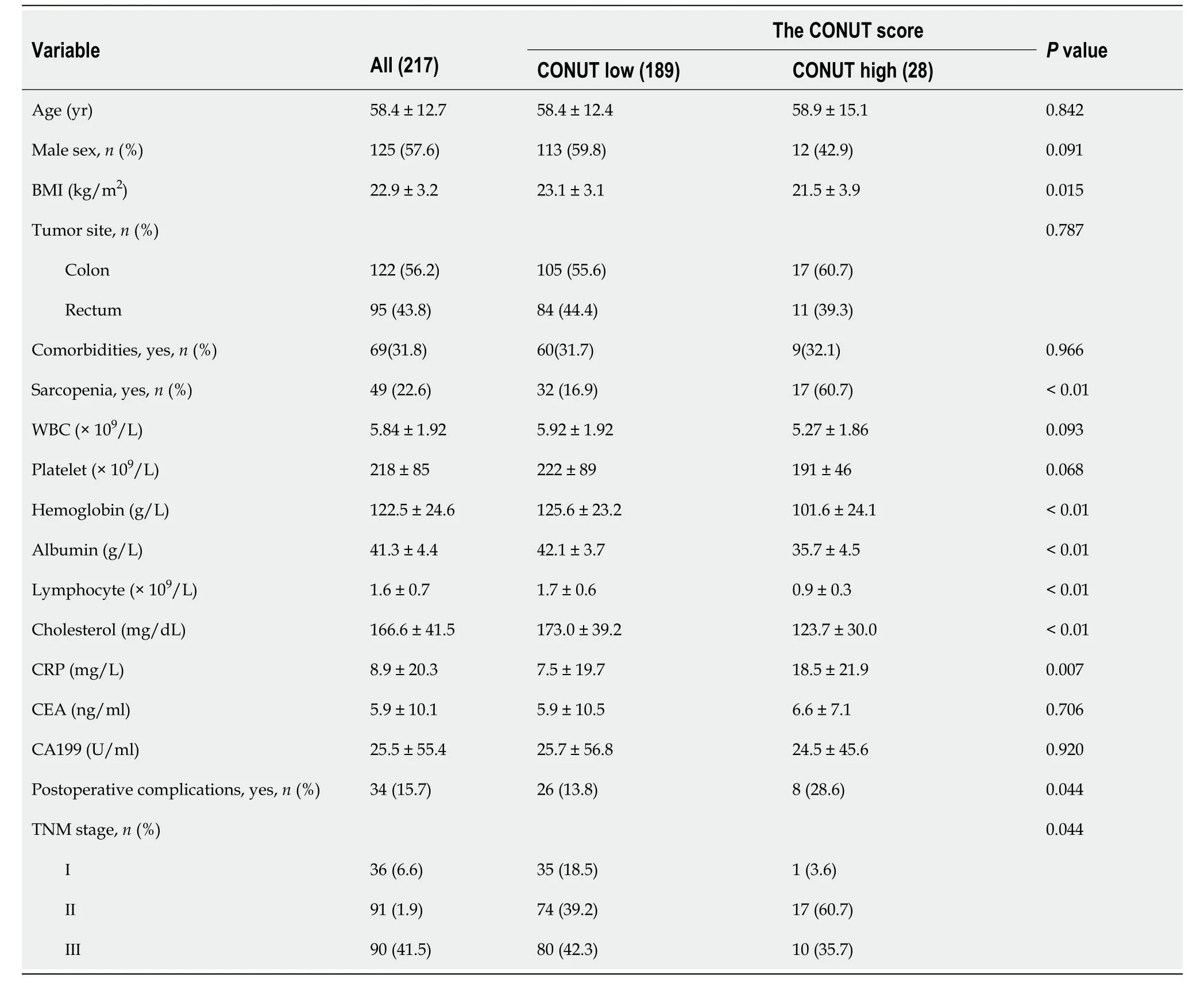
Table 2 Clinicopathological characteristics of 217 patients with colorectal cancer after surgery
CONUT and survival
Median follow-up was 49.6 mo (8-85 mo).The 3-year OS (94.1%vs71.4%,P<0.01) and RFS (89.9%vs64.2%,P< 0.01) of the CONUT low group were significantly higher than those in the CONUT high group.Due to the high mortality and recurrence rate of colon cancer in stage III patients,we analyzed stage III patients separately to better explore the relationship between the CONUT score and patient prognosis.In patients with TNM stage III,the 3-year OS and RFS in the CONUT low were also significantly higher than those in the CONUT high group (90%vs40%,P< 0.01;83.7%vs40%,P<0.01).There was a significant difference in the 3-year RFS between CONUT low and high in patients with TNM stages I-II (P< 0.01),but not with 3-year OS (P=0.08;Figure 2).This may be due to lower mortality and a relatively short follow-up period for participants in stage I-II.
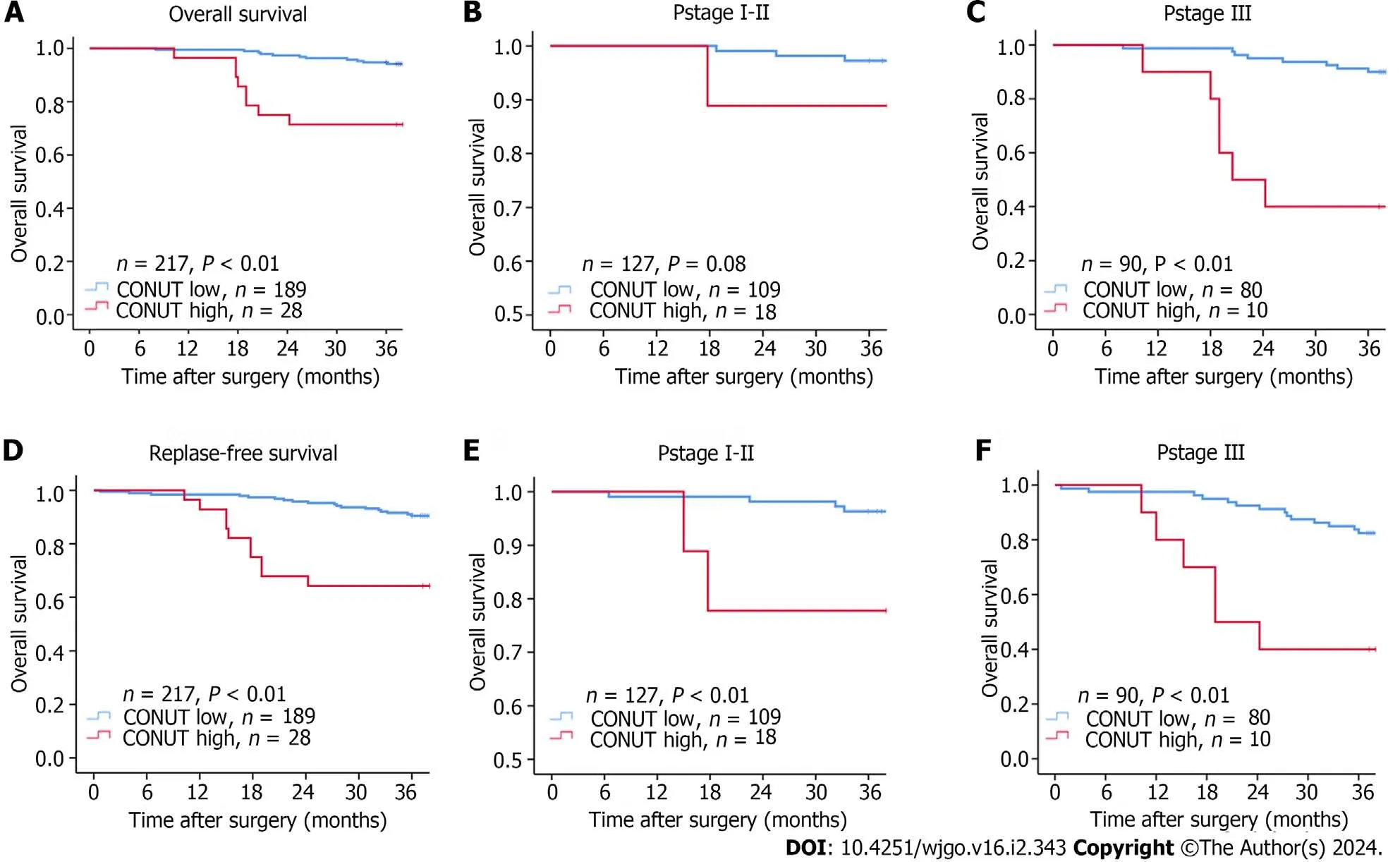
Figure 2 Kaplan-Meier curves for overall survival and replase-free survival. A and D: Controlling nutritional status high or low groups;B and E: pStageI-II patients;C and F: pStageⅢ patients.COUNT: Controlling nutritional status.
Cox regression analysis
Baseline factors without linear inter-correlations were included in univariate Cox regression analysis.Statistically significant factors were included in multivariate analysis which showed sarcopenia [hazard ratio (HR)=3.640,95% confidence interval (95%CI): 1.182-11.207,P=0.024],TNM tumor stage (ⅢvsⅡ,Ⅰ HR=4.396,95%CI: 1.534-12.598,P=0.006) and the CONUT score (HR=3.920,95%CI: 1.330-11.547,P=0.013) were associated with 3-year OS (Table 3).Sarcopenia (HR=4.122,95%CI: 1.678-10.125,P=0.002),TNM tumor stage (ⅢvsⅡ,Ⅰ HR=3.603,95%CI: 1.612-8.053,P=0.002),and the CONUT score (HR=2.992,95%CI: 1.241-7.212,P=0.015) were associated with 3-year RFS (Table 4).
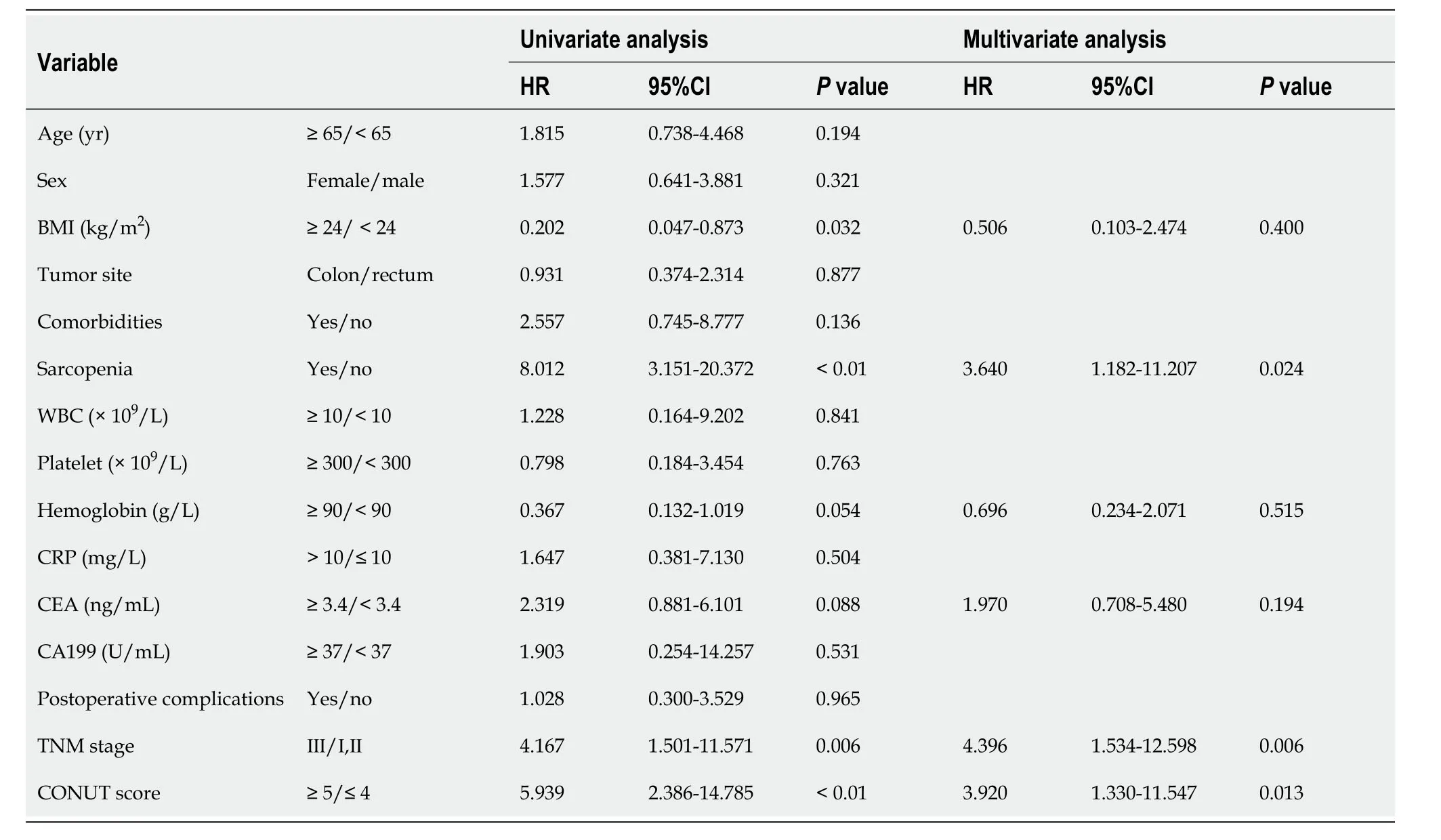
Table 3 Uni-and multi-variate analyses of factors associated with 3-year overall survival in patients with colorectal cancer
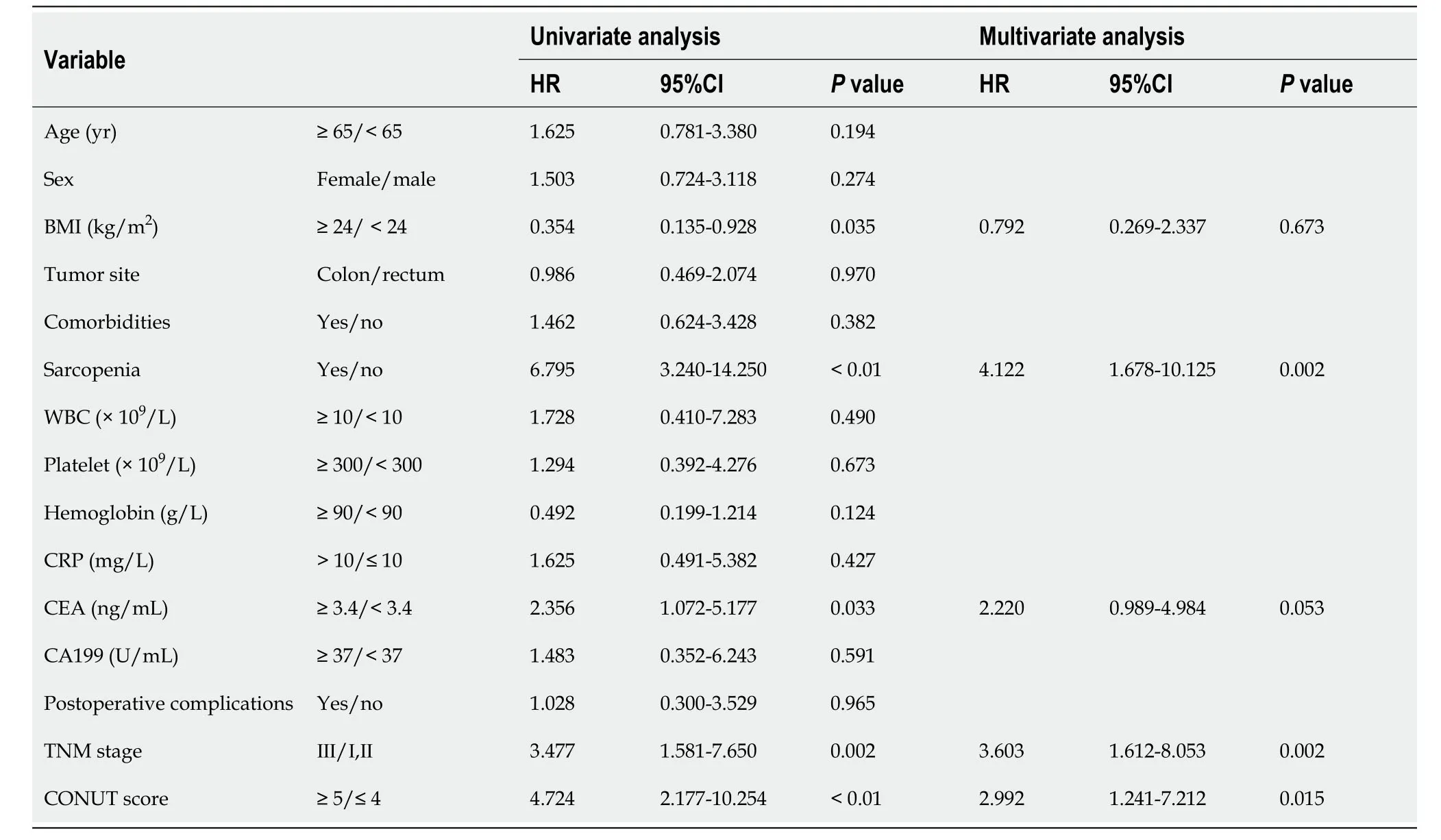
Table 4 Uni-and multi-variate analyses of factors associated with 3-year replase-free survival rates in patients with colorectal cancer
Comparison of the predictive accuracy between nutritional scores
Time-dependent ROCs were utilized to predict 3-year OS in overall patients.The area under the ROCs curve (AUC) ofthe CONUT,NLR,mGPS,and PNI were 0.728 (95%CI: 0.607-0.850,P< 0.01),0.585 (95%CI: 0.433-0.736,P=0.222),0.585 (95%CI: 0.445-0.726,P=0.219) and 0.414 (95%CI: 0.262-0.566,P=0.215),respectively (Figure 3).The CONUT score showed higher accuracy than NLR,mGPS,and PNI for predicting the 3-year OS in overall patients.The predictive accuracy was significantly different between CONUT and other scores (allP< 0.05) by the DeLong test.The best cutoff value of CONUT in predicting the 3-year OS was four as mentioned above.The CONUT score (AUC=0.662,95%CI: 0.546-0.778,P=0.005) was also more effective in predicting the 3-year RFS in general patients enrolled (Figure 3).

Figure 3 The time-dependent curves of controlling nutritional status,neutrophil-to-lymphocyte ratio,modified Glasgow prognostic score,and prognostic nutritional index.A: Predicting 3-year overall survival;B: Predicting 3-year replase-free survival.95%CI: 95% confidence interval;AUC: Area under the receiver operating characteristics curve;COUNT: Controlling nutritional status;NLR: Neutrophil-to-lymphocyte ratio;mGPS: Modified Glasgow prognostic score;PNI: Prognostic nutritional index.
Comparison and correlation between the CONUT score and SMI
Time-dependent ROCs were utilized to predict 3-year OS in all patients.The AUC of CONUT+TNM stage (AUC=0.803,95%CI: 0.703-0.904,P< 0.01) was higher than SMI+TNM stage (AUC=0.760,95%CI: 0.624-0.896,P< 0.01).When predicting the 3-year RFS,the AUC of CONUT+TNM stage (AUC=0.752,95%CI: 0.661-0.843,P< 0.01) was slightly lower than SMI+TNM stage (AUC=0.766,95%CI: 0.660-0.871,P< 0.01).Spearman correlation analysis was used to evaluate the correlations between the CONUT score and SMI.The CONUT score was negatively correlated with SMI (Figure 4).The relationships indicated that CONUT score could reflect the patient’s SMI to a certain extent and the predictive ability of postoperative prognosis of colorectal cancer is not weaker than SMI.
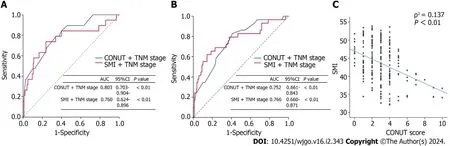
Figure 4 The time-dependent curves of controlling nutritional status+TNM stage and skeletal muscle mass index+TNM stage. A: Predicting 3-year overall survival;B: Predicting 3-year replase-free survival;C: The correlation between skeletal muscle mass index and controlling nutritional status.95%CI: 95% confidence interval;AUC: Area under the receiver operating characteristics curve;COUNT: Controlling nutritional status;SMI: Skeletal muscle mass index.
DlSCUSSlON
This study explored the associations between preoperative CONUT score and tumor prognosis among colorectal cancer patients.A pre-operative CONUT ≥ 5 was independently correlated with a 3.92-fold increased risk of poor OS and a 2.99-fold increased risk of poor RFS.By comparison,we found that the predictive power of the CONUT score was moreaccurate than that of other nutritional indexes.In addition,we observed a parallel relationship between the CONUT score and the patient’s skeletal muscle index,which strongly represents body protein reserve and nutritional state[21].Therefore,the CONUT score may serve as the optimal PNI to predict the long-term outcome after radical surgery for colorectal cancer.
Many studies have examined nutritional status and tumor prognosis in recent years.Low levels of skeletal muscle mass are often associated with malnutrition[22].Xiaoet al[9] found that preoperative levels of skeletal muscle could predict cancer prognosis.As reported,colorectal cancer patients with a pre-operative diagnosis of sarcopenia had a 1.1-1.2-fold higher incidence of postoperative complications and a 2-fold increased risk of death within 30 d after surgery than those without sarcopenia[6-9].Nonetheless,skeletal muscle measurement methods are not widely promoted because it is expensive,time and power consuming,carry radiation risks,and have other disadvantages.Therefore,a relatively convenient and safe early prediction indicator is needed.Although Golderet al[23] and Nozoeet al[24] found that mGPS,NLR,and PNI indexes could serve as prediction tools for prognosis in multiple cancers,the predictive power of these indicators remained unsatisfactory.In our study,the accuracy of the CONUT score was higher than that of mGPS,NLR,and PNI and showed satisfactory prediction performance.This objective,safe,simple,and easily accessible tool is more conducive to early and rapid prediction and has clinical application value.
As a nutritional status score,the effective role of the CONUT score has been clinically proven to evaluate nutrition[14].The ability of CONUT to predict the prognosis of colon cancer may be related to its three components.First,serum albumin is a biomarker for systemic inflammation.Tumor prognosis is highly correlated with an inflammation state.Excessive inflammatory activation affects the tumor microenvironment[25] and suppresses normal immune reactions[26].Second,Zhanget al[27],and Zhaoet al[28] demonstrated that colon cancer patients with reduced lymphocyte counts had worse prognoses than patients with normal lymphocyte counts.Lymphocytes,as immune cells,can recognize and kill tumor cells through humoral and cellular immunity pathways,thus playing a significant role in inhibiting tumor cell proliferation and metastasis[29].Third,cholesterol is mainly synthesized in the liver and exists in blood in the form of low-density lipoprotein (LDL).LDL receptor (LDLR) is expressed on the surface of both normal and tumor cells.Through the binding of LDLR to LDL,the serum LDL enters cells through endocytosis[30].Unlike normal tissues,LDLR does not limit intracellular cholesterol transportation through feedback regulation in cancer cells[31],allowing for unrestricted cholesterol transport into tumor cells to provide energy.Moreover,cancer cells can also use cholesterol metabolites to synthesize substances that promote their growth and development[32,33].Therefore,low serum cholesterol levels could be the result of an increased risk of cancer,indicating a poor prognosis.In conclusion,the ability of the CONUT score to predict prognosis may be due to its comprehensive reflection of the body's nutritional,inflammatory,and immune status,as well as tumor metabolism.
In addition,our study found a correlation between the CONUT score and skeletal muscle levels (R2=0.137,correlation coefficient -0.319,P< 0.01),possibly because both scores reflect the protein reserves in the body.Patients with cancer,especially those who undergo surgery procedures,could experience a larger demand for energy and protein intake than healthy people[34].Inadequate energy or protein intake would accelerate glycogenolysis leading to glycogen depletion,further promoting gluconeogenesis and leading to skeletal protein decomposition[35].Patients would be unable to tolerate surgery,delay recovery,and be even more prone to tumor recurrence,resulting in a poor prognosis when protein reserves are insufficient.This may be one of the factors contributing to the predictive power of CONUT scores.
The present study had several limitations.First,this study was a retrospective single-center study comprised of patients from the same region,and homogeneous in race.Second,the sample size was small,and the follow-up time was short.Last,the post-operative CONUT was not followed up and the nutritional status of patients could not be assessed dynamically.Therefore,prospective studies are warranted further to confirm the predictive significance of the CONUT score.
CONCLUSlON
To conclude,the CONUT score was significantly associated with the postoperative prognosis of colorectal cancer patients.Compared with other nutritional scores,the CONUT score could be an optimal PNI to predict the long-term outcome after radical surgery for colorectal cancer.In addition,the predictive power of the CONUT score may be related to skeletal muscle reserves.
ARTlCLE HlGHLlGHTS
Research background
At present,the nutritional status of cancer patients is closely related to the survival prognosis of patients.
Research motivation
The controlling nutritional status (CONUT) score can effectively evaluate the nutritional status of cancer patients,so we explored the relationship between CONUT score and prognosis of cancer patients.
Research objectives
To explore the relationship between CONUT score and postoperative prognosis of colorectal cancer patients.To study the prognostic performance of CONUT score in colorectal cancer patients and compare it with other nutritional scores.
Research methods
IBM SPSS Statistics for Windows,Version 26.0 (Armonk,NY: IBM Corp) was used for statistical analysis.The correlations between parameters were examined using Pearson's or Spearman's correlation coefficient when appropriate.Differences between groups were assessed byχ2test or analysis of variance.The Kaplan-Meier curve was used to analyze 3-year overall survival (OS) and 3-year relapse-free survival (RFS).Cox proportional hazards models were utilized to identify variables with significant independent associations with OS and RFS.The time-dependent receiver operating characteristic curve was used to evaluate the accuracy of prognosis prediction and was compared using the DeLong test between different scores.P< 0.05 was considered significantly different.
Research results
The CONUT score can effectively predict postoperative prognosis of patients with colorectal cancer,and its predictive function may be related to skeletal muscle reserve.The predictive effective of the CONUT score is not inferior to that of the other nutritional scores.
Research conclusions
The CONUT score was significantly associated with the postoperative prognosis of colorectal cancer patients.Compared with other nutritional scores,the CONUT score could be an optimal prognostic nutritional index to predict the long-term outcome after radical surgery for colorectal cancer.In addition,the predictive power of the CONUT score may be related to skeletal muscle reserves.
Research perspectives
Further improvement of the CONUT score makes it more effective in predicting the prognosis of cancer patients.
FOOTNOTES
Co-first authors:Li-Xiang Liu and Hao Wang.
Co-corresponding authors:Ji Miao and Wen-Xian Guan.
Author contributions:Liu LX,Wang H,Gao B,Ding C,Miao J and Guan WX designed the research;Liu LX,Yuan QG,Zhou SZ and Xu TT,performed the research;Ding C and Gao B contributed analytic tools;Liu LX,Wang H,Gao B and Ding C analyzed the data;Liu LX,Wang H,Gao B,Miao J and Guan WX wrote the paper;all authors were involved in the critical review of the results and have contributed to,read,and approved the final manuscript.Liu LX and Wang H contributed equally to this work as co-first authors.Guan WX and Miao J contributed equally to this work as co-corresponding authors.There are three reasons for designating Liu LX and Wang H as co-first authors and Guan WX and Miao J as co-corresponding authors.First,the research was performed as a collaborative effort,and the designation of co-corresponding authorship accurately reflects the distribution of responsibilities and burdens associated with the time and effort required to complete the study and the resultant paper.This also ensures effective communication and management of post-submission matters,ultimately enhancing the paper's quality and reliability.Second,the overall research team encompassed authors with a variety of expertise and skills from different fields,and the designation of co-corresponding authors best reflects this diversity.This also promotes the most comprehensive and in-depth examination of the research topic,ultimately enriching readers' understanding by offering various expert perspectives.Third,they put equal effort into the whole research process.The choice of these researchers as co-first authors/co-corresponding authors acknowledges and respects this equal contribution,while recognizing the spirit of teamwork and collaboration of this study.In summary,we believe that designating Liu LX and Wang H as co-first authors and Guan WX and Miao J as co-corresponding authors of is fitting for our manuscript as it accurately reflects our team's collaborative spirit,equal contributions,and diversity.
Supported byClinical Trials from the Affiliated Drum Tower Hospital,Medical School of Nanjing University,2022-LCYJ-PY-17;CIMF -CSPEN Project,Z-2017-24-2211;and Project of Chinese Hospital Reform and Development Institute,Nanjing University and Aid project of Nanjing Drum Tower Hospital Health,Education &Research Foundation,NDYG2022090.
lnstitutional review board statement:The entire process followed the ethical standards of the Declaration of Helsinki.This study was approved by the ethics committee of Nanjing Drum Tower Hospital and General Hospital of Eastern Theater Command,and was performed after informed consent was.
lnformed consent statement:All study participants,or their legal guardian,provided informed written consent prior to study enrollment.
Conflict-of-interest statement:All the Authors have no conflict of interest related to the manuscript.
Data sharing statement:The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
STROBE statement:The authors have read the STROBE Statement—checklist of items,and the manuscript was prepared and revised according to the STROBE Statement—checklist of items.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Wen-Xian Guan 0009-0000-4778-703X.
S-Editor:Lin C
L-Editor:A
P-Editor:Cai YX
 World Journal of Gastrointestinal Oncology2024年2期
World Journal of Gastrointestinal Oncology2024年2期
- World Journal of Gastrointestinal Oncology的其它文章
- Does enhanced recovery after surgery programs improve clinical outcomes in liver cancer surgery?
- Cardiotoxicity induced by fluoropyrimidine drugs in the treatment of gastrointestinal tumors
- Effect of screening colonoscopy frequency on colorectal cancer mortality in patients with a family history of colorectal cancer
- Tumour response following preoperative chemotherapy is affected by body mass index in patients with colorectal liver metastases
- Expression of cyclin-dependent kinase 9 is positively correlated with the autophagy level in colon cancer
- Progress in the treatment of advanced hepatocellular carcinoma with immune combination therapy