
Different serum levels of lgG and complements and recurrence rates in IgG4-positive and negative lacrimal gland benign lymphoepithelial lesion
2023-06-17 06:52:18RuiLiuNanWangJinJinWangJingLiXinGeJingXueZhangJianMinMa
Rui Liu, Nan Wang, Jin-Jin Wang, Jing Li, Xin Ge, Jing-Xue Zhang, Jian-Min Ma
Beijing Ophthalmology and Visual Sciences Key Laboratory,Beijing Tongren Eye Center, Beijing Tongren Hospital, Capital Medical University, Beijing 100730, China
Abstract● AIM: To analyze the differences in immune indicators and prognosis between IgG4-positive and negative lacrimal gland benign lymphoepithelial lesion (LGBLEL).
● KEYWORDS: benign lymphoepithelial lesion; lacrimal gland; IgG4; complement; prognosis
INTRODUCTION
IgG4-related disease (IgG4-RD) is an immune-mediated systemic disease characterized by diffuse infiltration of plasma cells expressing positive IgG4, which results in swelling of the diseased tissue accompanied by a significant increase in serum IgG4[1].IgG4-RD previously referred to as “Mikulicz’s disease”and benign lymphoepithelial lesion(BLEL) by some researchers[2-3].IgG4-related ophthalmic disease (IgG4-ROD) is a subtype of IgG4-RD and can involve all orbital tissues, the most common of which is lacrimal gland[4].The incidence of IgG4-ROD accounts for 4%-34% of IgG4-RD and 20%-25% of all instances of orbital lymphoproliferative disease[5-6].
The diagnostic criteria for IgG4-ROD: 1) Imaging findings show enlargement of lacrimal gland, trigeminal nerve or extraocular muscle as well as masses, enlargement or hypertrophic lesions in various ophthalmic tissues; 2)Histopathological examination shows marked lymphocyte and plasmacyte infiltration, and sometimes fibrosis.histopathological findings >10 IgG4+ plasma cells per high power field (×400) and an ⅠgG4+/ⅠgG+ cell ratio >40%; 3)Serum ⅠgG4 was elevated (≥135 mg/dL)[7].However, we found that some untreated cases had similar histopathological manifestations as IgG4-ROD, but the IgG4 expression did not meet the diagnostic criteria of IgG4-ROD through clinical observation.These cases were not classified as IgG4-ROD.Therefore, we proposed to name these cases as lacrimal gland benign lymphoepithelial lesion (LGBLEL) according to the pathological manifestations and involved site, and then divided it into IgG4-positive LGBLEL and IgG4-negative LGBLEL according to the IgG4-ROD diagnostic criteria.So far, we have carried out a series of studies on LGBLEL, and the name has gradually been recognized and accepted[8-10].Symptoms of LGBLEL include swelling of the eyelids and diffuse enlargement of the lacrimal glands.The typical pathological manifestations of LGBLEL are diffuse infiltration of lymphocytes and plasma cells in lacrimal gland tissue, atrophy and disappearance of glands, and hyperplasia of fibrous tissue[9-10].Therefore, this study comparatively analyzed the clinical characteristics, laboratory indicators, prognosis, and prognostic influencing factors of IgG4-positive and negative LGBLEL to identify the clinical indicators with differential diagnostic significance.
SUBJECTS AND METHODS
Ethical ApprovalWritten informed consent was obtained from all patients, and the study was approved by the Institutional Review Board (TRECKY2019-093) and conducted according to the tenets of the Declaration of Helsinki.
General Information and MethodsThis was a singlecenter retrospective clinical study.The medical records of 146 LGBLEL confirmed by pathology from June 2011 to June 2019 were collected from the medical records database, by professional ophthalmologists.The number of IgG4 positive expression was counted and confirmed by two professional pathologists.The 105 cases were IgG4-positive LGBLEL and 41 cases were IgG4-negative LGBLEL.Inclusion criteria for IgG4-positve group were as follows: 1) lacrimal gland enlargement, histopathological manifestations of extensive infiltration of lymphocytes and plasma cells, and hyperplasia of fibrous connective tissue; 2) histopathological findings >10ⅠgG4+ plasma cells per high power field and an ⅠgG4+/ⅠgG+cell ratio >40%; 3) a serum IgG4 concentration >135 mg/dL.Inclusion criteria for patients with IgG4-negative group were 1)untreated cases, but not IgG4-ROD cases with negative IgG4-expression after glucocorticoid treatment; 2) lacrimal gland enlargement, histopathological manifestations of extensive infiltration of lymphocytes and plasma cells, and hyperplasia of fibrous connective tissue; 3) histopathological findings ≤10ⅠgG4+ plasma cells per high power field and an ⅠgG4+/ⅠgG+cell ratio ≤40%; 4) a serum ⅠgG4 concentration ≤135 mg/dL.Exclusion criteria were as follows: 1) serum and staining data for IgG4 were unavailable; or 2) other lacrimal gland diseases and tumors.Participants with LGBLEL were required to satisfy the first two or more inclusion criteria.
Clinical DataThe clinical data of the IgG4-positive and negative LGBLEL were collected, including age, gender,affected eye, past medical history (postoperative glucocorticoid history, operation history, sinusitis, asthma, lymph node swelling, and other immune system diseases), clinical manifestations (including main symptoms and simultaneous symptoms), imaging characteristics, disease course, and immunohistochemical indicators.All patients had complete medical history, and the imaging examination included magnetic resonance imaging or computed tomography.The affected locations (including the lacrimal gland, orbital fat,extraocular muscle, optic nerve, eyelid, and conjunctiva)were recorded according to the results of magnetic resonance imaging (MRI) or computed tomography (CT).Course of disease referred to the duration of clinical symptoms.
Laboratory DataPeripheral venous blood samples of IgG4-positive and negative LGBLEL were collected using the immunoscattering turbidimetry to test for related indicators,including complement 3 (C3), C4, and rheumatoid factor(RF), C-reactive protein (CRP), anti-streptolysin O (ASO),immunoglobulin A (IgA), IgM, and IgG and its subtypes (IgG1,IgG2, IgG3, and IgG4).The laboratory indicators of the two groups were compared and analyzed.
Treatment and PrognosisAll patients were treated with partial surgical excision and glucocorticoid therapy.According to the volume of the lesion, either a subarcuate skin incision or a double eyelid skin incision on the anterior orbital temporal eyebrow was selected for the surgical approach.The subcutaneous tissue was separated to reach the orbital margin, and the orbital partition was cut into the orbit.The lesion was partially removed and histopathological examination was conducted.The patients were given glucocorticoids 80-120 mg/d for 3d after the operation, which was then changed to methylprednisolone tablets 24-28 mg/d.Tapering 4 mg/d every 1-2wk according to the patient’s condition until the withdrawal of the drug.The course of treatment was 1.5-3mo.
The effective follow-up time was from the definitive diagnosis of the first biopsy to the death of the patient or June 2020.The following observation indicators were collected during followup.1) General conditions: vision, eyelid swelling, proptosis,and others.2) Ⅰmaging findings: in order to objectively evaluate the therapeutic effect and observe recurrence, preoperative and postoperative MRI/CT examination was necessary.The specific time points were pre-operation, half a year after operation, 1-3y after operation, and 5y after operation.The criteria for recurrence include eyelid swelling and the MRI/CT of orbit showing lacrimal gland enlargement.
Statistical AnalysisGraphpad Prism 8.0 and SPSS 25.0 software were used for analysis.Measurement data were tested by one-sample Kolmogorov-Smirnov test.Mean±standard deviation and independent samplet-test were used to test the data of two groups consistent with normal distribution.Median and non-parametric rank sum test were used for data that did not conform to normal distribution.The Chi-square test or Fisher’s exact test were used for counting data.Survival curvesfor recurrence were created using the Kaplan-Meier method and compared between groups using log-rank tests.The influencing factors were analyzed by binary logistic regression analysis.APvalue <0.05 was considered statistically significant.
RESULTS
Clinical Characteristics of IgG4-positive and IgG4-negative LGBLELA total of 146 patients with biopsyproven LGBLEL were ultimately enrolled in the study, and 105 (71.9%) patients were placed in the IgG4-positive group based on pathological analysis.The results (Table 1) showed that the male-female ratio of the IgG4-positive group was 1:2.8,the ratio in the IgG4-negative group was 1:4.9 (P=0.283).The mean age of IgG4-positive group was 50.10±14.23 years old,and that of the IgG4-negative group was 44.76±11.43 years old(P=0.033).There were 14 cases of right eye lesions, 24 casesof left eye lesions, and 67 cases of binocular lesions in the IgG4-positive group, and 11 cases of right eye lesions, 12 cases of left eye lesions, and 18 cases of binocular lesions in the IgG4-negative group (P=0.059).Preoperative glucocorticoid therapy in 24 cases, 3 cases with operation history, 3 cases of asthma, 27 cases of sinusitis, 4 cases with history of lymph node enlargement, and 3 cases with other immune system diseases in the IgG4-positive group.There were 5 cases of sinusitis in the IgG4-negative group.
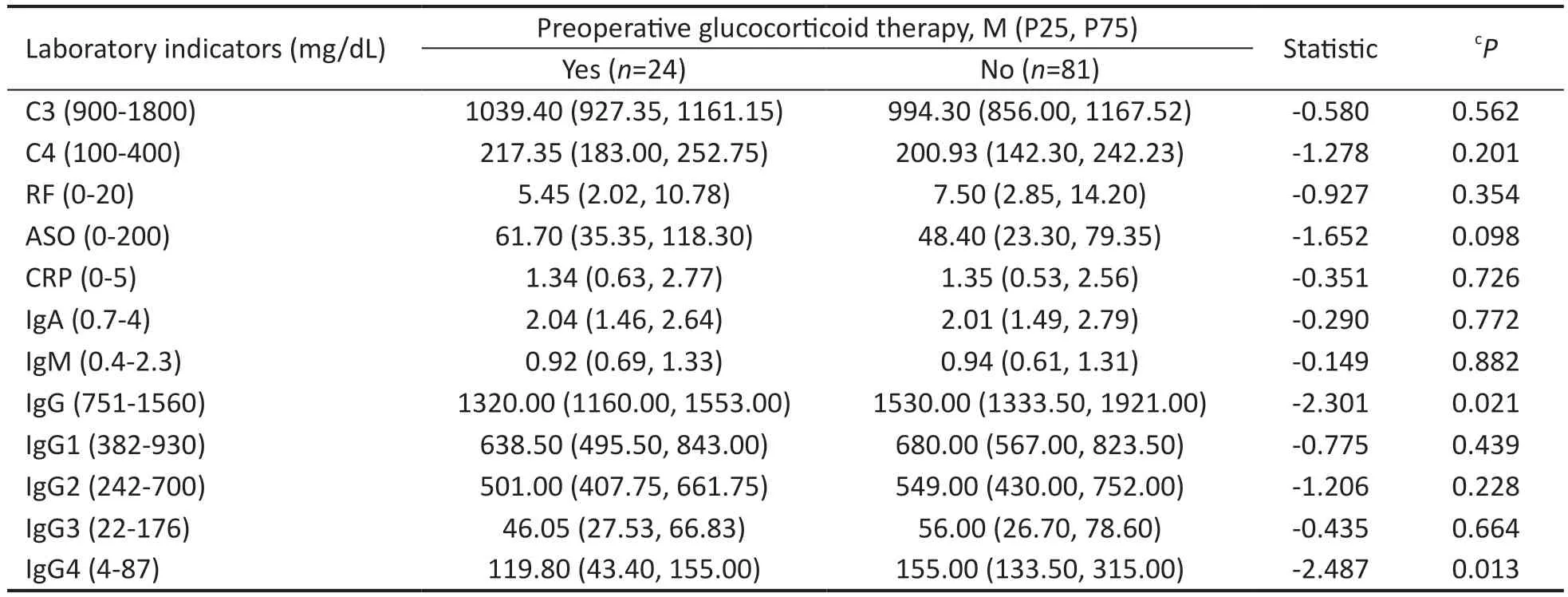
Table 2 Laboratory indicators in IgG4-positive LGBLEL with or without preoperative glucocorticoid therapy
The main clinical manifestations of the IgG4-positive group were eyelid swelling in 96 cases, proptosis in 2 cases, and eyelid mass in 7 cases.The main clinical manifestations of the IgG4-negative group were eyelid swelling in 33 cases,eyelid mass in 2 cases, and proptosis in 6 cases.Eyelid swelling was the main clinical manifestation in both groups.There were no statistical differences in main and simultaneous symptoms between the two groups (P>0.05).The 98% of the patients underwent MRI examination and 2% underwent CT examination.MRI/CT examination showed signs of lacrimal gland enlargement and eyelid swelling in both two groups.IgG4-positive group mainly manifested as sinus mucosa thickening (25.7%), extraocular muscle thickening(15.2%), and nerve (trigeminal, frontal nerve, maxillary nerve or mandibular nerve) thickening (3.8%), while IgG4-negative group mainly manifested as sinus mucosa thickening(12.2%), and extraocular muscle thickening (14.6%).There were no statistically significant differences in imaging findings between the two groups (P>0.05).The mean course of disease was 18.70±19.16mo in the IgG4-positive group and 21.22±25.87mo in the IgG4-negative group (P>0.05).
Serum Levels of IgG and Complements in IgG4-positive and IgG4-negative LGBLELThe serum levels of C3, C4,RF, ASO, CRP, IgA, IgM, IgG, IgG1, IgG2, IgG3, and IgG4 were analyzed (Table 1).There was no significant statistical difference in RF, ⅠgM, ASO, CRP, ⅠgA, and IgG3 between the two groups (allP>0.05).And the serum C3 and C4 was lower in IgG4-positive group (P=0.005, 0.002), while the serum IgG,IgG2 and IgG4 was higher in IgG4-positive group (P=0.000,0.008, 0.000).
As was shown in Table 2, compared with IgG4-positive LGBLEL group without preoperative glucocorticoid therapy history, the IgG and IgG4 in IgG4-positive LGBLEL group with preoperative glucocorticoid therapy history were lower(P=0.021, 0.013), while the C3, C4, IgA, IgM, RF, ASO, CRP,IgG1, IgG2, and IgG3 had no difference between the two groups (allP>0.05).
Prognosis in IgG4-positive and IgG4-negative LGBLELAll 146 patients underwent surgical resection combined with glucocorticoid therapy (Table 1).The average follow-up time of the IgG4-positive group was 4.10±1.91y, and 77 cases had no recurrence, 21 cases had recurrence, 6 cases were lost to follow-up, and 1 patient died naturally.The average follow-up time of the IgG4-negative group was 5.09±2.45y, and 35 cases had no recurrence, 3 cases had recurrence and 3 cases were lost to follow-up.After excluding the loss to follow-up and natural death cases, the recurrence-free cumulative percentages at 5y were 81.85% and 83.46% in IgG4-positive and negative LGBLEL respectively (P=0.216; Figure 1).
Factors Influencing the Recurrence of LGBLELBinary logistic regression analysis was performed on 136 patients with LGBLEL.Group (IgG4-positive and negative), gender,age, laterality, operation history, asthma, sinusitis, lymph node enlargement, other immune system disease history, nerve thickening, extraocular muscle thickening and laboratory indicators were analyzed in Table 3.The results showed that serum C4, and ⅠgG1 were factors influencing the recurrence of LGBLEL (P=0.017,P=0.048, respectively).
Binary logistic regression analysis was performed on 98patients with IgG4-positive LGBLEL.The results showed that preoperative glucocorticoid therapy history, serum C4, IgG1,and ⅠgG2 were factors influencing the recurrence of LGBLEL(P=0.002, 0.008, 0.046, 0.009, respectively; Table 4).

Table 3 Analysis of factors influencing recurrence of 136 patients with LGBLEL
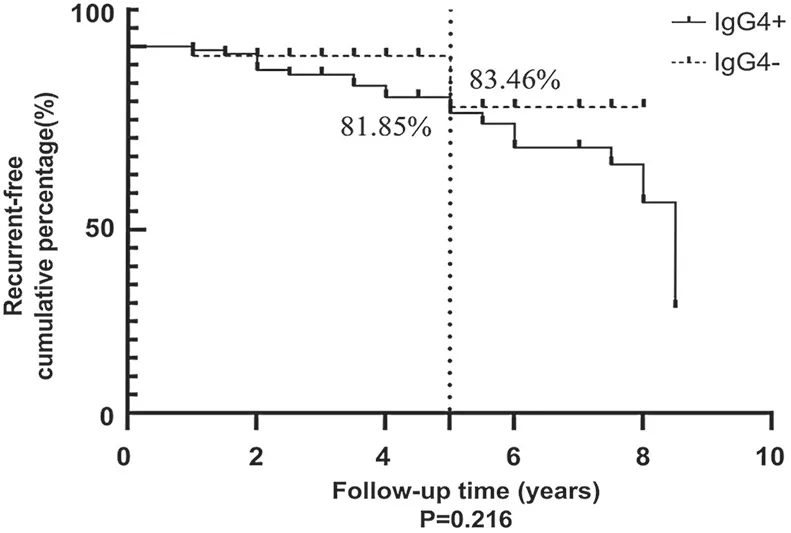
Figure 1 Comparative analysis of prognosis between IgG4-positive and negative LGBLEL The recurrence-free cumulative percentages at 5y in IgG4-positive and negative dacryoadenitis was 81.85% and 83.46%, respectively (P=0.216).LGBLEL: Lacrimal gland benign lymphoepithelial lesion.
DISCUSSION
In recent years, the prevalence of IgG4-ROD has been increasing gradually, which has attracted extensive attention from ophthalmologists.According to a study in China, the incidence of IgG4-ROD accounted for 60% of idiopathic orbital inflammatory disease[11].Other studies showed that the incidence of IgG4-ROD in Japan is about 61.5%, 52.4% in the United States, and 45.8% in South Korea[12-14].The results of this study showed that LGBLEL was more common in female,both in IgG4-positive and negative groups.The lacrimal gland inflammation could be influenced by the level of estrogen.Jianget al[15]found that estrogen and its receptor might inhibit the inflammatory response in rat colon tissues, suggesting that a decrease in estrogen may be one of the relevant factors in the occurrence of inflammation.In addition, there was a significantly difference in age between the two groups, and the mean age of IgG4-positive LGBLEL was older.This may indicate that levels of estrogen in female patients gradually decline with age, increasing the incidence of LGBLEL.
IgG4-ROD may be associated with immune system diseases,such as allergic rhinitis, asthma, lymph node enlargement, and Sj?gren’s syndrome[16-17].In our study, LGBLEL had a history of immune system disease, among which allergic rhinitis,sinusitis, and lymph node enlargement were common.The imaging findings were primarily lacrimal gland enlargement,accompanied by sinus mucosa, extraocular muscle, and ocular nerve thickening.In this study, 15.2% of patients in IgGpositive group presented with extraocular muscle thickening and 3.8% of patients presented with ocular nerve thickening,while 14.6% of IgG4-negative group presented with ocular muscle thickening and no case presented with ocular nerve thickening, which showed no significant difference between the two groups.These results may suggest that extraocular muscle and ocular nerve thickening are not specific indicators to differentiate ⅠgG4-positive and negative LGBLEL.
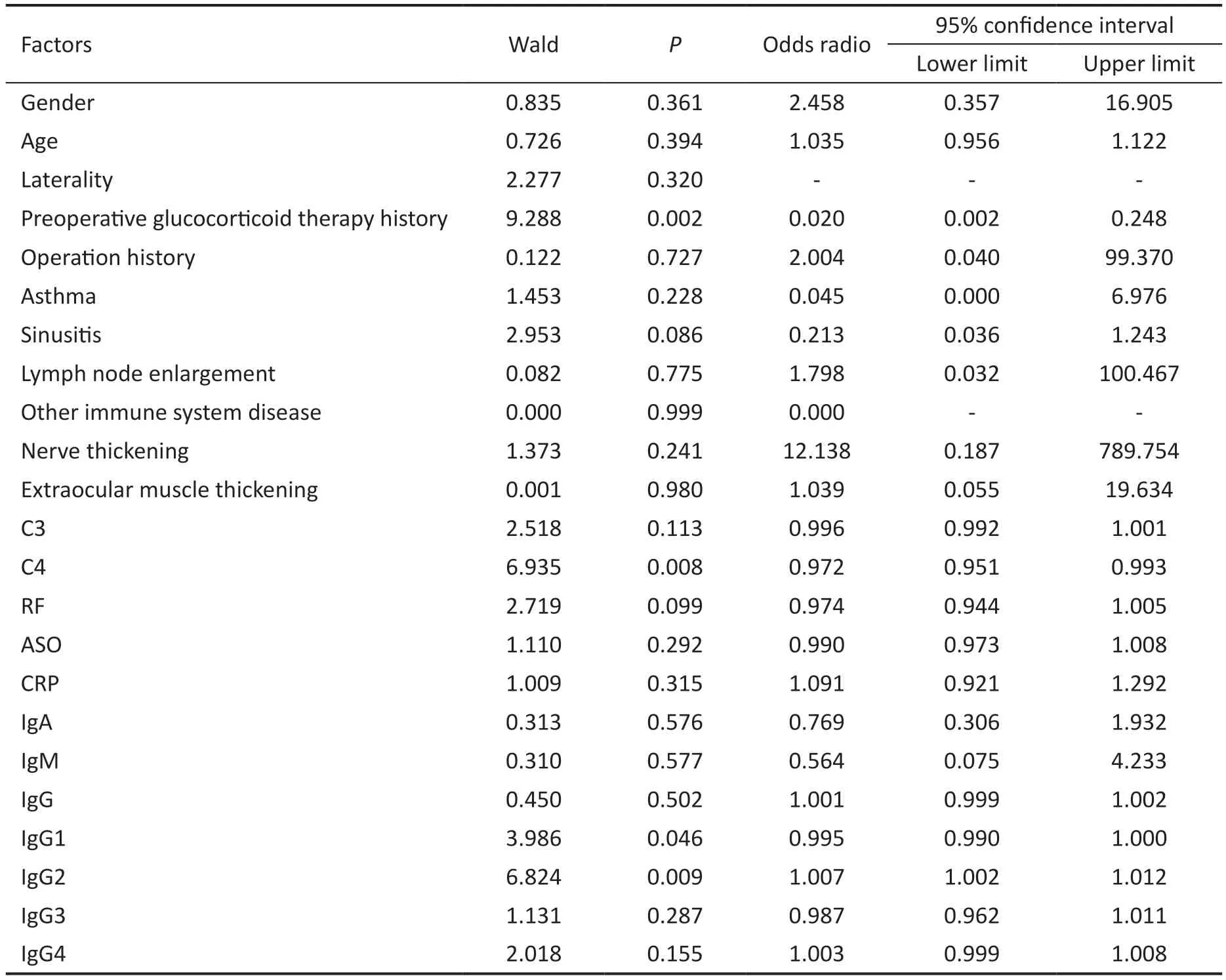
Table 4 Analysis of factors influencing recurrence of 98 patients with IgG4-positive LGBLEL
Immunoglobulin has the functions of activating complement,absorbing cells, and extracellular killing.Complement is a type of protein that mediates autoimmune and inflammatory responses.Studies have found that IgG can activate C3 through the classical pathway and IgG4 can activate C3 through the bypass pathway to play an immunomodulation role, while the complement system can play an anti-infection role, regulate inflammatory response and maintain immune homeostasis through the massive consumption of C3 and C4[18-20].Some studies had found that the serum C3, C4, IgG1,ⅠgG2, ⅠgG3, ⅠgE, and CRP were significant for the diagnosis of IgG4-ROD[21-22].Chenet al[11]found that compared with other orbital idiopathic inflammatory disease, serum C3 ofⅠgG4-ROD were significantly decreased.Ⅰn our study, relevant immune indicators were systematically analyzed, and the results showed that C3, C4, IgG, IgG2, and IgG4 were great significance for the differentiation between ⅠgG4-positive and negative LGBLEL, while there was no significant difference of RF, ASO, CRP, IgA, IgM, IgG1 and IgG3.Compared with IgG4-negative LGBLEL, the levels of C3 and C4 were decreased, while those of IgG, IgG2, and IgG4 were increased in the ⅠgG4-positive group, which had differential significance.And preoperative glucocorticoid therapy could reduce IgG and IgG4 expression in IgG4-positive LGBLEL.
At present, partial surgical resection combined with glucocorticoid therapy is the main treatment for LGBLEL,and more patients still relapse after treatment.Chenet al[11]reported that the recurrence rates of IgG4-positive and IgG4-negative idiopathic orbital inflammatory disease were 32.2%and 19.1%, respectively.A French study showed that about 2/3 of IgG4-ROD cases relapsed[21], and Suimonet al[23]found that the recurrence rate was about 33.3%.Owing to differences in race, sample size, follow-up time, and sensitivity to glucocorticoids, the recurrence rate of ⅠgG4-ROD differed across some research centers, but mostly ranged from 18% to 58%[24-26].In our study, the recurrence rate of 5-year in IgG4-positive and negative LGBLEL patients was 18.15% and 16.54%, respectively.There was no significant difference in recurrence rates between the two groups.
All patients were treated by the partial surgical resection combined with glucocorticoid therapy.The prognostic factors of LGBLEL were statistically analyzed, and lost to follow-up and natural death cases were excluded.The results showed that serum C4, and ⅠgG2 were the factors affecting the recurrence of LGBLEL.Studies have found that C3 and C4 levels are significantly decreased during active inflammation, while ⅠgG and its subtypes are increased[11,21-23].In patients with active IgG4-ROD, a large number of immune complexes will be produced, leading to elevated levels of IgG and its subtypes,thus activating the complement system.However, C3 and C4 can be consumed through classical and bypass pathways to eliminate immune complexes, leading to a decreased level of C3 and C4.Therefore, patients with increased C4 and decreased IgG2 may have a lower risk of recurrence.
Kubotaet al[27]found that extraocular muscle and trigeminal nerve thickening could affect the therapeutic effect of glucocorticoids and the prognosis of IgG4-ROD.Previous studies had shown that serum IgG4, RF, and male gender were risk factors for recurrence of IgG4-ROD treated with glucocorticoid therapy[28-30].Liuet al[31]found that IgG4-ROD symptom duration was significantly positively correlated with relapse rate.Our study showed that gender, extraocular muscle thickening, nerve thickening, sinusitis, IgG4 and RF were not risk factors for recurrence of LGBLEL.And the preoperative glucocorticoid therapy history, serum C4, IgG1 and IgG2 were the factors affecting the recurrence of ⅠgG4-positive LGBLEL.Chouet al[32]believed that serum IgG4 was a response to inflammatory stimulus, more likely a consequence than a cause of the disease, and patients with IgG4-ROD had a favorable outcome, regardless of their serologic status in the long-term.Serum ⅠgG4 was not found to be a factor affecting LGBLEL recurrence in this study, which was inconsistent with previous results indicating that ⅠgG4 was an influencing factor for ⅠgG4-ROD recurrence.This may be influenced by factors such as different study subjects, treatment modalities and responses to glucocorticoid therapy.
There were some shortcomings in this study.First, this was a retrospective study.Second, there were no standardized criteria for treatment, and the dose of glucocorticoid depended on the disease condition, which had an impact on the prognosis of LGBLEL.In addition, the follow-up time also influenced prognosis of LGBLEL.Some LGBLEL with IgG4 positive expression were treated with glucocorticoid before operation, which had a certain effect on the expression of immunological indexes.In summary, this study analyzed the clinical characteristics,immune indicators, and prognosis of IgG4-positive and negative LGBLEL.C3 and C4 was decreased, while IgG,IgG2, and IgG4 was increased, which had significance for distinguishing between IgG4-positive and negative LGBLEL.Serum C4, IgG1 and IgG2 could influence the recurrence of LGBLEL, and IgG4 was not a major prognostic factor.
ACKNOWLEDGEMENTS
Authors’contributions:Liu R, analyzed and wrote the manuscript; Wang N, Wang JJ, and Li J collected the data; Ma JM, Ge X, and Zhang JX read and reviewed the manuscript.All authors read and approved the final manuscript.
Foundations:Supported by Beijing Hospitals Authority’Ascent Plan (No.DFL20190201); Natural Science Foundation of Beijing (No.7222025); Beijing Science and Technology Rising Star Program-Cross-cooperation (No.20220484218).
Conflicts of Interest:Liu R, None; Wang N, None; Wang JJ, None; Li J, None; Ge X, None; Zhang JX, None; Ma JM, None.
 International Journal of Ophthalmology2023年6期
International Journal of Ophthalmology2023年6期
- International Journal of Ophthalmology的其它文章
- Role of 7-methylxanthine in myopia prevention and control: a mini-review
- How internal limiting membrane peeling revolutionized macular surgery in the last three decades
- Photoreceptor changes in Leber hereditary optic neuropathy with m.G11778A mutation
- Efficacy and safety of subthreshold micropulse laser in the treatment of acute central serous chorioretinopathy
- Efficacy of ripasudil in reducing intraocular pressure and medication score for ocular hypertension with inflammation and corticosteroid
- Subconjunctival conbercept for the treatment of corneal neovascularization